
Abstract
Stevioside (250-mg capsules) was given thrice daily for 3 days to 10 healthy subjects. Blood samples were collected and blood pressure measured after nocturnal fasting, before and at different time points during the third day of the administration of stevioside. No significant differences were found between the control and the stevioside condition for blood pressure and blood biochemical parameters. The 24-hr urinary volume and urinary excretion of electrolytes were not significantly different. Likewise, no significant difference was found for mean blood glucose and insulin between control and stevioside conditions. Thus, oral stevioside is not directly effective as a hypotensive or hypoglycemic agent in healthy subjects at the dose administered in this study.
Stevioside, free steviol, and steviol metabolites were analyzed in blood, feces, and urine after 3 days of stevioside administration. No uptake was found of stevioside by the gastrointestinal tract or the amounts taken up were very low and below the detection limit of the UV detector. Stomach juice did not degrade stevioside. All the stevioside reaching the colon was degraded by micro-organisms into steviol, the only metabolite found in feces. In blood plasma, no stevioside, no free steviol or other free steviol metabolites were found. However, steviol glucuronide (SV glu) was found in maximum concentrations of 33 μg/ml (21.3 μg steviol equivalents/ml). In urine, no stevioside or free steviol were present, but SV glu was found in amounts of up to 318 mg/24-hr urine (205 mg steviol equivalents/24 hrs). No other steviol derivatives were detected. In feces, besides free steviol, no other steviol metabolites or conjugates were detected. Steviol was excreted as SV glu in urine.
Introduction
The natural sweetener stevioside is a diterpene glycoside extracted from the plant Stevia rebaudiana (Bertoni) Bertoni that belongs to the Asteraceae family and is native to Brazil and Paraguay. Stevioside tastes about 300 times sweeter than 0.4 M sucrose and is noncaloric. In some parts of the world, including Japan, South Korea, Israel, Mexico, Paraguay, Brazil, Argentina, and Switzerland, stevioside is used to sweeten food products and beverages. In the USA, powdered Stevia leaves and refined extracts from the leaves have been used as a dietary supplement since 1995 (1).
It has been reported that both stevioside and aqueous extracts of Stevia induce direct blood pressure reduction in hypertensive rats (2) and anesthetized dogs (3). In addition, increased diuresis and natriuresis were observed during infusion experiments on male Wistar rats with both normal and experimental renal hypertension (4, 5). The hypotensive effects were confirmed in double-blind, placebo-controlled studies in Chinese hypertensive men and women taking 750 mg (6) or 1500 mg (7) of stevioside a day for 1 (6) or 2 years (7). In both studies, the systolic and diastolic blood pressure of the stevioside group was significantly lower (about 7%). The blood pressure–lowering effect persisted throughout the whole study (6, 7). In vitro studies with incubated mouse pancreatic islets have indicated that hypoglycemic effects of stevioside and steviol result from the stimulation of insulin secretion via direct action of these compounds on β-cells and the β-cell line INS-1 (8). Long-term human administration studies did not reveal effects of stevioside on fasting glucose concentrations in hypertensive volunteers with normal glucose levels (6, 7).
Steviol, the aglycone of stevioside and other steviol glycosides occurring in Stevia rebaudiana (Bertoni) Bertoni, is still a controversial metabolite. Weak mutagenic effects of steviol and/or its metabolites were reported in the forward mutation assay using the very sensitive Salmonella typhimurium TM677 (9–13). After metabolic activation, it was shown that so far unknown steviol metabolites caused mutations in S. typhimurium TM677, that is, transitions, transversions, duplications, and deletions at the guanine phosphoribosyltransferase (gpt) gene (14). However, stevioside and steviol were inactive in various TA strains of S. typhimurium, Escherichia coli WP2 uvrA/pKM101 and the rec-assay using Bacillus subtilis even when activation S9 mix was present (11, 15). The activity of steviol in S. typhimurium TM677 was very low and was only about 1/3,000 that of 3,4-benzopyrene, and that of steviol methyl ester 8,13 lactone, a synthetic compound, was 1/24,500 that of furylfuramide (13). Although a weak activity of steviol and some of its derivatives was found in the very sensitive S. typhimurium TM677 strain, the authors concluded that the daily use of stevioside as a sweetener is safe. Moreover, the presence in the blood of the chemically synthesized steviol derivatives after orally feeding stevioside is not proven at all. The genotoxicity of steviol (>99% purity) was evaluated using the comet assay, in which DNA damage is detected by DNA strand breaks and alkali-labile sites (16). Steviol was evaluated in vitro and in vivo. With in vitro experiments, comet assays were done in the human lymphoblastoid cell lines TK6 and WTK-1. No statistically significant differences in DNA damage were observed at concentrations of 500 μg/ml or below, either with or without metabolic activation. In in vivo studies, steviol was administered to BDF1 or CRJ:CD1 mice as one oral dose at 250, 500, 1000, and 2000 mg/kg. Three and 24 hrs after gavage, DNA was assessed in the liver, kidneys, stomach, colon, and testes. No statistically significant differences in DNA damage were observed in any of the organs of animals to which steviol was administered (16). After chronic oral administration of steviol to hamsters for 22 (males, up to 199 mg/kg body wt) or 18 months (females, up to 183 mg/kg body wt), no treatment-related changes could be observed in any organ or tissue (17).
It was shown that oral stevioside and rebaudioside A were not taken up by the human body or the uptake was extremely low (18, 19), and none of the digestive enzymes from the gastrointestinal tract of different animals and man were able to degrade stevioside into steviol, the aglycone of stevioside (18, 20). Nevertheless, the bacterial flora of the rat cecum converts stevioside and rebaudioside A into steviol (21). In feeding experiments with rats and hamsters, stevioside was metabolized to steviol by the bacterial flora of the cecum and free steviol was found in the blood of the animals, with the maximum concentration occurring after 8 hrs (22, 23). Bacteria isolated from the human colon were able to transform stevioside into steviol in vitro (20, 23, 24). In vivo stevioside degradation to steviol occurred by bacterial action in the colon of pigs (19) and humans (25). Among the selected intestinal groups, bacteroidaceae were the most efficient in hydrolyzing Stevia sweeteners to steviol (24). Studies with roosters (26) and chickens (laying hens and broilers) (27) indicated that stevioside was rapidly eliminated from the body, largely untransformed. Contrary to these results, in the colon of pigs and humans, oral stevioside was completely degraded into steviol, which was found to be the only metabolite in the feces (19, 25, 28). However, no stevioside or free steviol were found in the blood of the animals (19, 27).
In its 63rd meeting (8–17 June 2004), the Joint Food and Agriculture Organization/World Health Organization Expert Committee for Food Additives (JECFA) evaluated the safety of stevioside and its metabolism. A temporary allowable daily intake (ADI) of 0–2 mg steviol equivalents/kg body weight has been suggested (29). However, the Food and Drug Administration (USA), European Food Safety Agency (EU), and Food Standards Australia, New Zealand (Australia and New Zealand) do not accept this temporary ADI.
Recently, steviol glucuronide (SV glu) was positively identified in urine after oral stevioside administration (30). So far, no extended metabolism studies of oral stevioside in human volunteers have been published, and experimental evidence from human trials on the effects of stevioside on blood pressure and plasma glucose concentrations is scarce. Therefore, the aim of the present experiments with healthy volunteers was to study the metabolism and fate of oral stevioside. In addition, blood pressure and plasma glucose and insulin concentrations were measured.
Methods and Material
Chemicals.
The experiments were performed using commercial stevioside
([19-O-β-glucopyranosyl-13-O-(β-glucopyranosyl(1→2)-β-
Subjects.
To be included in this study, subjects had to be between 18 and 40 years old, be healthy as assessed by a medical questionnaire, and possess an easy blood take, and women could not be pregnant, as determined from a pregnancy test at the beginning of the investigation. Persons using medication known to affect the blood pressure and those with diabetes were excluded (this was assessed by determining glucose in a urine sample and by the medical questionnaire). Before the start of the study, weight and height of the subjects were measured.
Ten healthy volunteers (5 female, 5 male) participated in the study. The volunteers were all between 21 and 29 years old. The women were on average 23 ± 1 years old and 172 ± 5 cm tall and weighed 65 ± 7 kg. The men were on average 26 ± 2 years old and 175 ± 5 cm tall and weighed 74 ± 11 kg. Subjects’ body mass index (BMI) averaged 23.1 ± 0.9 kg/m2.
Study Design.
After the selection procedure, the volunteers collected a 24-hr control urine. On the first day, a fasting blood sample was taken and fasting blood pressure measurements were done before the ingestion of the first capsule. Then, capsules with 250 mg stevioside were given to the subjects three times a day at 8-hr intervals for a period of 3 days. This dose is far above the daily maximum amount needed as a sweetener and is equal to that used in a study on hypertension (6). The volunteers were instructed to take the capsules with a glass of water. On the third day of the experiment, the volunteers received a standardized breakfast, lunch, and dinner and were asked to drink only water, tea or coffee. On the third day, six blood samples (2 × 4 ml) were taken before breakfast and before the first stevioside dose (0 hrs), and after breakfast and the first stevioside dose (at 0.5, 1, 3, 5, and 7 hrs). Blood pressures were also measured six times (before and 30, 60, 90, 120, and 180 mins after the first dose). On this third day the volunteers were asked to collect a 24-hr urine sample (stevioside urine). A 24-hr feces sample was collected on the fourth day of the experiment. The urine and feces samples were immediately delivered to the laboratory. The urine volume was measured and the analysis started immediately. The feces sample was weighed and samples of 20 g fresh weight were frozen in solid CO2 and then freeze dried. In addition, every subject was asked to give three fasting control blood samples (before and 30 and 60 mins after drinking a glass of water) and to do five control blood pressure measurements (before and 30, 60, 90, and 120 mins after drinking a glass of water). For logistic reasons, the control clinical measurements were done on each subject 3 weeks after the stevioside test. The Medical Ethical Committee of the University Hospital Gasthuisberg Leuven approved the study protocol ML2196. After the purpose of this study was explained to the volunteers, all gave written informed consent to the protocol.
Clinical Analyses.
Systolic (SBP) and diastolic (DBP) blood pressures were measured using an automatic, validated device (OMRON M5-I; Omron Healthcare Europe BV, Hoofddorp, the Netherlands). The measurements were always made in the same room by the same technician. The subjects were in a sitting position for at least 10 min before the measurement and were not allowed to speak or move. The blood pressure was measured three consecutive times with intervals of 1 min; the mean of the three measurements was used in the analysis.
Blood samples were taken in 4-ml tubes containing heparin. Samples were then centrifuged (10 min, 3000 rpm) and plasma divided into aliquots of 700 μl and frozen immediately (−80°C). The plasma glucose level was determined by the hexokinase method (32, 33). Plasma insulin was analyzed by microparticle enzyme immunoassay (MEIA; Abbott, Wiesbaden, Germany). In addition, several markers for tissue damage were analyzed. Alkaline phosphatase (IL Test Alkaline Phosphatase; Instrumentation Laboratory, Milano, Italy), alanine aminotransferase (ALT) and glutamic pyruvate transaminase (GPT) (IL Test ALT/GPT, Instrumentation Laboratory), creatine kinase (IL Test CK-NAC, Instrumentation Laboratory), and lactate dehydrogenase (IL Test LDH-P, Instrumentation Laboratory, Milano, Italy) were analyzed by colorimetric methods. To two blood plasma samples of 700 μL, 4 μg internal standard (IS) was added. Then the samples were stored at −20°C for later analysis of steviol and stevioside.
From the 24-hr control and stevioside urine, 20 ml was taken for the detection of different markers. Creatinine was determined using the Jaffé method (34). Sodium and potassium were detected by indirect potentiometric determination by means of ion-selective electrodes. For the calcium determination, a complexometric method was used, based on the reaction of calcium with o-cresol-phthalein complexone in alkaline solution (35). For the analysis of urea a kinetic UV assay was applied based on the coupled urease/glutamate dehydrogenase enzyme system (36).
Urine Analysis.
The total 24-hr urine fraction (between 1124 and 2494 ml) was run over an Amberlite XAD-2 column (Sigma) at about 30 ml/min. The column bed volume was 200 ml, which is sufficient for the adsorption of all amphipathic molecules of a 24-hr urine. 1 The columns were then rinsed with 1 liter of distilled water and then eluted with 400 ml MeOH:acetone (50:50, v/v). The eluate was divided into 4 equal fractions and the solvent was evaporated by use of a rotavapor at 50°C. The dry weight of the fractions was recorded.
Geuns et al., unpublished, June 2003.
Analysis of Free Steviol and Stevioside.
Fraction 1 was dissolved in 10 ml MeOH/acetone (50:50, v/v) and samples of 250 μl were pipetted off for free steviol determination. After the addition of 4 μg dihydroisosteviol as IS (37), the sample was completely dried and dissolved in 100 μl MeOH, and diluted with 500 μl acetate buffer, pH 5. This solution was purified on C18 cartridges of 500 mg (Alltech, Lokeren, Belgium). Before use, the cartridges were conditioned by rinsing with 3 ml MeOH, followed by 3 ml of distilled water. After application of the sample in MeOH/buffer (100:500), the columns were rinsed with 3 ml 20% MeOH in water and 3 ml 50% MeOH in water. Then the steviol and IS–containing fraction was eluted from the column with 5 ml MeOH. This fraction was evaporated to complete dryness and dissolved in dry acetone. This aprotic solvent is necessary for a complete esterification of the free carboxyl group with 4-(bromomethyl)-7-methoxycoumarin to the 7-methoxy coumarinyl ester of steviol and IS. HPLC analysis was on a C18 column as described (37): column 250 × 4.6 mm C18, 5 μm, Alltech; isocratic flow of MeCN/H2O (80:20); fluorimetric detection, λexcitation = 321 nm, λemission = 391 nm; detection limit, 100 pg). The recovery of steviol and IS was around 65% after sample cleanup. However, the ratio of steviol to IS did not change significantly, implying that the losses of steviol were adequately corrected for by the internal standard (37).
Samples of Fraction 2 were treated as above for stevioside analysis. For this purpose, the dried residue after C18 cartridge purification was dissolved in 0.2 ml EtOH containing 3% diethyl ether and 10 μl samples were injected onto the HPLC column (250 × 4.6 mm C18, Alltech; isocratic flow of MeCN/H2O (35:65); UV detection at 210 nm; detection limit: 50 ng). Recovery of stevioside was around 75%.
Analysis of Bound Steviol.
Steviol possibly bound to glucuronides and sulfates was obtained by β-glucuronidase/sulfatase from Helix pomatia digestive juice. Steviol was measured after derivatization to its 7-methoxycoumarinyl ester, because this could be measured more sensitively by a fluorescence detector. Urine fraction 3 was dissolved in 10 ml MeOH/acetone (50:50), and to samples of 250 μl, 200 μg of IS were added. The samples were then evaporated and dissolved into 500 μl acetate buffer, pH 5. Then 50 μl β-glucuronidase/sulfatase was added (5000 and 375 U respectively). The mixture was incubated for 6 hrs at 37°C. Under these conditions, a complete conversion to steviol occurred. After hydrolysis the samples were purified on C18 cartridges (500 μl bed volume, Alltech) that were conditioned before use with 3 ml MeOH followed by 3 ml H2O. After application of the enzyme mixtures, the columns were rinsed with 3 ml water and 3 ml 50% MeOH. The steviol and IS were eluted with 5 ml MeOH. Of this last fraction, 250 μl was evaporated under a stream of nitrogen at 50°C. The completely dried residue was then derivatized in dry acetone to the 7-methoxy-coumarinyl ester as described above. After reaction, the samples were purified by thin layer chromatography (TLC) on silica gel in CHCl3:MeOH (98:2). The blue fluorescing band of the derivatives under UV 366 nm was scraped off and eluted with CHCl3/MeOH (80:20). After evaporation of the solvent, the residue was dissolved in a known amount of MeOH and analyzed by HPLC as above. The identity of the steviol 7-methoxy coumarinyl ester was checked by mass spectrometry (MS). Recovery of steviol was as above.
Blood Analysis.
Free Steviol and Stevioside.
The first series of the 700-μl fractions was acidified to pH 6 with 6 N acetic acid and then extracted three times with equal volumes of peroxide-free diethyl ether. The ether fraction was completely dried and the 7-methoxy coumarinyl esters were made in dry acetone and analyzed as described above. The lower water phase of the plasma was quantitatively applied to a preconditioned 500-mg C18 cartridge (Alltech) that was rinsed with 5 ml 40% MeOH. If present, stevioside and steviolbioside can be eluted with 3 ml of a 90% MeOH solution as shown with standards. The extracts were evaporated at 50°C under a flow of nitrogen and the residues were redissolved in 0.2 ml of EtOH containing 3% diethyl ether. Extracts of blood samples needed purification by TLC on silica gel with ethyl acetate/EtOH/water (130:27:20) as solvent. The bands occurring between the spots of stevioside standards at both sides of the TLC plates (Rf = 0.20) were eluted with MeOH, which was again evaporated in HPLC sample vials and dissolved in 0.2 ml of EtOH containing 3% diethyl ether, of which 10 μl were injected onto the HPLC column for stevioside quantification as described previously.
Conjugated Steviol.
The second series of 700-μl fractions was hydrolyzed after the addition of 1 ml acetate buffer, pH, 5.0, and 50 μl β-glucuronidase/sulfatase (5000 and 375 U respectively). The mixture was incubated at 37°C for 6 hrs. After incubation, the samples were extracted three times with 2 ml diethyl ether. The combined ether fraction was completely dried at 50°C under a flow of N2. Then, 7-methoxy coumarinyl esters were prepared and analyzed as described above.
Feces Analysis.
Stevioside Determination.
Weighed aliquots of about 100 mg of powdered excreta pulverized in a Retsch mixer mill (MM200; Labo Service, Kontich, Belgium),were extracted with MeOH (4 × 1 ml). Then, 6 ml H2O was added to the pooled extract fractions and the solution was acidified with HCl to pH 6.5 to facilitate the binding of possible acid metabolites (steviol and steviolbio-side) onto C18 cartridges. This solution was quantitatively applied to a conditioned 500-mg C18 cartridge (Alltech) that was rinsed with 5 ml 40% MeOH. If present, stevioside and steviolbioside can be eluted with 3 ml of a 90% MeOH solution. The extracts were evaporated at 50°C under a flow of nitrogen and the residues were redissolved in 0.2 ml of EtOH containing 3% diethyl ether. Extracts of excreta samples could be directly injected onto the HPLC column for stevioside and steviolbioside quantification as described previously.
Free Steviol.
To weighed samples of about 25 mg dried and powdered feces, 4 μg IS was added and then the sample was extracted with acetone (4 × 1 ml). The extracts were concentrated and purified by TLC on silica gel (CHCl3/MeOH, 90:10). The bands corresponding to standards of steviol and IS (Rf = 0.35, visualized under UV of 366 nm) were eluted with CHCl3/MeOH (50:50) and the solvent completely evaporated under a stream of nitrogen (traces of water interfere with the subsequent derivatization reaction). The residue was derivatized by esterification of the free carboxyl group with 4-(bromomethyl)-7-methox-ycoumarin and chromatographic analysis was as above.
Conjugated Steviol.
To weighed samples of about 25 mg dried and powdered feces, 4 μg IS was added and then the sample was extracted with acetone/MeOH (50:50; 4 × 1 ml). The extracts were evaporated under a stream of N2 at 50°C. To the residues, 1 ml acetate buffer pH 5.0 and 50 μl β-glucuronidase/sulfatase (5000 and 375 U respectively) were added. The mixture was incubated at 37°C for 6 hrs. After incubation the samples were extracted three times with 2 ml diethyl ether. The combined ether fraction was completely dried at 50°C under a flow of N2, and 7-methoxy coumarinyl esters were prepared and analyzed as described above.
Incubation of Stevioside in Stomach Juice.
Stevioside was incubated in 3 freshly taken samples (intubation) of stomach juice at 37°C for 6 hrs (1 mg/ml). At 0 hrs and after 2, 4, and 6 hrs samples were taken and directly analyzed by HPLC as described previously.
Statistical Analysis.
Data were analyzed using the General Linear Models procedure of SAS (SAS software, version 8.1; SAS Institute, Inc., Cary, NC) to test differences between stevioside and control groups with repeated measurements for the different time points. Results are expressed as mean ± SEM. Differences were considered statistically significant when the P value was less than 0.05.
Results
Clinical Observations.
As one of the male volunteers did not return after the first week of the experiment, the results of the clinical study were limited to 9 volunteers. The fasting glucose concentrations fluctuated around 4.60 mM for the control and 4.63 mM for the stevioside condition (Table 1). The insulin concentration was on average 5.6 mU/liter for the control and 5.9 mU/liter for the stevioside condition, with no significant differences between them. The SBP/DBP fluctuated around 114/74 mm Hg for the control and around 115/72 mm Hg for the stevioside condition, and again, differences were not significant. The volume of 24-hr urine samples averaged 36% higher after the stevioside intake (1561 ± 489 ml) compared to the control condition (1150 ± 488 ml). However, this difference did not reach statistical significance (P = 0.06) because of the large interindividual variations. No significant differences were detected in electrolytes excreted in the 24-hr urine (Table 2). There were no indications of tissue damage as the values for 4 indicators (alkaline phosphatase, alanine aminotransferase, glutamic pyruvate transaminase, and creatine kinase; Table 2) were within normal ranges. No breakdown of stevioside occurred after 6 hrs of incubation in stomach juice at 37°C (results not shown).
No differences because of the sex of the volunteers were observed. Therefore, no further consideration will be given to the sex of the subjects.
Blood Analyses.
No stevioside or free steviol could be detected in the blood samples at any time of the experimental period (results not shown). However, after enzymatic hydrolysis by β-glucuronidase/sulfatase, steviol could be detected in concentrations ranging from 0.7 to 21.3 μg/ml plasma (Table 3). From Table 3 it can be seen that the metabolism in different volunteers was quite different and that the maximum steviol conjugate concentration in the plasma occurred at different periods after stevioside administration. As an example, Figure 1 shows the steviol (SV) concentration set free out of SV glu of Volunteer 1. In two volunteers no clear maximum could be discerned (Table 3, numbers 8 and 9). Because the maximum conjugate concentrations of different volunteers occurred at different periods, the mean at each data point was fluctuating around 5.65 μg/ml plasma. Blood analyses were done during the first 8 hrs of Day 3, whereas urine and feces were collected during 24 hrs, that is, after 2 additional doses of stevioside. Therefore, the maximum amounts of steviol found in SV glu (Table 3) were multiplied by 3 to estimate the total amounts of steviol found in SV glu in the plasma over the 24-hr period (Table 4). The plasma volume was estimated assuming that blood volume was about 7% of body weight, and plasma volume about 50% of blood volume.
Urine Analyses.
No stevioside or free steviol were detected in urine samples (results not shown). However, after enzymatic hydrolysis by β-glucuronidase/sulfatase, high levels of steviol could be detected ranging from 28 (No. 7) to 205 mg (No. 6) per 24-hr urine, being between 43.4 and 318 mg SV glu/24-hr urine (Table 4). Figure 2 shows an example of a chromatogram of the 7-methox-ycoumarinyl ester of steviol found after enzymatic hydrolysis of urine samples.
Feces Analyses.
No stevioside or steviol conjugates were detected in the feces samples. However, the amounts of free steviol ranged from 13 to 40 mg in a 24-hr feces (Table 4).
Of the daily dose of 750 mg stevioside, theoretically about 300 mg free steviol could be produced by bacteria in the colon. The total recovery of steviol calculated as the sum of the amounts found in blood, urine, and feces varied between 109.4 and 304.1 mg or between 36.5% and 101.4% with an average recovery of 75.5% ± 7.8% (Table 4), which is similar to the methodologic recovery.
Discussion
This study showed that 3 days of oral stevioside administration (750 mg per day) affected neither the systolic or diastolic blood pressure nor the fasting plasma glucose and insulin concentrations of healthy volunteers. Animal experiments with hypertensive rats (2) and anesthesized dogs (3) showed that the effects of stevioside, when administered intravenously, were direct and dose dependent. With 50 mg stevioside/kg, small but significant reductions of arterial blood pressure were obtained after less than 10 minutes in hypertensive rats (2). Other investigators reported blood pressure–lowering effects in normal and hypertensive rats after intravenous administration of 16 mg/kg body wt (5). The maximal reduction of blood pressure (around 30%) was obtained with the highest dose of 200 mg/kg (2). Nasogastric administration of 200 mg stevioside/kg was less effective and slower than intravenous administration, but this very high dose still resulted in a significant blood pressure lowering by 9% after 60 minutes in healthy mongrel dogs (3). In our study, dosages of stevioside were around 10–15 mg/kg per day, and were administered orally to human volunteers with normal blood pressures. Therefore, the dosage was probably too low and/or the period too short to expect direct effects using this method of administration. The latter reason is supported by the chronic intervention studies, which reported significant hypotensive effects in hypertensive subjects with a similar dosage of stevioside after 2 weeks of administration (6) and with a larger dose after 1 week (7). One of the mechanisms proposed for the hypotensive effects of stevioside is the direct action of stevioside or its metabolites on renal function. Intravenously administered stevioside (16 mg/kg) in rats increased water, sodium, and potassium excretion (4). This suggested a vasodilating effect on the kidney, which could eventually result in blood pressure reduction. It is not known whether these effects would occur after oral administration, as the uptake of stevioside is extremely low (18, 19). It is further proposed (4, 5) that the vasodilating action of stevioside depends on the blocking of calcium channels similar to the action of verapamil. By this mechanism, calcium influx of the smooth muscle cells is inhibited, resulting in vasodilating effects (3).
Stevioside and other steviol glycosides might also influence carbohydrate metabolism and induce hypoglycemic effects, especially after a glucose load, as has been observed in diabetic Goto-Kakizaki rats (38) and streptozotocin (STZ)- or fructose-induced diabetic male Wistar rats (39, 40), as well as in human experiments (41, 42). It was shown that stevioside increased whole-body insulin sensitivity, and low concentrations (0.01–0.1 mM) modestly improved in vitro insulin action on skeletal muscle glucose transport in both lean and obese Zucker rats, indicating a potential site of action of stevioside in the skeletal muscle glucose transport system (43). In STZ-induced diabetic Wistar rats, stevioside enhanced insulin secretion as well as insulin sensitivity because of a decreased phosphoenol pyruvate carboxokinase gene expression in the liver slowing down gluconeagenesis (40). Our study indicated that orally administered stevioside did not induce direct effects on the fasting plasma glucose or insulin concentrations in humans. In studies with Chinese hypertensive volunteers, no significant change was observed in the fasting glucose concentrations (6, 7). Whether stevioside affects blood glucose levels in healthy volunteers needs to be investigated in further experiments looking at postprandial effects. This study demonstrated that oral stevioside, administered for 3 days in three doses of 250 mg, is not directly effective as a hypotensive or hypoglycemic agent in healthy subjects, and it has no health-compromising effects.
Because of its molecular size, the uptake of stevioside by the intestinal tract is expected to be extremely low, as suggested by experiments with everted gastrointestinal sacs of rats (18) and Caco-2 cell layers (19). Stevioside was not degraded by the digestive enzymes from the gastrointestinal tract of different animals and man (20, 23, 25) nor by the acid conditions of the stomach. In contrast to our observations, by use of liquid chromatography-MS (LC-MS) (selected ion monitoring [SIM]) very low stevioside concentrations were found in blood plasma (0.1 μg/ml), with a large interindividual variation (25). However, most of the stevioside administered is degraded by bacteria of the colon, resulting in free steviol that is easily absorbed (18–22). Between 13 and 40 mg free steviol could be detected in a 24-hr feces collection. The lack of stevioside in the feces proves that the bacterial flora degraded all the stevioside into steviol, which itself was not further metabolized, as also shown in pigs in vivo (19) and in pig and human feces in vitro under anaerobic conditions (19, 23, 24). These results are opposite to those obtained with chickens in in vivo and in vitro experiments, which demonstrated that not all of the stevioside was degraded into steviol (26, 27). In the human colon, only the group of bacteroidaceae were efficient in hydrolyzing stevioside into steviol (24). However, in our experiments, no free steviol could be detected in the blood or the urine of the volunteers. These results are in agreement with the lack of free steviol in chicken or pig blood (19, 27). These results are also in agreement with the metabolism studies recently performed with 9 volunteers by Simonetti et al. who, by use of LC-MS, also failed to detect free steviol in blood and urine (25). To demonstrate the presence of stevioside or free steviol, it might be possible that higher doses than 750 mg have to be administered.
After enzymatic hydrolysis by β-glucuronidase/sulfatase, steviol could be set free out of the SV glu that was the only conjugate detected in urine (30). The amounts of steviol obtained after enzymatic hydrolysis in plasma varied between the different subjects, showing values between 0.7 and 21.3 μg/ml plasma in the period between 0 and 7 hrs after the first dose on the third day. In the different volunteers the maximum amounts occurred at different times after the stevioside dose, a variability that is quite normal in metabolism studies.
The portal blood could not be analyzed in our experimental setup, but it possibly contained free steviol directly taken up from the colon. The presence of free steviol in portal blood of rats fed free steviol (45 mg/kg body wt) was demonstrated (18). The highest concentration (18.3 μg/ml) occurred at the first sampling time (15 min) and then sharply declined, demonstrating that steviol is easily absorbed (18, 19). Free steviol or steviol conjugates were not analyzed in the peripheral blood of the rats. The absence of free steviol in the peripheral blood of the volunteers and the presence of conjugated forms suggest that all free steviol occurring in the portal blood was converted into SV glu by the liver, as also shown by (25).
No free steviol was detected in urine. After enzymatic hydrolysis of urine extracts by β-glucuronidase/sulfatase, steviol was found as the only aglycone present. There was no indication for the occurrence of, for example, steviol sulfates, even after large scale extractions of urine (30). From in vitro incubations of steviol with human liver microsomes, it was concluded that the transformation of steviol by human microsomes was very low and about 4 times lower than that by rat microsomes (18). As no other metabolites were found, the following excretion route is suggested (Fig. 3). After degradation of stevioside to steviol by bacteria of the colon, part of the steviol is absorbed by the colon and transported to the liver by portal blood. In the liver, the SV glu is formed; it is released into the blood and filtered out by the kidneys into the urine. The high levels of SV glu in the urine suggest that there is no accumulation of steviol derivatives in the human body. The SV glu present in the blood is expected to be excreted in the urine during the next 24 hrs. It is known that glucuronide formation easily happens in the liver, and this is also the case with soy isoflavones that, after uptake, were metabolized to compounds that were hydrolyzable with a combined β-glucuronidase and sulfatase enzyme preparation (44).
Besides SV glu, no free steviol or any other of the possible steviol metabolites could be detected in blood or urine, proving that the hepatic metabolism of steviol is extremely low, if it exists at all. This is in agreement with the results of (18), a study that demonstrated in in vitro experiments that the steviol metabolism by human microsomes was 4 times lower than that of rat microsomes, and the latter was already very low.
High doses of oral stevioside lower blood pressure in hypertensive patients (6, 7) and might be used to lower blood glucose levels in type 2 diabetes (38). However, it is not proven that oral stevioside itself is the active compound leading to these effects. Our results demonstrated that no stevioside or free steviol were detected in blood plasma. Therefore, it should be investigated whether SV glu is the active principle after oral stevioside administration.
Plasma Glucose, Insulin, SBP, and DBP, Measured on the Third Day of the Experiment Before and After Stevioside Administration a
Clinical Blood Chemistry Parameters Before and After Stevioside Administration a
Steviol a Found After Enzymatic Hydrolysis by β-Glucuronidase/Sulfatase of Blood Plasma of 10 Volunteers
Weight, BMI, Estimated Total Plasma Volume, Total SV glu in Plasma Volume, Total SV glu in 24-hr Urine, and Total Free SV in 24-hr Feces for 10 Volunteers
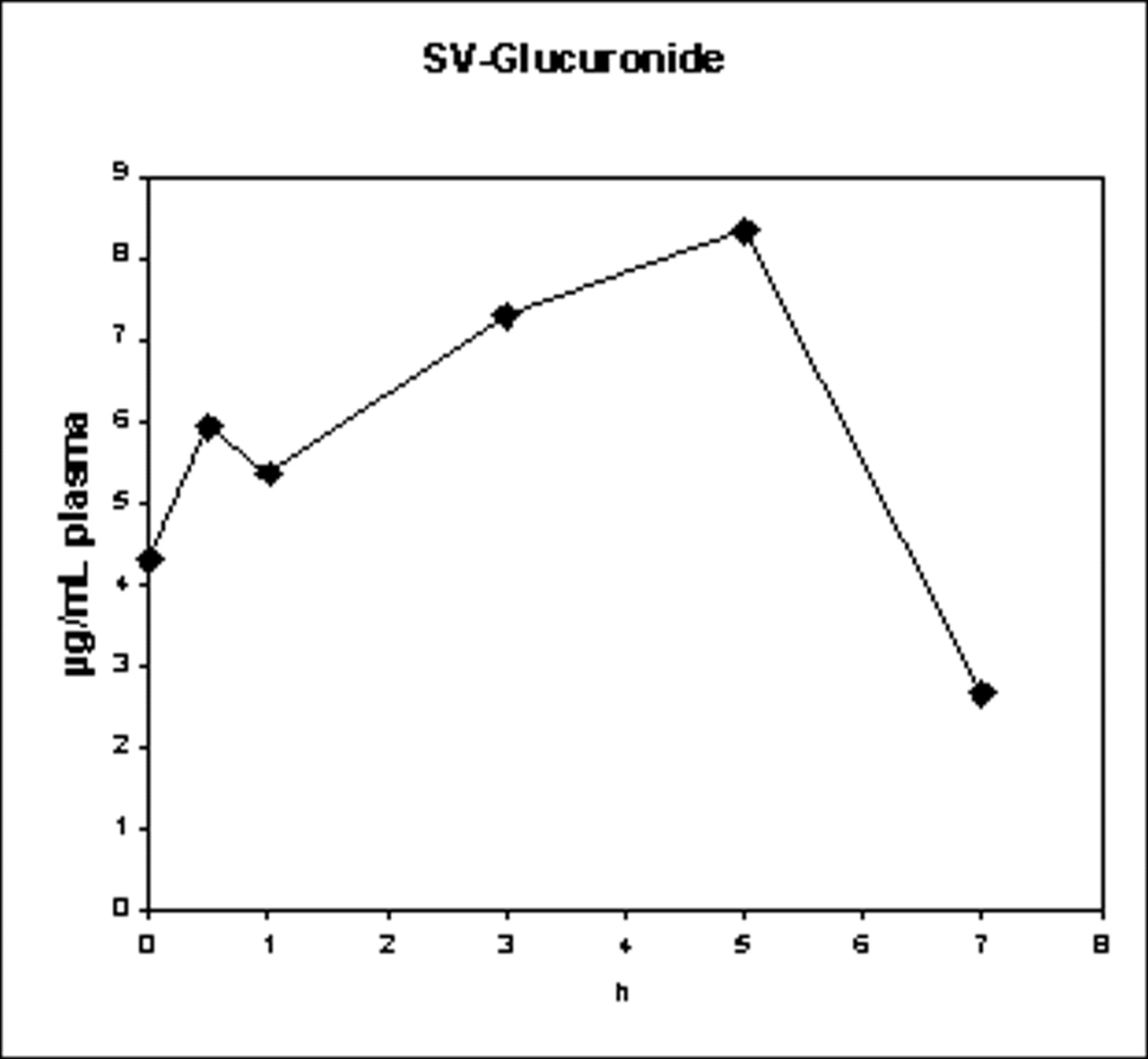
Amounts of steviol from the glucuronide (μg/ml plasma) in blood plasma of Volunteer 1 with time after the first stevioside administration on Day 3 of the experiment.
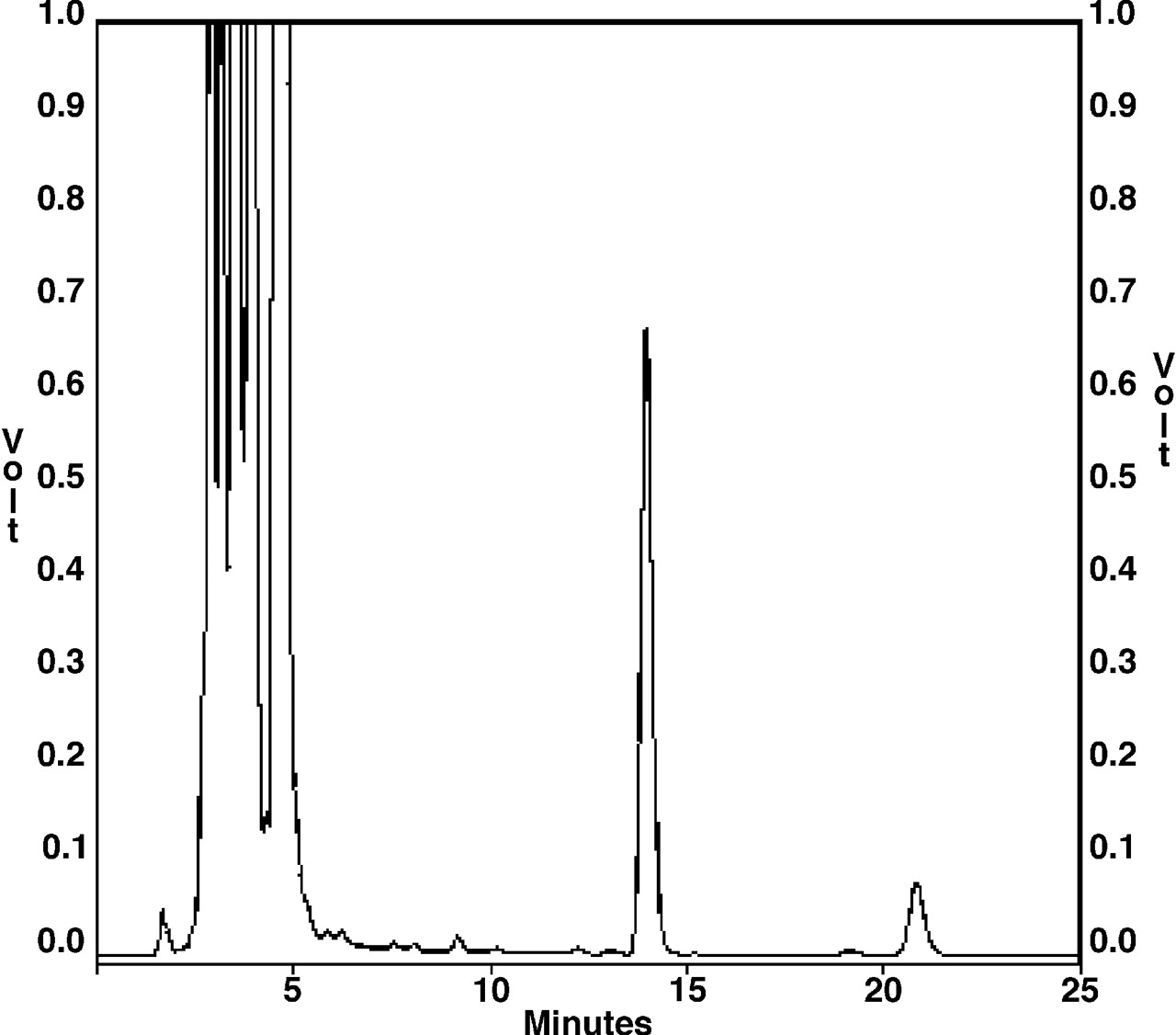
Example of HPLC analysis of steviol set free from SV glu of a urine sample (Rt 14: steviol 7-methoxy coumarinyl ester; Rt 21: dihydroisosteviol 7-methoxy coumarinyl ester, IS).

Hypothetical route from dietary stevioside to steviol glucuronide in human urine.
Footnotes
This work was supported by grant OT/00/15 from the Onderzoeksraad KULeuven, grant G.0111.01 from the Fonds voor Wetenschappelijk Onderzoek and Brulo Beheer.
Acknowledgements
We thank the volunteers for their participation in the study; the personnel of the division of Youth Health Care (University of Leuven) for taking the blood samples; the central laboratory of the University Hospital Gasthuisberg of Leuven for the analyses of plasma glucose, plasma insulin, and the different markers in the urine (creatinine, sodium, potassium, calcium, and urea); and Hilde Verlinden, Tom Struyf, and Christine Vergauwen for their excellent technical assistance.