
Abstract
Doctors' wellbeing is overlooked, although stress and burnout is high. Evidence suggests links between mentoring and health and wellbeing, but little is known. This mixed methods, Realistic Evaluation investigated relationships between mentoring by ‘trained’ mentors, and doctors experiences of health and well-being. Data included a questionnaire (n=57) and multiple interviews (n=43) with 13 mentors over 20 months. Findings identified many threats to doctors’ health and wellbeing. However, an ‘empowerer’ model of mentorship enacted via formal and informal interactions enabled constructive responses which go beyond individuals to groups, and appear to increase social capital, individual and group agency, resourcefulness and resilience.
Introduction
Mentoring has always been a form of support for doctors but is traditionally associated with senior figures with little or no preparation offering advice and sponsorship to junior colleagues (Connor et al., 2000). Indeed, the Collins Dictionary describes mentoring as just this; “the practice of assigning junior members of staff to the care of more experienced people who assist them in their careers”. However, a profound shift in emphasis has taken place with mentor preparation and training courses developed which teach professionals at any career stage to use ‘empowerer’ frameworks to help mentees work through issues or problems (Connor et al., 2000; Terry et al., 2019). The Collins Dictionary defines empower as “to give them (someone) the means to achieve something” and Mentor preparation courses with this focus are increasingly available. Mentoring schemes now frequently utilise such ‘trained’ mentors and offer support to doctors in coping with difficulties, transitions, and expectations (Terry et al., 2019). Experience, advice, and patronage do not figure in these schemes. There is also a growing literature (Beech & Brockbank, 1999; Department of Health, 2004; Memon & Memon, 2010; Steven et al., 2008; Terry et al., 2019; Wilson et al., 2017; Desselle et al., 2021) suggesting mentoring may benefit professional practice, personal and professional development, and health and wellbeing (H&WB). However, little has been done to investigate any links between mentorship activity by mentors trained in ‘empowerer’ frameworks and doctors’ health and wellbeing.
As well as being “a proven path to scientific progress” (Lescano et al., 2019 p3),mentoring as a form of collegial support echoes a growing strategic focus on healthcare professionals' health and well-being (H&WB)(Boorman, 2009; Department of Health, 2010) highlighted in the recent ‘Caring for doctors Caring for patients’ report (West & Coia, 2019). Wellbeing is often used to encompass various health-related subtleties, including traditional objective components of health, and more ‘subjective’ or personal attributes. Low levels of subjective well-being are associated with increased anxiety and depression, whilst high levels are considered to reduce morbidity and mortality (Beech & Brockbank, 1999). The Department of Health described ‘Wellbeing’ as “Feeling good and functioning well and comprises an individual’s experience of their life, and a comparison of life circumstances with social norms and values” (Department of Health, 2014).
The heightened focus on staff H&WB relates to mounting evidence indicating relationships between H&WB levels and staff retention, employee engagement, motivation, and performance (Fairhurst & O’Connor, 2010; West & Coia, 2019). Elton (2019) points to some structural changes in the medical profession that potentially contributes to this. For example, the shorter 4-month hospital rotation influencing confidence building, absence of "the old style ‘firm’ and removal of the doctors’ mess. Studies report higher incidences of work-related mental ill-health reporting in doctors in comparison to other occupations (West & Coia, 2019; Zhou et al., 2017) and postulate repercussions both for the individual, care quality and patient safety. Similar conclusions emerged recently from the Picker Institute and Kings Fund, suggesting work pressures and limited resources impact negatively on staff wellbeing, and in turn patient experience and care quality (Sizmur & Raleigh, 2018). Links between wellbeing, staffing and care provision are pertinent in times of limited workforce supply, issues with retention and a continued drive for safer, more effective, and efficient care (Gerada et al., 2018; Kinman & Teoh, 2018; West & Coia, 2019). Indeed, in low and middle-income countries effective mentorship is valued for underpinning capacity building (Hansoti et al., 2019).
Medical bodies such as the British Medical Association (BMA) promote mentoring as a support mechanism, and much research has explored organised mentoring schemes and activities, highlighting roles, functions, benefits, and challenges (Connor et al., 2000; Overeem et al., 2010; Steven, 2015). However, where conceptualisations of mentoring are explicit in publications these tend to either rely on received wisdom, patronage-based notions of mentoring or describe limited mentor preparation concentrating on process aspects such as frequency and length of meetings. Meanwhile the collective experience of the authors in mentoring, mentor training, and mentoring research, over two decades increasingly indicated possible links between the mentoring activities of those prepared in using ‘non-patronage’ models of mentoring and improved health and wellbeing.
A systematic narrative literature (Wilson et al., 2017) exploring relationships between mentoring and doctors Health and wellbeing reported finding evidence of some relationships. However little of the literature examined explicitly related to ‘trained’ mentors or the use of mentoring frameworks indicating a lack of research focusing on the experiences, practices and perspectives of doctors who have attended mentor preparation courses and are trained to use specific models, techniques, or frameworks.
To begin to fill this knowledge gap this study aimed to;
Retrospectively explore any links between trained mentoring activities and H&WB, via a questionnaire survey of doctors with >2 years’ experience as trained mentors, giving a ‘historical’ perspective.
Contemporarily track mentoring activities of doctors who had < 2 years' experience as trained mentors, to explore if and how they enact mentorship through employing frameworks and skills learnt, and what, if any, relationships were noted regarding the H&WB of those involved.
Previous studies indicate that skills become embedded and to some extent tacit (Eraut, 2000, 2004), thus, the contemporary tracking element of this research attempted to capture perspectives from participants potentially still ‘conscious’ of their mentoring skills.
Methodology and Methods
This study is based on the view that both education (e.g., mentor training and development programmes) and professional support activities (e.g., mentoring activities) are complex social processes which take place in complex settings. Therefore, methodology drew on Realistic Evaluation (RE) principles (Pawson, 2013), which views social reality as complex and multi-layered. RE proposes that by comparing what works, how and why, and under what circumstances, commonalities, and variations across contexts (e.g., environmental factors), mechanisms (e.g., individual agency and actions, systems, and process), and outcomes (perceptions and experiences of health and well-being) can be explored. Mechanisms at play may span individual and structural levels, involving both resources and reasoning, which in conjunction with the context lead to particular outcomes (Dalkin et al., 2015). Unlike traditional science research which attempts to study phenomena in closed systems, investigations to reduce bias or influence (e.g., Randomised Controlled Trial), RE emphasises the importance of both identifying mechanisms of change, and their relationships to the complex social contexts of implementation (Dalkin et al., 2015; Pawson, 2013). Therefore, associations between learning mentoring frameworks and techniques, engaging in mentoring activities, and health and well-being outcomes were sought, interrogated and potential associations or configurations outlined.
Patient and Public Involvement statement
Patients and the public were not involved in any way in this research given the study was focused specifically on Health care professionals.
Ethics
Approval was gained from Northumbria University Faculty of Health and Life Sciences ethics panel (ref DHCSteven171014). Participation was voluntary, written informed consent gathered and on-going consent checked at each stage. Interviews were recorded, transcribed, and anonymised, except for one participant who preferred written notes to be taken.
Data collection and participants
Key to the study was the recruitment of participants who had attended a mentor preparation course which taught a framework-based approach (Connor & Pokora, 2007; Terry et al., 2019). Although not completely standardised, courses commonly run over 3 or 4 days and include theoretical ‘teaching’ of the frameworks, demonstrations of framework and associated skills use, group practice and feedback, and discussion. Courses are often provided by professional bodies, associations, and Healthcare organisations (Terry et al., 2019).
An online questionnaire was carried out followed by semi-structured interviews. The online questionnaire was developed and disseminated via SurveyMonkey® software (www.surveymonkey.com). This questionnaire was distributed to doctors with >2 years’ experience as trained as mentors. Questionnaire development drew on; a previous tool (Steven, 2015), the Business in the community Workwell model (Business In The Community, 2013), the literature review (Wilson et al., 2017), and the British Medical Association’s cohort study (Health policy and economic research unit, 2015). The questionnaire included definitions of mentor, mentoring, and H&WB, with fixed or open-text questions covering five sections:
Job / role
Mentor training
Mentoring activities
Issues brought to mentoring sessions
Perceived H&WB impact of mentoring
Pre-testing involved 10 individuals to enhance quality (Aday & Cornelius, 2006). The questionnaire link and study information were distributed through established professional Association and Royal College mentoring networks to 181 individuals. Participation was optional, and given the historical nature of some lists, validity of email addresses was uncertain. 57 people responded (response rate: 31/), characteristics are shown in table 1.
Questionnaire Respondent characteristics
Following the online questionnaire, a series of semi-structured interviews were carried out with doctors who had < 2 years' experience as trained as mentors. Each participant took part in up to four interviews over 20 months (total 43 interviews) (see Appendix 2 Interview Matrix). Purposive sampling drew on nationwide training distribution lists. Thirteen doctors (10 male; 3 female) participated across the UK. Specialties included surgery, anaesthetics, general practice, and general medicine. The interview schedule drew on the previous literature review (Wilson et al., 2017) and findings from the questionnaire. As is accepted in qualitative research practice, the interview guide was not prescriptive given each narrative was unique, evoking particular follow up questions (Cresswell, 2013). Participants were encouraged to raise issues they felt important, thus allowing new insights. Forty-three interviews were completed, nine participants completed four, two dropped out after two (no reason given), two were unable to complete one interview due to ill health.
Data analysis
Thematic analysis of interview data and questionnaire free text drew on realistic evaluation principles. These methodological principles were complimented by use of the Business In the Community Workwell model (Business In The Community, 2013), which incorporates physical, psychological, and social components of H&WB. The BITC Model (2013) outlines an understanding of each component, and these are expressed in Table 2.
The four components of the BITC Model (2013)
These components are viewed as acting together in creating healthy environments that support employee H&WB. The BITC Model acted as a heuristic coding framework aiding analysis, but we were vigilant to the potential for forcing or constraining the analysis.
Analysis was facilitated by NVivo 11 Software (https://www.qsrinternational.com). Interviews were coded independently by individual team members as the data was gathered. Team members were researchers with nursing, midwifery, medical and educational experience which brought a range of viewpoints and understanding to the data. Coding was then compared, discussed, assumptions challenged, refuted if applicable and confirmed in a series of whole team workshops to minimise researcher bias and to consider research reflexivity. As the project progressed coding incorporated topics emerging from the initial interviews with categories, and sub-categories developed to allow additional areas to emerge inductively. Quantitative responses in the online questionnaire data were analysed using descriptive statistics. Data set comparisons from the online questionnaire and semi-structured interviews were made. In addition, the analysis also tracked as far as possible, ‘enactment’ of mentorship (use of elements of the mentoring models taught), and each mentor-mentee situation described by the mentors over multiple interviews.
Critics of realist evaluations argue that they lack explanatory focus, with some researchers simply listing contexts, mechanisms, and outcomes as factors without reflecting upon them or investigating them in configurations (Pawson, 2013). To address this, after thematic analysis and data set comparisons from the online questionnaire and semi-structured interviews, two authors (AS & VL) re-examined the themes to outline configurations (Table 3). These were then re-explored in detail in a series of whole team workshops in order to enhance rigour, and explanatory models illustrating emerging configurations and relationships were developed (Figures 1 &2).
Results
Analysis provided four outcome themes in which mentorship emerged as:
An overarching vehicle for better specialist support
Supporting better personal and professional relationship building
Supporting better professional and personal well being
Supporting better working communities and cultures
This is illustrated by Figure 1 which provides an overview of the entire process, indicating the complex interplay at work during ‘enactment’ giving rise to a range of reported outcomes.
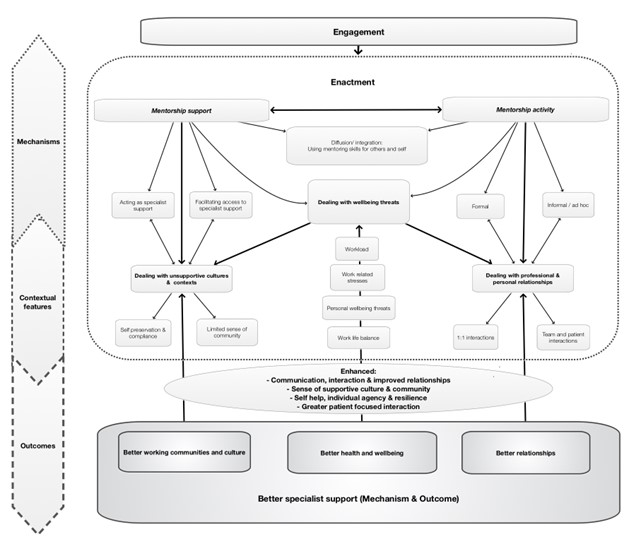
Explanatory model of mentorship engagement leading to enactment and better specialist support
The thematic narrative which follows uses data, 2 linked explanatory models and Table 3 to illuminate the themes and demonstrate the complex interplay at work between contextual features, mechanisms, and outcomes. Where data excerpts are used ‘Q’ indicates questionnaire participant, ‘P’ an interviewee.
Engagement – the first step
The first step of all mentoring activity is for the mentee to desire and be able to engage with the mentoring process. This process is illustrated by Figure 2
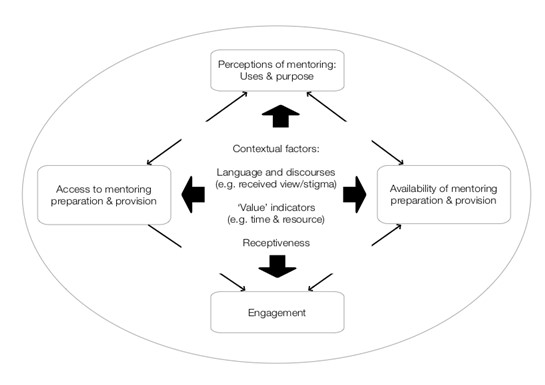
Explanatory model of initial engagement
Figure 2 shows issues and relationships influencing initial ‘engagement’. Participants considered mentorship acted as a vehicle for providing specialist support but emphasised engagement in mentoring preparation courses and other mentoring activities (e.g., mentoring schemes or networks) as a fundamental starting point.
Access to ‘training’ and mentoring relationships was influenced by a lack of mentor preparation opportunities and limited publicity or awareness of courses and schemes. This was compounded by limited ability to engage with courses that did exist, exacerbated in resource poor contexts by the limited value placed on mentoring by individuals and organisations. One questionnaire respondent noted “you never get credit for it (P036)” while others noted,
We don’t get provision for anything outside of the clinical timetable at all. So not even completing our e-portfolio or completing audits. And so all of it is done in our own free time. PG
Being allowed time in my job-plan for mentoring would make me feel that the organisation values its contribution” [QP40]
Workplace cultures acted to reinforce certain perceptions and utilising mentors as a ‘disciplinary’ or ‘remedial’ measure was felt to stigmatise and consequently limit receptiveness. This potentially influenced access intentions of both doctors wishing to learn how to mentor, and those wishing to be mentored.
Again, there’s a perception it’s for doctors that are in difficulty . . . I think there’s sometimes possibly a feeling that there could be some stigma for seeking mentorship PA
Thus, engagement emerges as central to mentorship enactment, and is co-dependent on conditions such as availability (of courses and mentoring opportunities such as formal schemes), awareness (of what is available) and access (influenced by resource provision). These conditions appear influenced by interlinked contextual features often functioning as mechanisms, such as received views of mentoring, the value placed on, and organisational support (resources) given to programmes and schemes.
Enactment- the second step
Once engagement is established, mentorship enactment through activity enables support to emerge. These become intermediate level mechanisms through which other CMO configurations come into play to engender better relationships, better working communities, and better health and wellbeing outcomes, as illustrated in Figure 1 at the beginning of the results section. The different components are described next.
Mentorship as a vehicle for better specialist support:
Mentors utilised the frameworks, techniques and skills learned to ‘enact’ their mentorship via various activities. The most cited framework was Egan’s ‘Skilled Helper’ model (Egan, 2010). Participants commented that techniques inherent to this framework were often new to them and involved mentors suspending customary diagnostic ways of thinking and behaving - away from diagnosis, management and advice giving. At times mentors found this challenging and mentees surprising, as they expected directive guidance.
most difficult is keeping my mouth shut and not telling them what to do. So it’s about listening and getting them to verbalise everything that’s going on in their head PP
‘Opens up a whole new way of thinking’ [QP16]
Mentoring conversations attended to the individual, prompted mentees to reappraise and review situations and assisted them to develop solutions in a tangible way.
people like the fact that it (mentoring) ends in something quite concrete – so the timeline with the set list of things to do that have been… That feels very achievable PG
Both mentors and mentees acknowledge the importance of building trust to maximise mentoring success. Respondents highlighted the importance of confidentiality and being “listened to non-judgementally and respected (QP29)”. This involved mentors being approachable, empathetic, and non-judgemental.
Often if people come and talk to you, they’re suspicious – what are you going to say? Are you going to report to someone? Gaining trust becomes more important. So once we felt comfortable with each other’s company, then he started opening up. PL
Although some participants differentiated between support and the risk of dependency, mentoring was predominantly experienced as a mechanism enabling access to focused collegial support. Where mentoring alone was insufficient, it provided routes to additional specialist services.
we went through quite a number of (mentoring) sessions. I said on a number of occasions, “I really think you ought to consider seeing your GP because there is an element of depression…I got him/her assessed by occupational health. PO
Questionnaire results: Issues discussed during mentoring sessions
Mentorship supporting better personal and professional relationships
A frequent outcome of mentorship was the enhancement of personal and professional relationships. This included relationship issues brought to formal mentorship interactions (see table 3) and ad hoc application of mentoring skills to develop collegiate relationships. Workplace relationships prompted ad-hoc skills use in a range of informal situations. This included providing opportunities to colleagues who were unlikely to engage in formal mentoring but who benefitted from a mentoring approach, by enhancing 1:1 and team interactions.
don’t think he appreciates anybody thinking he was failing horribly or weak or anything else. And so I think he would have found it very difficult coming to me, (for mentoring). But me going to him and just chatting about stuff enabled him to come to (a solution) PJ
Mentorship supporting better professional and personal well-being
Questionnaire participants identified the frequency of issues discussed during mentoring, many of which can be viewed as constituting wellbeing threats (see table 3).
Within the interview data, many mentions were made of workload related stress and its impact.
it was all about workload. And feeling guilty.... the hospital altered the way it wants consultants to work. . . He/she found it difficult to admit that it was affecting his/her health . . clearly it was… he/she was losing sleep, anxious, worried, wasn't concentrating.. . And I think he/she found the mentoring helpful PO
Mentoring skills and techniques enabled both mentees and mentors to respond more constructively, using techniques to ‘self-help’. Re-appraisal of professional and personal concerns contributed to mentees (and mentors) feeling generally more positive about themselves and the workplace, suggesting development of individual agency and resilience strategies.
helped him to use his energy and time in a more constructive way… Rather than trying to struggle to fit in and then getting very over-burdened. PL
The enhanced positivity reported appeared associated with perceptions of being valued and able to help mentees achieve goals, role fulfilment, job satisfaction and mentoring as giving “a sense of legacy (QP06)”.
huge benefit to me (mentoring) in terms of feeling valued, feeling my worth, aspects of one’s self. Be it worth or esteem or knowing. Because then there is a bit… This sort of veneer against all that is out there, that demoralises and leads to a disillusioned workforce. So I feel somewhat protected, or armoured– against what is out there that others might succumb to. PM
Questionnaire respondents overwhelmingly viewed involvement in mentoring as positively, or very positively, influencing Drs H&WB (see table 4). However, a few questionnaire respondents described mentoring as being stressful, tiring and sometimes ‘uncomfortable’ (P001, P040, P031, P036, P048, P057). One described mentoring as leading to “sleepless nights when the process runs into difficulties” (P045), which highlights a need for mentor support systems.
Questionnaire items relating to perceived impact and influence of mentoring
Mentorship Supporting Better Working communities and cultures
Existing practice contexts were described as largely unsupportive and with a limited sense of cohesion or community which at times resulted in a focus on self-preservation.
I don’t see many happy doctors anymore. Because it’s such a stressed organisation as a whole.… I think trust is missing at the moment. I think everybody is self-protecting PF
Issues of bullying and lack of support were also mentioned
I went through the mentoring process with him/her… in this particular instance, there was a clear element of bullying in the department...PO
Oh, without doubt it’s [support] lacking in medicine in generally. Totally. You know, you’re supposed to show no weakness, I think, as a rule. If you show weakness… It’s very much dog eat dog, without a doubt. You know, there is… There is not much room for people to fail, I think, you know. There’s no option. And considering we work in a caring profession, that we don’t care for each other very much at all, really. Which is a bit disheartening. PJ
Working within such cultures was perceived as unconducive to a healthy work-life balance (see Table 4), which consequently was a common focus of mentoring conversations.
Most of the time it’s juggling work-life issues (refers to mentoring sessions)... Feeling overwhelmed by trying to juggle, kind of, career and family life PG
Participants suggested mentoring could act as a mechanism mediating unsupportive environments and facilitating development of cohesive and supportive communities of practice (Table 4). This sense of cohesion was considered to be derived from application of mentoring skills, particularly those that improved communication. This enhanced individuals’ sense of belonging to, and being valued as, part of the community.
It (mentoring framework and skills) helps with communication on all levels, really. Because it does improve listening. And so I think for meetings, things like that I’m more likely to listen for longer. And then also often recap what somebody was saying. Just to make sure that they knew that they would be listened to PJ
An emotionally safe practice environment was recognised as crucial, enabling staff to raise concerns, potentially benefitting organisational function including patient care.
I think the only happy ones (Drs) I see are the ones who feel safe, at least amongst their team. That, actually, I can raise a concern. And I won’t pay for it, or be judged for it or… And people will listen (implies mentoring) PF
Questionnaire respondents overwhelmingly viewed mentoring as engendering a supportive environment (Table 4). However, moving beyond working environments or cultures several participants described using mentoring skills to benefit patient care.
I probably do use them (mentoring skills) ...When I’m discussing treatment options with patients, you know. So I think you do use those skills. You know, I think it maybe gives you a tendency to be more patient-focused and perhaps explore… Explore what a patient’s wants and needs are. And then target your interventions to that, you know.” PA
I experienced that [feeling of not being listened to], first hand. The, sort of, need to shout and say, “Just listen to me.” You know, nobody is listening to me… Having experienced it first hand, I [also now after learning about mentoring] listen to patients differently.PF
And this [mentoring skills and techniques] comes in handy when you deal with patients. Particularly if you say that you have to take the confidence from the patient to make the decisions... I apply it more in patient situations now. PL 2
To conclude this section, the principles of Realistic Evaluation (Pawson 2013) as applied to the results are provided in Table 5 which gives an overview of each outcome theme, related categories which can be viewed broadly as mechanistic and/or contextual (indicated by C and/or M) and configuration statements.
Themes, categories, and configurations
Discussion
Our findings illuminate how learning specific ‘empowerer’ orientated mentoring frameworks and skills, and mentorship enactment via engagement in mentoring activities appear associated with more positive H&WB; improved personal and professional relationships, and enhanced working communities and cultures. We suggest this facilitates and supports improved medical working and ultimately, enhanced patient care (Sizmur & Raleigh, 2018; West & Coia, 2019). The model developed (Figure 2) illustrates ways in which the mentoring approach learned and enacted (Egan, 2010; Terry et al., 2019) engenders a form of ‘mentorship’ which acts as a vehicle for better specialist support. This mentoring approach (Egan, 2010; Terry et al., 2019) positions those involved differently to traditional methods, in that the mentor, while assisting the ‘mentee’ to work through their issue and arrive at an action plan, does not use experience or authority to advise, steer or drive the mentee (Connor & Pokora, 2007; Terry et al., 2019). This ‘other’ centred, or developmental approach appears facilitatory, positioning the mentor as an empowerer rather than a ‘superior’ adviser or rescuer. Traditional patronage or sponsorship styles of mentoring can be seen as practices which emphasise hierarchy and authority, thus reducing or curtailing the ‘individual agency’ of the mentee and positioning this with the mentor. In such situations mentoring can be viewed as presenting experience as ‘foundational and authoritative’ (Usher et al., 1997), thus, perhaps privileging length of service and maintaining disciplinary power systems.
‘Empowerer’ approaches place agency almost entirely with the mentee, potentially enhancing ownership and satisfaction, and perhaps developing more effective coping mechanisms. Participants reported using aspects of the approach to ‘self-mentor’ making them feel more able to deal with situations. In this study, empowerer approaches to mentoring seemed to encourage the development of social capital, evidenced by some mentees crossing traditional hierarchical power boundaries to develop intra and inter group relationships, as well as vertical relationship networks (Desselle et al., 2021). Between colleagues, ‘bonding and bridging’ relational networks emerged that nurtured positive social relationships through the development of trust and sense of community and camaraderie (Desselle et al., 2021;Ommen et al., 2009). Collectively, this potentially enhances individual, team and organisational social capital , and in turn “helps people and organizations cope with stress and helps foster salutogenic potential” (Ommen et al., 2009) a clear advantage for both doctors H&WB, and patient care. While some view mentoring as aimed at the individual and suggest links with personal resilience development (Hamilton & Forbes, 2017), we postulate that learning and enacting ‘empowerer’ approaches engenders greater individual and team resilience and becomes a humanistic mechanism for dealing with a variety of situations as identified (see Table 3).
Participants reported they and ‘mentees’ experienced multiple, often significant wellbeing threats frequently related to relationships, workload, competing priorities, working cultures and conditions. This concurs with UK work (McKinley et al., 2020; Sizmur & Raleigh, 2018; West & Coia, 2019), indicating high levels of burn out, with suggestions and conclusions that staff wellbeing is impacted by overstretched workforces, while internationally, others highlight increased levels of stress, anxiety, mental illness and burn-out amongst doctors (Dewa et al., 2014; Gerada et al., 2018; Kinman & Teoh, 2018; Kumar, 2016). Suggested causes include heightened expectations to deliver more with fewer resources, systems undermining peer support and unsupportive, or ‘blaming’ cultures (Gerada et al., 2018), perhaps even more so in the current Covid situation.
As the powerful and sometimes harrowing accounts in this study indicate, reduced wellbeing and ‘burn-out’ comes at a cost for individuals, healthcare organisations and systems, and patient care (Kumar, 2016). A survey of UK doctors (Sizmur & Raleigh, 2018) reported 31/ felt a more manageable workload would help and nearly a third described being ‘burned-out’. Experiences of study participants parallel suggestions from a UK doctors mental health report (Kinman & Teoh, 2018) proposing Drs are at greater risk of ‘work-related stress, burnout and mental health problems’ than the general working population, and recommending, “Processes which encourage better support at work, such as mentoring and effective team working, need to be facilitated” (Kinman & Teoh, 2018 p3).
This concurs with a review into factors impacting on the mental H&WB of medical students and doctors (West & Coia, 2019) which highlights the importance of supportive cultures and the potential of mentoring as a vehicle for better specialist support - as found in this study. Indeed, relationships and working in supportive teams may positively impact stress levels by influencing social support and role clarity (Boorman, 2009 ; Department of Health, 2004; Fairhurst & O’Connor, 2010; Gerada et al., 2018; Kinman & Teoh, 2018; Sizmur & Raleigh, 2018; Zhou et al., 2017). In this study, the skills and approach learnt were enacted beyond formal situations, skills use was not compartmentalized but employed in multiple places and spaces (including corridor conversations and team meetings), via a collaborative style which seems to engender cultures where people feel valued and listened to. However, for benefits to be actualised they rely upon engagement in and with ‘mentorship’, in turn dependent upon availability of, and access to, mentor preparation courses and trained mentors. This crucial ‘access’ is influenced by multiple mechanisms; some latent including received views and ‘receptiveness’ of those involved (Steven et al., 2008; Desselle et al., 2021) and other contextually contingent issues including availability and awareness of courses and schemes. Furthermore, participants described common perceptions of mentoring as a ‘remedial’ measure, inferring failure, lack of competence or capability. Consequently, involvement, especially as a mentee, was potentially stigmatising, similar perceptions of stigma have previously been reported elsewhere (Memon & Memon, 2010), and may discourage engagement.
Received views regarding the value and legitimacy of mentoring may also influence resource allocation decisions. There is a need to reduce stigma surrounding mentoring and enhance its value and legitimacy to promote engagement, enabling mentoring to become a more widespread vehicle for specialist support, thus helping us care for our staff and ultimately provide better patient care. Achieving appropriate funding for trained mentors’ time and mentoring schemes, underpinned by framework-based mentor preparation courses which have a positive learning climate and clear learning outcomes, may be difficult in the current climate of austerity and workforce shortages where continuing professional development may be cut first. However, for successful mentorship, all levels; mentee, mentor and institutional, should be considered and this also has much relevance for the critical issue of succession planning (Hansoti et al., 2019). These are issues for policy makers and clinicians to consider.
Limitations and strengths
This study involved individuals interested in mentoring, perhaps predisposing them to positive views. However, this is not reason to disregard mentorship or mentor education, perhaps like medical specialities mentoring is something which attracts certain people, but which may benefit many more beyond.
If mentor education is perceived as an ‘intervention’ there are also limitations in the non-standardised character of course content and delivery. Our samples are not representative interviewed were mainly men, however participants included various UK specialties and locations. Although findings may not be statistically generalisable, we suggest they have resonance and transferability.
Conclusion
This study suggests ‘empowerer’ mentorship approaches have significant positive impacts on H&WB which go beyond individuals to groups, teams, and communities of practice, and which increase individual and group agency, resourcefulness, and resilience. However, to engender such benefits, a change in current received views, which stigmatize and devalue mentoring, are needed. More research into impacts on mentees is required –especially tracking impacts over time. Discerning ‘effect’ in mentoring is similar to difficulties experienced in trying to link education to patient outcomes and requires diverse research approaches to build a multi-facet body of knowledge and evidence. To reap the benefits highlighted in this study requires a cadre of ‘trained’ mentors, skilled in empowerment approaches. Training should be framework-based, with attention paid to providing a range of activities within a positive learning culture, within a structure that scaffolds and builds over time (Sheri et al., 2018; Desselle et al., 2021). Indeed ‘humanizing’ attitudes towards doctors' health and wellbeing, surfacing the paradox between expected ideas about what a patient is in relation to what a doctor is (Wistrand, 2017), to caring for doctors physical, psychological and social health and wellbeing is increasingly important in the current global health care situation (West & Coia, 2019). The relatively small amount of resources required to provide courses, alongside ongoing support and encouragement of mentorship could have the potential of large benefits, including as this study indicates, humanizing support impacts on staff wellbeing and patient care.