
Abstract
This study investigated the feasibility of a coach-led digital health platform for mitigating burnout and enhancing wellbeing among hospital workers. After an initial online anonymous needs assessment, consenting hospital workers (n=24) were randomly stratified into intervention and waitlist control groups for 12 weeks. Feasibility was examined using the first three elements of the RE-AIM Framework: Reach, Effectiveness, and Adoption. Secondary outcomes examined changes in burnout and wellbeing, and semi-structured interviews were conducted with participants post-intervention. Results showed improvements in wellbeing and reduced burnout in the intervention group. The platform was well accepted, though attrition rates were high. Further research with larger samples is needed to enhance recruitment and assess broader impact.
Introduction
Recent research has highlighted a need to protect the physical and mental health of frontline hospital workers (World Health Organisation, 2020; Burke et al., 2021; Xiang et al., 2019; Søvold et al., 2021; O’Brien et al., 2022). Healthy hospital workers play a fundamental role in creating healthcare services that are effective, efficient and compassionate. Despite this, hospital workers often report experiencing poor wellbeing, high levels of work-related stress and burnout (Johnson et al., 2018; O’Connor, Hall & Johnson, 2020; Dunne et al., 2019; Lynch et al., 2018). Before the COVID-19 pandemic, a survey of 1,759 doctors based in Ireland, revealed that 35/ experienced psychological distress related to high levels of stress and anxiety (Hayes et al., 2017). In the same period, Irish medical interns (US residents equivalent) reported high levels of burnout and stress, with 37/ of those assessed experiencing psychological distress, including emotional exhaustion (Hayes et al., 2017; Hannan et al., 2018). These levels of stress and burnout were exacerbated during the COVID-19 pandemic and across all healthcare sectors (O’Brien et al., 2022; Bohlken et al., 2020; Zhou et al., 2022; Denning et al., 2021; Wilbiks et al., 2021; Müller et al., 2023), resulting in increased burnout, anxiety and PTSD among hospital workers (Chirico et al., 2021; Nishimura et al., 2021). This has heightened the need to implement approaches dedicated to improving and maintaining hospital worker wellbeing (Søvold et al., 2021; Burton, 2010; Rehder, Adair & Sexton, 2021; National Academies of Sciences, 2019).
Although the Irish Health Service Executive (HSE) has developed support structures for hospital worker and healthcare staff in general, research shows that hospital workers are less likely to engage in supports that are linked to their employer (Hayes et al., 2017; Harrison, 2008), and are more likely to use independent support platforms (Ah-kee & Asif Khan, 2015; Shenouda, Davies & Haq, 2018; Payne, Wharrad & Watts, 2012). Important research on hospital workers coping with the psychological effects of disaster relief has shown that resilience (defined as positive adaptation despite adversity), can be enhanced and post-traumatic stress can be attenuated by adopting three strategies: (i) focused specific preparatory training; (ii) high levels of social support and (iii) encouraging proactive coping styles (Müller et al., 2023; Brooks et al., 2020). The interventions used in the current project are particularly relevant to the latter two of these strategies.
Positive Health Coaching and Positive Health Science
In the current study, we discuss the application of positive health coaching, delivered via a digital health platform (smartphone app) that rests on Positive Health Science. Positive health coaching focuses on an individual’s strengths, resources and potential for growth, rather than weaknesses or problems. This type of coaching can occur face-to-face or via digital communication platforms (phone, text and video). Emerging Positive Health Science (Burke et al., 2023) currently draws on the combined fields of positive psychology (Seligman, 2000), lifestyle medicine (Bodai et al., 2018) and health psychology. Positive Health Coaching integrates positive psychology, lifestyle medicine and behaviour change theory into an active coaching conversation to facilitate a holistic approach to health and wellbeing changes. It also adopts a dialogical approach, balancing facilitative and directive conversational interventions. This dialogical approach aims to balance asking and telling; providing a person-centred, facilitative environment while simultaneously allowing the coach to share evidence-based advice, information and guidelines (van Nieuwerburgh & Knight, 2023).
Coach Connect Project
The COVID-19 pandemic triggered a shift towards virtual coaching, which benefits service users by being more affordable and easily accessible without having to physically move geographical locations (Stoyanov, 2021; van Coller-Peter & Manzini, 2020; Borghouts et al., 2021). Despite this, there is limited knowledge of how human coaching and technology can work together to deliver more effective and efficient coaching services to users and allow for the scalability of online interventions. The majority of studies relate to clinical, athletic or healthcare settings, focusing on physical activity, nutrition, and chronic conditions (Ribbers & Waringa, 2015). Within a healthcare setting, patients have reported that their virtual coach supported and motivated them to become more mindful and reported a perceived reduction in anxiety, depression, and stress symptoms (Bassi et al., 2022). However, there are mixed findings concerning the effectiveness of using human coaches on digital platforms (Gao, Galley & Li, 2019; Sasaki, Ihaya & Yamada, 2017; Araujo, 2018; Lovejoy, 2018). Examining the feasibility of online coaching for hospital workers is vital, given that it offers a less time-consuming and more convenient, potentially scalable alternative to in-person interventions (Tement et al., 2021).
The current study aims to investigate the feasibility of delivering positive health coaching, using a positive health sciences approach, to hospital workers via a smartphone app and digital health platform. The primary outcome of this study was to evaluate the reach, adoption and efficacy of the coach-led digital platform, as part of the RE-AIM framework for examining the feasibility of pilot studies (Glasgow, Vogt & Boles, 1999). The secondary outcomes examined changes in wellbeing, burnout and perceived lifestyle medicine-based vital signs (sleep, daily exercise, eating well, stress management, cultivating relationships and avoiding risky substances such as tobacco and alcohol) over 12 weeks among hospital worker research participants.
Materials and Methods
Design
Coach Connect is a feasibility study incorporating a mixed-methods design, based on the
Participants
Participants were not involved in formulating the study questions or the outcome measures. An anonymous needs assessment survey was conducted using secure Microsoft Forms survey links developed by the (Omitted per double-blind reviewing), and delivered by email through human resources departments and department heads across (hospitals omitted per double-blind reviewing). The results of this survey were used to prepare online support content for the Coach Connect smartphone app used by the online coach and study participants. The survey also invited respondents to declare interest in a subsequent online pilot project (Coach Connect). Twenty-six participants were recruited from a sample of 119 hospital workers who completed the needs assessment survey between May and August 2021. Aggregate summaries of the results of the Coach Connect project were emailed to all participants in September 2022.
Randomisation and sequence generation
Participants were randomly stratified into wait-list control (n=13) and intervention (n=11) groups based on gender, role and age. The random allocation sequence was generated using Research Randomizer (Social Psychology Network, 2022), a free online resource for assigning participants to experimental conditions. Twenty-four hospital workers were subsequently randomly stratified into waitlist control based on gender, age, role and location. Informed consent was obtained from participants before onboarding into the study. The data managers for this study (initials omitted per double-blind reviewing) generated the random allocation sequence, enrolled participants and assigned participants to interventions.
Intervention Group
Intervention group participants were onboarded onto the smartphone app in September 2021 and assessed over 12 weeks, culminating in December 2021. Wait-list control participants were onboarded onto a restricted smartphone app with access to online surveys only, in September 2021. The same participants were provided with full access to the coach and smartphone app for 12 weeks between January and April 2022. Survey assessments were conducted at three time points (T): T1 September 2021, T2 (January 2022) and T3 for wait-list control participants only (April 2022) to measure changes in wellbeing, burnout and perception of LM vital signs.
Coach Connect Digital Support Platform
Consenting participants were onboarded onto the digital support platform managed by our technical partner (name omitted per double-blind reviewing). All data was stored securely on Amazon Web Services platforms based in (location omitted per double-blind reviewing). Coaches and participants had access to pre-developed evidence-based content (in video, audio and pdf format) related to LM vital signs. An online human coach chose relevant evidence-based interventions, based on individual goals and scores related to participant wellbeing, burnout and perceived lifestyle vital signs. Participants completed all survey assessments on the digital platform.
Coaching Approach
A Positive Health Coaching approach (van Nieuwerburgh & Knight, 2023) was used to deliver online coaching by a qualified, accredited coach (European Mentorship and Coaching Council). Coaching was text-based only via the smartphone app. Review sessions occurred bi-weekly to review and celebrate progress online via the app. Participants had the opportunity to discuss challenges or barriers and make amendments to their change plan.
Primary outcomes
The feasibility of the coach-led digital health solution was measured following the first three components of the RE-AIM framework. Feasibility was examined throughout the project and post-completion.
Secondary outcomes
Changes in wellbeing (PERMA-Profiler) (Butler & Kern, 2016), burnout (Oldenburg Burnout Inventory) (Demerouti et al., 2003) and perceived LM vital signs (1-5 Likert scale on sleep, eating well, daily activity, stress, relationships and avoiding risky substances; 1=poor – 5=very good), measured at three time points (T): T1 September 2021, T2 (January 2022) and T3 for wait-list control participants only (April 2022) to measure the efficacy of the online platform.
Qualitative Assessment
Semi-structured interviews were conducted with 11 participants after they engaged with the Coach Connect intervention (5 wait-list control group participants and 6 intervention group participants). Interviews were conducted via a professional Zoom account. Both the interviewers and the participant kept their videos turned off throughout each interview and used pseudonym names.
Sample Size
As this is a feasibility study, a power calculation to determine sample size was not undertaken (Glasgow et al., 1999). Instead, this sample size is justified based on, (1) the primary focus on feasibility rather than on estimated effects of intervention; (2) past research reporting the median numbers of participants recruited for feasibility studies incorporating both quantitative and qualitative elements (Bell, Whitehead & Julious, 2018); and (3) practical considerations.
Analysis
Comparative statistics (mean, standard deviation) were applied to all data. Inter and intra-group comparisons were calculated using parametric, paired or unpaired (depending on the data set) student t-tests using SPSS. T-values (t) show the difference in means of each group. P-values (p) reflect the probability that there is a significant difference between mean scores. Cohens' d (d) is the effect size for the difference between means. Confidence Intervals (CI) indicate the value range in which 95/ of the population will fall within. Interviews were analysed using thematic analysis to understand the acceptability of the intervention (adoption) and their individual experiences of engaging with the project.
Results
Reach
An anonymous needs assessment survey was conducted (between May and August 2021 – during the peak of the COVID-19 pandemic) with hospital workers from three general hospitals among the Royal College of Surgeons in Ireland hospital group to capture consensus information on lifestyle. All staff working in these hospitals were invited to complete the survey by individual human resources departments and senior hospital management, via staff email. This survey examined needs related to LM vital signs incorporating sleep, stress management, eating well, exercise, relationships, and avoiding risky substances, as well as interest in using smartphone apps for enhancing wellbeing.
The needs assessment survey was completed online between May and August 2021. Respondents (n=119) were predominantly female (82/), aged between 40 and 54 years (44/), and largely members of allied healthcare (41/), medical (19/), and nursing staff (24/) with all other groups (hospital support staff, medical scientists, and administrative staff), accounting for the remainder (16/); all hospital staff were invited to take part. Survey participants were asked about their perceptions of their own health and wellbeing, related to the pillars of lifestyle medicine and whether or not they would like to receive additional support in the form of online coaching. Most survey respondents indicated that they would like support related to exercise (79/), as well as cultivating meaning and purpose in life (78/). Nineteen percent of respondents required assistance with substance control (alcohol and tobacco). Ninety-one percent of participants indicated that were willing to use a smartphone app for health and wellbeing. These findings informed the development of specific online support content (video, audio and pdf files of educational and evidence-based interventions) available to the coach and participants of the subsequent Coach Connect project. Participants were asked if they were interested in taking part in the Coach Connect project during the survey. Twenty-six (22/) out of the 119 survey respondents consented to join the project. The majority of participants (92/) on the Coach Connect project were female, which was largely representative of hospital staff who completed the initial needs assessment survey. Participant professional roles were divided predominantly into health and social care allied health professionals (n=7), medical scientists (n=6) and nurses (5), with two doctors (Table 1). Eighteen out of twenty-four participants were aged between 30 and 49 years.
Coach Connect participant demographics
Adoption (uptake, attrition rates, engagement and response rates)
Uptake
Twenty-six out of 119 of the needs assessment respondents (22/ uptake) were recruited onto the project between May and September 2021.
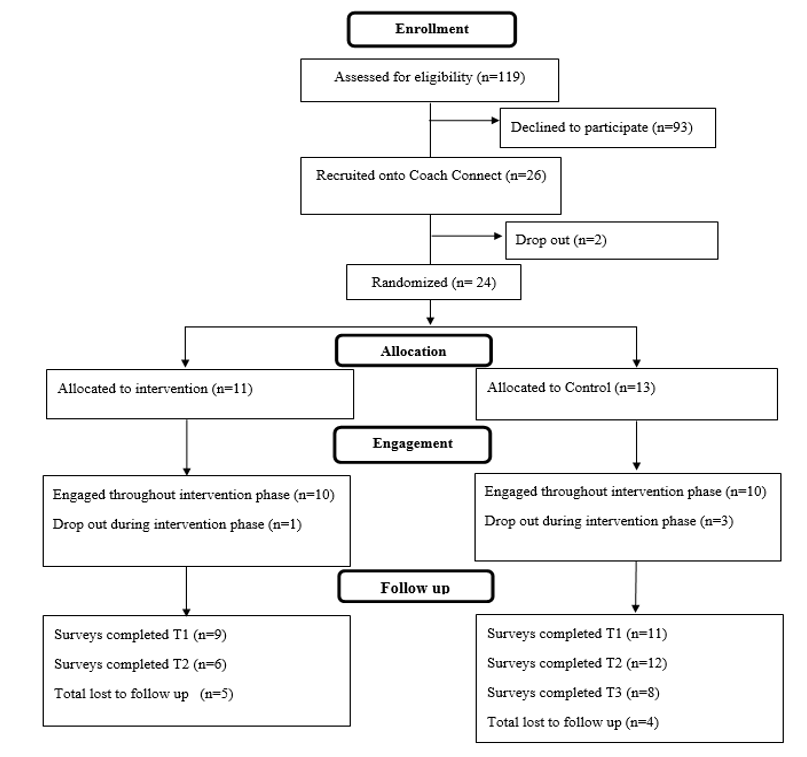
CONSORT Participant Flow Diagram
Reach and Adoption
Reach and adoption (uptake, and attrition rates) of study participants before, during and post-study follow-up. Non-usage attrition refers to participants who did not complete the 12-week programme, while drop-out attrition is concerned with those participants who are lost to follow-up (Eysenbach, 2005).
Engagement as behaviour with the digital health-coaching platform
The engagement of participants from both experimental groups (intervention and wait-list control) with goal-setting sessions and subsequent reviews with the coach is described in
Engagement with the smartphone app
Table showing the number of logins by intervention group (September to December 2021 – January to April 2022) and wait-list control group participants (January to April 2022) onto the smartphone app over two separate 12-week periods.
Participant Goals
Of the participants who engaged in goal setting with the coach, the most targeted LM vital sign was mental health, followed by exercise and movement for both intervention (42.9/ and 14.3/, respectively) and wait-list control groups (37.5/ and 37.5/ respectively) (
Participant goals
Specific pillars of lifestyle medicine chosen as the first goal to improve lifestyle by participants from both experimental groups.
Survey response rates
Within the intervention group, nine participants completed surveys (PERMA-profiler and Oldenburg Burnout Inventory) at T1 (82/ response rate), and six at T2 (54/ response rate). Eleven wait-list control group participants completed the same surveys at T1 (85/ response rate), twelve at T2 (92/ response rate) and eight at T3 (61/ response rate) (Fig. 1).
Effectiveness
Lifestyle Medicine Vital Signs
Perceived changes in LM vital signs were measured over three time points using a subjective Likert scale (1-5). Changes in these subjective scores from study participants are listed in Table 5. Four intervention group participants and three of the wait-list control group recorded improvements in their chosen goal (Table 5).
Goal progress related to LM vital signs
Intervention and wait-list control group participants chose to address specific lifestyle medicine vital signs to improve over each 12-week programme. A score of 1 indicates poor management of the specific lifestyle vital signs, while a score of 5 indicates a perception that this area of lifestyle is well-managed. Intervention group participants did not survey T3.
Wellbeing and burnout
Intervention Group
Overall wellbeing improved between T1 (n=6) and T2 (n=6) (p=.01, d= 1.39). Improvements in Positive Emotion (p=.006, d=1.86), Happiness (p=.04, d= 1.08) and Health (p=.04, d=1.1), with a corresponding reduction in Negative Emotion (p=.02, d=1.3) were also measured between T1 and T2. In addition, overall burnout decreased between T1 (n=6) and T2 (n=6) (p=.04, d= 1.05) with a similar reduction in Exhaustion (burnout subscale) between the same time points: T1 (n=6) and T2 (p=.02, d=1.31).
Waitlist Control Group
There was an improvement in overall wellbeing from T1 to T3 (p=.007, d= 1.52) as well as between T2 and T3 (p=.01, d= 1.18). There was a corresponding improvement in Positive Emotion at T1 compared to T3 (p=.01, d=1.28), Relationships at T2 and T3 (p=.03, d= .92) and in Accomplishment at T2 and T3 (p=.02, d=.99). No statistically significant change was measured for burnout at any time point.
Between Group Results
There was no significant difference in overall wellbeing (between-group PERMA scores) at T1 (p=.37,) or T2 (p=.07); however, medium to high effect sizes were noted at T1 (d=.41) and T2 (d=.97). There was a significant difference in Engagement (p=.02, d=.96) and Happiness (p=.01, d= 1.33) when total intervention and wait-list control scores were compared at T2.
Qualitative Findings
The extended results of these interviews are described in a parallel publication (O’Donovan et al., 2024). They are summarised here. Three overarching themes were identified (Human-centred Conversation, Facilitated Awareness, Learning and Growth, Forward Momentum in the pillars of Lifestyle Medicine). Interviewees had a positive overall impression of their coach and the service provided. Participants reported a positive experience of setting goals with the coach. They felt that the goal-setting process was well-structured and clearly explained. It provided participants with a focus and allowed them to structure their thoughts in relation to their goals. The process also helped participants to become clear about their goals and to find ways of measuring and tracking their progress. Participants felt motivated after their sessions with the coach and felt that they could harness this motivation towards achieving their goals. Working with the coach acted as a catalyst for motivation, which extended into other aspects of their lives. Participants who had lower engagement, still commented that working with the coach was a good reminder to them to continue work towards their goal. The coach was a source of accountability for participants. This was particularly the case with the review sessions conducted with participants on a biweekly basis. Lastly, interviews provided insight into the reasons for mixed levels of engagement on the platform. Barriers to engagement included time, technological issues and external factors. Platform engagement was enabled by a belief that participants were contributing to the greater good and a strong connection to the coach.
Discussion
The Coach Connect project might represent a feasible option to support hospital workers’ wellbeing, based on the first three elements of the RE-AIM Framework (Reach, Engagement and Adoption). However, poor recruitment, high attrition and low survey response rates, as well as mixed engagement (as behaviour) and adoption throughout the project, highlight the need for additional work. Although total participant numbers were low for both experimental groups, those who engaged with the online coach, achieved goals related to improving lifestyle vital signs, improved wellbeing and limiting burnout (intervention group only) over 12-week periods during the COVID-19 pandemic. The feasibility and potential of a digital solution can be measured in numerous ways. We suggest that taking a more traditional quantitative and positivistic approach to feasibility represents only one means of assessment. We propose that taken together, the quantitative and qualitative approaches to assessing feasibility and impact, provide a more rounded evaluation of digital eHealth platforms such as the one described in this study.
Reach and Recruitment
The reach for the initial needs assessment was very low (0.29/), while the recruitment onto the Coach Connect study, from survey respondents was higher (22/). These low reach and recruitment rates might have been partially due to the fourth wave of Covid-19 occurring in Ireland between June and July 2021[52]. This placed increased pressure on hospital workers during that time (including increased workload, staff shortages and themselves or a family member contracting Covid-19). As a result, many hospital workers may not have had the time or resources to take part in a research study. Previous research has highlighted that it is challenging to recruit hospital workers for research projects and that this may be due to their lack of time, high workload, study burden, ambivalence about the value and applicability of the research being conducted, perceived lack of research experience, skill, or knowledge (Asch et al., 2000; Hummers-Pradier et al., 2008; Nkrumah et al., 2018; Jahan et al., 2015). A study examining the facilitators and barriers to the recruitment of community-based healthcare providers found that while extrinsic motivation might aid in the initial enrolment of hospital workers, it rarely resulted in active participation long-term (Krebs et al., 2021). Instead, they suggest that having an intrinsic motivation and interest in the trial’s aims and goals is as important in facilitating hospital worker recruitment (Krebs et al., 2021). Broyles et al. (2011) recommend the use of multimodal recruitment strategies including email, flyers, presentations at clinical forums, and face-to-face recruitment to improve hospital worker recruitment. They highlight that these multimodal approaches play a vital role in enhancing contact, communication, and rapport building with hospital workers. Hospital workers have reported that a key incentive for taking part in research is the potential benefit that the outcomes of the research may have (Jahan et al., 2015; Brodaty et al., 2013; Murphy et al., 2015; Rosemann & Szecsenyi, 2004). Therefore, the positive trends reported in the current study may be beneficial when recruiting participants for future research in this area.
Adoption (uptake and attrition)
Attrition rates are notoriously high among web-based internet and digital eHealth-based solutions (Eysenbach, 2005; Meyerowitz-Katz et al., 2020). In 2005, Eysenbach (2005) defined two types of attrition related to eHealth solutions: (1) non-usage attrition, when participants do not complete a prescribed study programme, and (2) drop-out attrition, losing participants to follow-up. There is evidence of both types of attrition in this study. Non-usage attrition was relatively low among intervention group participants (9/) but was significantly higher among their wait-list control counterparts (23/). Dropout attrition was higher than non-usage attrition for both the intervention and wait-list control groups. As with Reach, these high attrition rates might have been due to the fifth wave of COVID-19 infections that hit Ireland in January 2022.
Engagement
Broadly speaking, two types of engagement with eHealth or digital health solutions have been described in the literature: (1) the amount of enjoyment experienced from engagement and the level of attention to the digital platform as an interactive technology, and (2) engagement as behaviour, which describes the frequency and duration of engagement (e.g., number of logins over time) (Ryan, Bergin & Wells, 2018). Perski and colleagues (2017) suggest an integrative conceptualisation of engagement that can be measured using self-report questionnaires, verbal reports, automatic recording of digital platform use as well as biological and psychological parameters. It is clear that traditional positivistic approaches to measuring engagement are not sufficient to measure engagement, according to the conceptualisations described above.
There was mixed engagement in behaviour with the Coach Connect platform, which may also have been exacerbated by the timing of the intervention during the COVID-19 pandemic. Generally speaking, engagement as behaviour (measured by the number of logins and scheduled sessions with the online coach) peaked at the start of each study period and tailored off as time progressed. Furthermore, there was a significant amount of heterogeneity in engagement as behaviour with some participants not engaging, even at the start of each study period. Participant and coach experiences of engagement with the Coach Connect digital support platform are presented and discussed more detail in our qualitative findings (reference omitted per double-blind reviewing). Findings from this parallel qualitative study revealed that lower engagement with the coach was not linked to poorer outcomes for participants or decreased motivation to work on their goals. Additionally, participants felt connected to their coach and experienced benefits in their lifestyle and wellbeing that continued even when they stopped engaging with the coach. This parallel study also identified the barriers and facilitators of hospital workers engagement with the digital platform (reference omitted per double-blind reviewing).
Effectiveness
The most commonly targeted lifestyle vital signs by participants were mental health and exercise. Participants reported improvements in their goals after working with the coach; three participants reached their long-term goal related to LM vital signs during the project. Improved wellbeing and burnout were observed for those participants who engaged (even once) with the online coach. The core support content and approach by the online coach for this project are based on those described in positive health science. We believe that this theoretical and practical approach, which includes positive psychology-based interventions such as meditation-based practices among others (Lynch et al., 2018; Tement et al., 2021; Dunne et al., 2019; Wen et al., 2017) can help to mitigate burnout and enhance wellbeing among hospital workers (Bazargan-Hejazi et al., 2021).
Strengths
The current study addresses the need to include a control population when examining the impact of an online intervention to improve hospital workers wellbeing and reduce burnout (Wen et al., 2017; Pflugeisen et al., 2016). We have used two validated surveys to measure participants’ wellbeing (PERMA-Profiler) and burnout (Oldenburg burnout inventory). Qualitative data was also collected to provide an in-depth understanding of participants’ experience of engaging with the online digital platform, however, these findings have been reported elsewhere (reference omitted per double-blind reviewing). The information gathered in the current study will inform future research to develop an Intelligent Coaching Assistant (ICA) that can augment the coach-led digital platform for both coaches and users.
Limitations
For the current study, participants were asked to simply rate their perceived competence with engaging practices that cultivate or manage LM vital signs. Future research should use a more detailed and validated measure, similar to the Short Multidimensional Inventory Lifestyle Evaluation-Confinement (SMILE-C) scale (Balanzá-Martínez et al., 2021), although longer assessments may further impact response rates. The current study has a small sample size, which limits the generalisability of our findings. In addition, underpowered significance tests may lead to both Type I and Type II errors (Orsmond & Cohn, 2015). It remains important that studies with larger numbers should be carried out to confirm the results reported by our study. Our sample included only two men, meaning that findings are likely not be representative of the general healthcare population. Unfortunately, the low numbers of male hospital workers participating in similar initiatives is common (Wen et al., 2017). Larger studies should also investigate any difference in engagement and effectiveness of the intervention based on gender, age or work role.
Future Research
Future research should include larger sample sizes and be conducted in different healthcare settings, incorporating geographical and cultural diversity. Multimodal approaches to recruitment should be used to enhance contact, communication and rapport building with hospital workers. The positive trends identified in the current study should be used to highlight the potential benefits of engaging in similar research projects and foster hospital workers’ intrinsic motivation to participate. Future research should also examine the sustained effect of the online coaching intervention by conducting long-term follow-up studies. This would provide important information to healthcare organisations to help them to plan and implement interventions to support hospital workers’ wellbeing (Tement et al., 2021). Finally, additional studies will adopt a more rounded approach to engagement that will include the traditional quantitative with qualitative assessments.
Conclusion
Coach Connect might represent a feasible option to support hospital workers’ wellbeing. This is important given the high levels of poor wellbeing and burnout found among hospital workers (Johnson et al., 2018; O’Connor et al., 2020; Chirico et al., 2021; Nishimura et al., 2021) and the need to implement approaches to improving and maintaining hospital workers wellbeing (Søvold et al., 2021; Burton, 2010; Rehder et al., 2021; National Academics of Sciences, 2019). Combining human coaching with technology to support Hospital workers wellbeing can facilitate access to affordable interventions regardless of geographical location (Stoyanov, 2021; van Coller-Peter & Manzini, 2020; Borghouts et al., 2021).