
Abstract

Discovery consists of seeing what everybody has seen and thinking what nobody has thought
Albert Szent-Gyorgi (1893–1986)†
†From The scientist speculates, by Irving Good in 1962. Hungarian-born physiologist who discovered vitamin C and was awarded the Nobel prize in Physiology or Medicine in 1937.
Over the past 150 years, akin to the vicissitudes of mood that define the illness, interest in bipolar disorder and its treatment has undergone many ups and downs. During the latter half of the 19th century, and over a similar time span in the 20th century, lithium gradually surfaced in psychiatry and established itself as a therapeutic agent for manic depressive illness. Its initial uptake, by regulatory authorities, was rather slow and it took considerable time, especially in the USA, to become a recognized treatment for bipolar disorder.
Like most baby boomers lithium had its heyday as a mood stabilizer in the 1960s and 70s. Its reign, however, was relatively short-lived because agents that had stronger commercial backing soon eclipsed it. Nevertheless, over the subsequent decades lithium has continued to be used in the treatment of mood disorders and is experiencing a revival, as its neurobiology is better understood and putative neuroprotective effects are realized.
In practice lithium is widely regarded as the uncrowned king among bipolar treatments and is, in effect, the archetypal mood stabilizer. It has endured competition from both the antidepressants and anticonvulsants but is once again being challenged for its royal status. On this occasion it is the atypical antipsychotics that form the charge, with their eager migration into the lucrative mood stabilizer arena. It would seem that over the past 60 years, whenever a new agent purported to have efficacy in the treatment of some aspect of bipolarity, the evidence that supports the use of lithium and forms the throne upon which it sits comes under threat.
This editorial briefly recounts the efforts of the many men that, through their endeavours both individually and collectively, have assigned lithium its unique clinical role and served to sustain its special status (Figure 1).
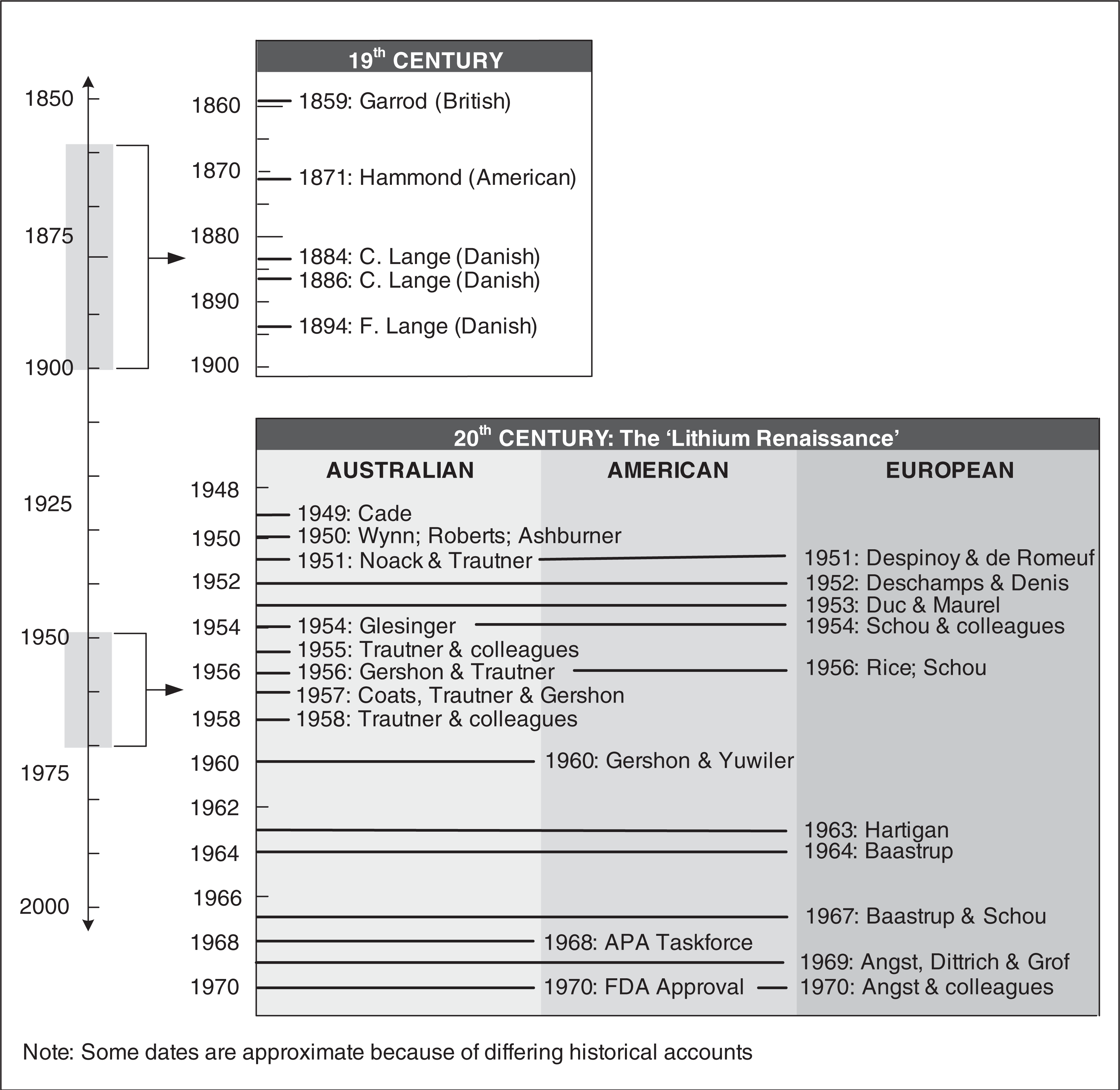
Timeline of key figures in relation to lithium.
Mood disorders in the making
The discoveries that led to the use of lithium in the treatment of mood disorders are inherently difficult to chronicle because of differing historical accounts and variable levels of record keeping and documentation. Inevitably, this has resulted in certain key aspects of the story remaining open to speculation. For instance, the assignment of priority specifically with respect to the mood stabilizing properties of lithium remains somewhat contentious. The issue is further obfuscated by the fact that, since its inception, the definition of the illness has been ever changing and even to this day the taxonomy of bipolarity remains in a state of flux. Hence the ‘bipolar syndrome’ of today is most likely not the same as that described by Kraepelin when referring to ‘manic-depressive insanity’, and probably shares little with cyclothymia as conceptualized by Hecker and Kahlbaum [1,2]. The latter characterized cyclothymia as recurrent episodes of depression or dysthymia interspersed with periods of hypomania or hyperthymia, whereas Kraepelin subsumed most cases of severe, recurrent, episodic melancholic depression, along with mixed states and uncommon cases of recurrent mania, within his group of manic depressive illnesses [3]. Interestingly, it took more than half a century to understand the polarity of mood disorders and it was not until the middle of the 20th century that a subgroup of recurrent unipolar depressive illness was partitioned from bipolar manic depression [4,5]. The latter has subsequently been subdivided into bipolar I and II, on the basis of manic features, and cyclothymia is now used to describe lifelong mood instability [6,7]. In recent years the clinical complexity of bipolar disorder has become increasingly apparent and terms describing admixtures of symptoms (mixed episodes), patterns of cyclicity (rapid cycling, ultradian cycling) along with levels of symptoms that fail to qualify as syndromes (subsyndromal depression) have been coined, and are now used to describe the seemingly myriad presentations of bipolar disorders [8].
Ion men
The discovery of lithium's mood stabilizing properties has been recounted many times [9,10], and a recent monograph that serves as a wonderful reference provides a meticulously detailed account of original reports, opinions and debates concerning the matter [11]. A key issue that has interested psychiatry historians is how lithium came into clinical use. Of particular interest is the exchange of ideas that led to its administration to patients with mood disorders and, more specifically, whether because of prior knowledge certain discoveries can be genuinely regarded as novel insights. The figure at the centre of this controversy is John Cade, born in 1912, in a small town near Melbourne in Australia, called Horsham.
Lithium renaissance
Cade trained in medicine and pursued psychiatry prior to enlisting in World War II, in which he was captured by the Japanese and imprisoned for nearly 4 years. After the war he returned to Melbourne to practise as a psychiatrist and began experiments using guinea pigs to test the properties of urine from psychiatric patients in the belief that there must be a medical basis for psychological disturbances. By observing the effects of urine, injected into the abdomens of the animals, he postulated the existence of a toxic urinary substance that was being excreted by the patients. While attempting to identify the nature of this substance Cade found that lithium produced a psychotropic effect in its own right and speculated that this could perhaps be used to treat psychotic excitement. It is of note that he took lithium himself before administering any to his patients. In the latter he reported that lithium had an antimanic action and suggested that mania may be the result of a deficiency in the body of lithium ions [12].
Cade's seminal paper described only 10 patients, one of whom was described as schizoaffective. Six patients had episodic mania and three had chronic mania but all responded within days to the administration of lithium, with five patients showing sufficient improvement to be eventually discharged from hospital [12]. The effect was profound. The timing of this publication, however, was somewhat unfortunate because it coincided with a lithium fatality thought to have occurred because of cardiotoxicity [13]. The publication of this paper in the same journal as Cade's article, along with others [14], forestalled the use of lithium especially in the USA, where lithium had been recently banned. The concerns as regards toxicity highlighted the need for monitoring lithium treatment and determining a safe dosage.
Victor Wynn, also in Melbourne, in the Department of Physiology at The University of Melbourne, successfully applied the newly developed flame spectrophotometer to determine the levels of potassium and sodium in body fluids [15]. Edward Trautner, in the same department as Wynn, along with a psychiatry colleague Charles Noack, administered lithium in a treatment trial to 100 patients and, in addition to reporting an antimanic effect, developed indicators for safe lithium levels [16]. This was an important paper because at the time it presented the largest clinical experience with lithium and raised the possibility of a specific antimanic action. Further, along with other Australian publications [17], it was influential in promoting the use of lithium. Trautner and colleagues, which included Samuel Gershon, adopted the use of lithium assays and began examining the disposition of lithium in a series of important studies [18]. In a paper entitled ‘The excretion and retention of ingested lithium and its effect on the ionic balance of man’ that detailed the use of the spectrophotometric assay of lithium, the authors suggested that lithium may possess some pharmacological specificity for ‘typical’ cases of mania [18,19]. Similarly, another paper, published in 1956 by Gershon and Trautner, alluded to its prophylactic potential but the issue of lithium specificity was engulfed by a greater interest in its safety and tolerability [20]. A number of Australian studies at the time examined and reported on lithium toxicity [21] and even investigated its potential teratogenicity in rats [22].
The response in the UK to Cade's publication was modest and slow, with the first British report of lithium use for the effective treatment of mania appearing in 1956 [23]. The greatest interest in Cade's paper, immediately following its publication, was seen in France. A number of reports corroborating Cade's findings appeared in successive years [24–26], but in France lithium was competing with chlorpromazine, which had the advantage of both pharmaceutical backing and the potential to provide a platform for the development of other molecules. The interest in lithium was therefore not sustained and only a few reports, which included two Czech and two Italian articles, were published during this time [27]. Having recently migrated from the hub of lithium research in Australia, Samuel Gershon published the first article on lithium therapy for mania in the USA [28]. Following this, however, few other US publications emerged and there was a noticeable hiatus of almost a decade.
In the meantime, the Danish psychiatrist Mogens Schou, born in Copenhagen in 1918, came under the tutelage of Eric Stromgren. Stromgren brought Cade's findings to the attention of Schou and facilitated his interest in the evaluation of lithium. Schou conducted a rigorous placebo-controlled trial and found that patients with chronic mania improved on lithium but deteriorated when switched to placebo. Further, those with a pattern of recurrent illness showed sustained improvement when maintained on lithium [29,30]. Through his work Schou managed to cultivate research connections at home and overseas with Poul Baastrup from Denmark and Toby Hartigan from Britain, respectively. Collectively through a series of studies they showed that lithium had prophylactic properties and that it benefited those with recurrent affective illnesses [31–33]. Despite these promising insights that occurred early and over a relatively short period of time, the progress of Schou's lithium research was constricted by resistance from Michael Shepherd and colleagues based in the Institute of Psychiatry in London. Criticisms of their studies as regards their methodological validity and findings thwarted advancement until, assisted by Jules Angst and Paul Grof, the group was able to show in controlled trials that lithium administration reduced the frequency of affective episodes [34,35]. Finally, lithium had arrived, not as an antimanic agent but as a mood stabilizer.
Across different countries lithium had entered into quiescence for different reasons. In the USA Samuel Gershon did for lithium what Schou had achieved in Europe. As a member of the lithium task force appointed by the American Psychiatric Association in 1969, Gershon along with Biff Bunney, Joseph Tupin and Robert Prien sought approval for the use of lithium for mania. Publications by these researchers and others, who included Ronald Fieve and Fred Goodwin to name but a few, ultimately persuaded the Food and Drug Administration to approve lithium for the treatment of mania. Interestingly, lithium was not approved for prophylaxis, but because of its demonstrated specificity [19] it was affecting diagnostic classifications and led in part to the separation of bipolar disorder from other mood disorders. Further, its differential activity across bipolar and unipolar depression prompted a re-evaluation of bipolar disorder that contributed to the conception of bipolar II disorder.
Birth of therapeutic lithium
It is difficult from the vantage point of the 21st century to fully appreciate the context within which early practitioners of medicine operated. Physiological and anatomical knowledge was basic at best and models of disease were rudimentary if they existed, and usually incorrect. Having been identified in the first half of the 19th century as an alkali metal, lithium was widely used as a medicinal additive to create alkaline solutions. Spas, used routinely at the time to treat rheumatic conditions and gout, were usually alkaline and many had been found to contain lithium. Hence, lithium was readily available and thought to be of benefit for a wide variety of health-related conditions.
Alfred Garrod in 1859 reported that lithium, while being administered to treat gout, produced a more general sense of well-being [36]. Similarly, in the USA, Silas Weir Mitchell noted that the use of lithium bromide when treating epilepsy in addition improved aspects of personality and conferred a sense of generally feeling well [37]. In 1871 William Hammond made a more specific comment, suggesting that lithium was perhaps a useful agent for nervous states [38]. Thus, in the latter half of the 19th century the possibility that lithium possessed psychotropic properties was being entertained and communicated and this set the stage for the Lange brothers.
Carl George Lange, born in Copenhagen in 1834, studied medicine and became Denmark's first neurologist. At the same time as Hughlings Jackson he described aphasia and made a number of key neurological discoveries for which he receives little recognition, having published in Danish. He is best known for his contribution to the James–Lange theory of emotions (1885) [39] but in the context of the current discussion his major contribution came in 1886 in a key paper that describes the treatment of melancholic depression with lithium and characterized a ‘new illness’, namely, periodical depression [40]. Taking his cue from Carl, his elder brother Frederick, who was in charge of an asylum in Middelfart, administered lithium to depressed patients using doses similar to those prescribed today and reported the benefits of lithium therapy, noting that, upon initiating treatment, responses occurred within a matter of weeks [40].
Unfortunately for those interested in lithium, as the century ticked over so too the focus of medicine changed dramatically, with a wholesale shift towards specificity of action both medically and surgically on the basis of developments in bacteriology and anaesthesiology [41].
Lithium's legacy
The story of how lithium came into clinical use for the treatment of mood disorders is complicated [42], and one that clearly involved many individuals over a span of nearly two centuries. Each and every one needs to be credited for their contribution to the discovery of lithium's unique properties and hence this editorial on the 60th anniversary of Cade's paper. To this day, lithium continues to baffle and inform with respect to its chemical properties, clinical actions and impact on brain functioning. It is important to acknowledge, however, that lithium continues to provide an essential function as the gold standard for the management of bipolar disorder and that throughout its history it has served to both define the illness and those who have attempted to understand its properties.
Footnotes
Acknowledgements
The authors acknowledge the NHMRC Program Grant (510135) for essential financial support. In the past 3 years Professor Gin Malhi has served on a number of international and national pharmaceutical advisory boards, received funding for research and has been in receipt of honoraria for talks at sponsored meetings worldwide involving the following companies: Astra Zeneca, Eli Lilly, Jansen-Cilag, Organon, Pfizer, and Wyeth.