
Abstract
Beneficial effects of inhaled nitric oxide (iNO) on arterial oxygenation in acute lung injury (ALI) suggest the presence of vasoconstriction in ventilated lung regions and this may be influenced by endothelin-1 (ET-1). We studied a possible interaction between ET-1 and iNO in experimental ALI. Sixteen piglets were anesthetized and mechanically ventilated (inspired O2 fraction, 1.0). After induction of ALI by surfactant depletion, animals were randomly assigned to either inhale 30 ppm NO (iNO group, n=8), or to receive no further intervention (controls, n=8). Measurements were performed during the following 4 hrs. In all animals, induction of ALI significantly decreased arterial oxygen tension (PaO2) from 569 ± 15 (prelavage) to 58 ± 3 mm Hg. Inhaled NO significantly increased PaO2 when compared with controls (iNO group: 265 ± 51 mm Hg; controls: 50 ± 4 mm Hg, values at 4 hrs, P < 0.01). Prelavage ET-1 plasma levels were comparable between groups (iNO: 0.74 ± 0.03, controls: 0.71 ± 0.03 fmol/ml, NS). During the protocol, the ET-1 levels increased and were different at 3 hrs (iNO: 0.93 ± 0.06, controls: 1.25 ± 0.09 fmol/ml; P < 0.05). PaO2 changes induced by iNO revealed a moderate and significant correlation with ET-1 plasma levels (R = 0.548, P = 0.001). Our data suggest that endogenous ET-1 production influences the efficacy of iNO in ALI. Furthermore, iNO reduced ET-1 plasma levels, possibly indicating anti-inflammatory properties of iNO in the early phase of ALI.
Introduction
Acute lung injury (ALI) and the acute respiratory distress syndrome (ARDS) are characterized by the presence of alveolar collapse, an increased intrapulmonary right-to-left shunt, and acute pulmonary arterial hypertension, consecutively resulting in severe hypoxemia (1). The improvement in gas exchange and a simultaneous reduction in pulmonary artery pressure are essentials in the therapy of ALI. In patients with ARDS, inhaled nitric oxide (iNO) has been demonstrated to induce selective vasodilation of pulmonary vessels in ventilated lung regions, thereby improving gas exchange and reducing pulmonary hypertension without effects on systemic circulation (2, 3).
Not all patients with ALI or ARDS, however, respond favorably to iNO therapy. Various studies have reported a fraction of 20%–35% nonresponders. Despite intensive investigation only little is known about the pathophysiologic factors influencing the response to iNO. It is, however, reasonable that beneficial effects of selective vasodilation in ALI suggest a certain degree of vasoconstriction in ventilated lung regions (4). This is confirmed by investigations in septic patients with ARDS demonstrating a reduced response to iNO, most likely from an increased expression of inducible NO synthase (5). Vasoconstriction in ventilated lung areas might be influenced by endothelins, which were reported to be markedly increased in plasma and lung tissue in ARDS patients (6, 7).
Endothelin-1 (ET-1), the main endothelin subtype, has been characterized to be a potent vasoconstrictor, a mediator of pulmonary hypertension and bronchoconstriction, and is possibly related to pulmonary inflammatory responses (8, 9). We hypothesized that an increased formation of ET-1 may affect the response to iNO and investigated a possible relation between iNO-induced improvements in arterial oxygenation and ET-1 plasma levels in an experimental model of acute lung injury.
Materials and Methods
General Experimental Procedure.
This study was approved by the Berlin Animal Protection Committee in accordance with the German Animal Protection Law, and conforms with the Guide for the Care and Use of Laboratory Animals (DHHS, PHS, NIH Publication No. 85-23). Sixteen piglets with a body weight of 25 ± 4 kg were studied. After premedication, anesthesia was performed as previously described in detail (10). The animals were tracheotomized, intubated with a tracheal tube (inner diameter of 8.0 mm), placed in a supine position, and mechanically ventilated in a volume controlled mode (tidal volume 12 ± 2 ml/kg−1, respiratory rate 16 min−1, inspired O2 fraction [FiO2] 1.0, inspiratory-expiratory ratio 1:1, positive end expiratory pressure [PEEP] 5 cm H2O) using a Servo 300A ventilator (Siemens-Elema, Solna, Sweden). Throughout the experiments, no cardiotonic or vasoactive drugs were administered.
In each pig a pulmonary artery catheter (model 93A-431-7.5Fr; Baxter Healthcare Corporation, Irvine, CA) was inserted via the femoral vein, and an arterial line (18 G; Vygon, Ecouen, France) was placed into the femoral artery. These catheters served for blood sampling and hemodynamic measurements. Heart rate, mean arterial pressure, and mean pulmonary artery pressure (MPAP) were recorded using a Hewlett-Packard monitoring system (Model 66 S; Böblingen, Germany). Cardiac output was determined using the thermodilution technique and is expressed as the mean of four measurements during different phases of the respiratory cycle. Intrapulmonary shunt (QS/QT) was calculated using standard formula. Blood samples for blood gas analysis were collected anaerobically and analyzed immediately (ABL 520; Radiometer, Copenhagen, Denmark). Arterial oxygen saturation and mixed venous oxygen saturation were measured by spectrophotometry with the analyzer calibrated for pig blood (OSM 3 Hemoximeter; Radiometer). Quantitative determination of ET-1 plasma concentration was performed with an enzyme immunoassay (BI-20052; Biomedica, Vienna, Austria): detection limit 0.05 fmol/ml, intraassay coefficient of variation <5%, interassay coefficient of variation <10%. Samples were collected in aprotinin-coated, cooled plastic vials. After centrifugation, plasma was stored in uncoated vials at −20°C until analysis. According to the manufacturer’s instruction for the handling of plasma samples from animals, a precipitation reaction to reduce nonidentified interfering substances was performed before measuring ET-1.
Experimental Protocol.
Repeated lung lavages with isotonic saline were performed to wash out lung surfactant as reported and described in detail elsewhere (11). An arterial oxygen tension (PaO2)/FiO2 ratio persisting below 100 mm Hg for 1 hr was considered as onset of ALI. After induction of ALI, animals were randomly assigned to either receive iNO (AGA, Bottrop, Germany) at a dose of 30 ppm continuously (iNO group, n = 8) or to receive no further treatment (controls, n =8). iNO was mixed into inspired gas using a module attached to the ventilator (Servo 300A/NO; Siemens-Elema). A fast-responding chemiluminescence analyzer (CLD 700 AL; ECO Physics, Duernten, Switzerland) was used to measure iNO concentrations.
Statistical Analysis.
Results are expressed as mean ± SEM. Data were obtained at baseline (prelavage), immediately after the induction of ALI (after lavage), and at hourly intervals during a 4-hr period. Statistical analysis was performed using SPSS for Windows 8.0 (SPSS Inc., Chicago, IL). Normal distribution of the variables was verified with the Kolmogorov-Smirnov test. Differences between groups were evaluated with Student’s t test for unpaired samples (two-tailed). Correlation coefficients were calculated according to Pearson. Statistical significance was assumed at P < 0.05.
Results
Gas Exchange.
The animals were comparable with regard to body weight and prestudy conditions. Induction of ALI decreased PaO2 from 569 ± 15 mm Hg (prelavage) to 58 ± 3 mm Hg in all animals and increased pulmonary shunt from 14 ± 1% to 50 ± 2% (Table 1). Inhalation of 30 ppm NO induced substantial and sustained improvements in gas exchange. In the iNO group, PaO2 increased from 60 ± 6 mm Hg after induction of ALI to 265 ± 51 mm Hg at 4 hrs of treatment, whereas PaO2 remained low in controls (PaO2 at 4 hrs: 50 ± 4 mm Hg; P < 0.05). Accordingly, QS/QT was significantly reduced in the iNO group when compared with controls (21 ± 3% vs. 55 ± 4%; values at 4 hrs; P < 0.05).
Hemodynamics.
During the protocol, mean arterial pressure remained stable and measured values were not significantly different between groups (Table 1). Induction of ALI increased MPAP in all animals from 23 ± 1 to 30 ± 2 mm Hg (Table 1). In controls, MPAP continued to increase during the following 4 hrs to a value of 42 ± 1 mm Hg. MPAP values in the iNO group were significantly lower when compared with controls at 3 hrs and at 4 hrs, respectively. There were no significant differences in heart rate or cardiac output between the groups before and after induction of lung injury (Table 1). All animals from both groups survived the study period.
ET-1 Plasma Concentrations.
Prelavage ET-1 plasma levels were comparable between groups (iNO: 0.76 ± 0.03, controls: 0.73 ± 0.03 fmol/ml, NS). After an initial increase at 1 hr after onset of ALI (iNO: 1.01 ± 0.06, controls: 1.08 ± 0.1 fmol/ml; NS), values were significantly different at 4 hrs (iNO: 0.88 ± 0.06, controls: 1.19 ± 0.10 fmol/ml; P < 0.05; Fig. 1). There was a significant correlation between relative changes in PaO2 (calculated as difference from PaO2 at the onset of ALI) and ET-1 plasma levels at 1 hr (R = 0.806, P = 0.016) and at 4 hrs (R =0.906, P =0.002); changes in intrapulmonary shunt were inversely correlated with ET-1 plasma levels at 1 hr (R =0.809; P =0.015), and there was a trend for such a relation at 4 hrs (R =−0.632, P = 0.093). We further increased the variability of the data set by including for each animal the four values of PaO2 differences from ALI onset and the four ET-1 plasma levels that were obtained during the protocol at the different time points, ending up in 32 single determinations. Statistical analysis of this data set revealed a moderate and significant correlation between PaO2 changes induced by iNO and ET-1 plasma levels (R = 0.54, P = 0.001; Fig. 2). Similar to arterial oxygenation, there was a moderate inverse correlation between iNO-induced changes in pulmonary shunt (calculated as difference from QS/QT values at the onset of ALI) and ET-1 plasma concentrations (R =−0.53, P = 0.002; Fig. 3). Values of mean pulmonary artery pressure were moderately correlated with ET-1 plasma levels in controls (R = 0.46, P = 0.003; Fig. 4), whereas no such relation was found in the iNO group (R = 0.16; P = 0.329). To increase variability of the data set, we included for each animal five pairs of values for MPAP and ET-1 plasma levels, which were measured during the protocol at the onset of ALI and the subsequent 4 hrs, resulting in 40 data pairs for both groups.
Discussion
In our experimental model of ALI, 30 ppm iNO significantly improved gas exchange when compared with untreated controls. This was not accompanied by systemic effects demonstrating selective pulmonary vasodilation. The beneficial effects of iNO on arterial oxygenation and on pulmonary right-to-left shunt were significantly correlated with the magnitude of ET-1 plasma levels. The increase in ET-1 plasma concentration at 3 hrs and 4 hrs after induction of ALI was significantly lower in the iNO group when compared with controls.
Apart from being directly vasoactive, the values of arterial ET-1 plasma levels may also reflect an increased production of ET-1 in lung tissue induced by ALI, which has been previously reported in biopsies of ARDS patients (12). Shear stress, hypoxia, proinflammatory cytokines (tumor necrosis factor-α, interleukin-1β), and growth factors (transforming growth factor-β) induce the expression of ET-1 mRNA (9), thus contributing to enhance pulmonary vascular tone in ALI. These mechanisms are not restricted to consolidated shunt areas; moreover, their presence is also expected in ventilated lung tissue. The enhanced ET-1 production induced by ALI contributes to increase pulmonary vascular tone as we demonstrated by a significant correlation between MPAP values and ET-1 plasma levels in controls. In the intervention group, this correlation was lost, most likely because iNO antagonized vasoconstriction by ET-1 in ventilated lung regions.
Two main factors that potentially influence the efficacy of iNO to improve gas exchange in patients with ALI and ARDS have been identified. First, it has been demonstrated that beneficial effects of iNO at various concentrations on arterial oxygenation were correlated with the extent of intrapulmonary shunt (5, 13), favoring application as rescue treatment in severe refractory hypoxemia (4). Second, the reduction in pulmonary artery pressure and pulmonary vascular resistance induced by iNO demonstrated a significant correlation with baseline values of these parameters before treatment (5, 14). The importance of pulmonary vasoconstriction has been confirmed in septic experimental models in which a cytokine-induced endogenous iNOS expression diminished the response to exogenously applied iNO, whereas iNOS inhibitors could reverse this effect (15). In this context, our data provide the first experimental evidence for a significant correlation between ET-1 release and iNO-induced effects on gas exchange in ALI. Because iNO is selectively active in ventilated lung regions, this suggests an important contribution of ET-1 to vasoconstriction in these areas. It has to be considered, however, that the correlation obtained was only moderate and that other constricting substances may also be involved.
Our results were obtained in responders because PaO2 increased in all animals receiving iNO by more than 20%. Thus the efficacy of iNO in this subgroup depends on the presence of vasoconstriction due to ET-1. This does not necessarily imply that iNO nonresponders among ARDS patients may have substantially reduced ET-1 levels; most likely, this phenomenon is primarily caused by endogenous NO being produced by inducible NO synthase, which is upregulated during inflammatory processes in septic patients. The increased endogenous NO formation antagonizes constricting effects unselectively in both ventilated and shunt areas without improving gas exchange. Accordingly, an increased fraction of iNO nonresponders among septic ARDS patients has been reported (5).
A further major finding of our study was that iNO significantly suppressed the release of ET-1 in an experimental model of ALI. This parallels the results of other investigations. Boulanger and Lüscher reported an increased release of ET-1 in porcine aortae preconstricted with thrombin when endogenous NO synthesis was inhibited by L-NMMA (16). In cultured human umbilical vein endothelial cells Kourembanas and colleagues have demonstrated a down-regulation of ET-1 gene expression by the NO donator nitroprusside during hypoxia. Thus NO may exert vasodilating effects in two ways: by a cGMP-mediated direct effect on vascular smooth muscle cells and by suppressing ET-1 formation (17). In addition to its vasoconstricting properties, ET-1 is involved in pulmonary inflammation (18). Stimulation of pulmonary endothelin-A receptors mediates the release of leukotrienes, platelet-activating factor, and cytokines. Accordingly, endothelin receptor blockers have been successfully used in animal models of airway inflammation (19). The decrease in ET-1 formation induced by iNO might therefore indicate possible anti-inflammatory effect of the inhaled treatment in the early phase of ALI.
In conclusion our data suggest that the release of ET-1 is one of the factors influencing the efficacy of iNO to improve gas exchange in ALI. Furthermore, iNO reduced ET-1 plasma levels by a negative feedback mechanism, contributing to vasodilation and possibly indicating anti-inflammatory properties of iNO in the early phase of ALI.
Parameters of Hemodynamics and Gas Exchange a
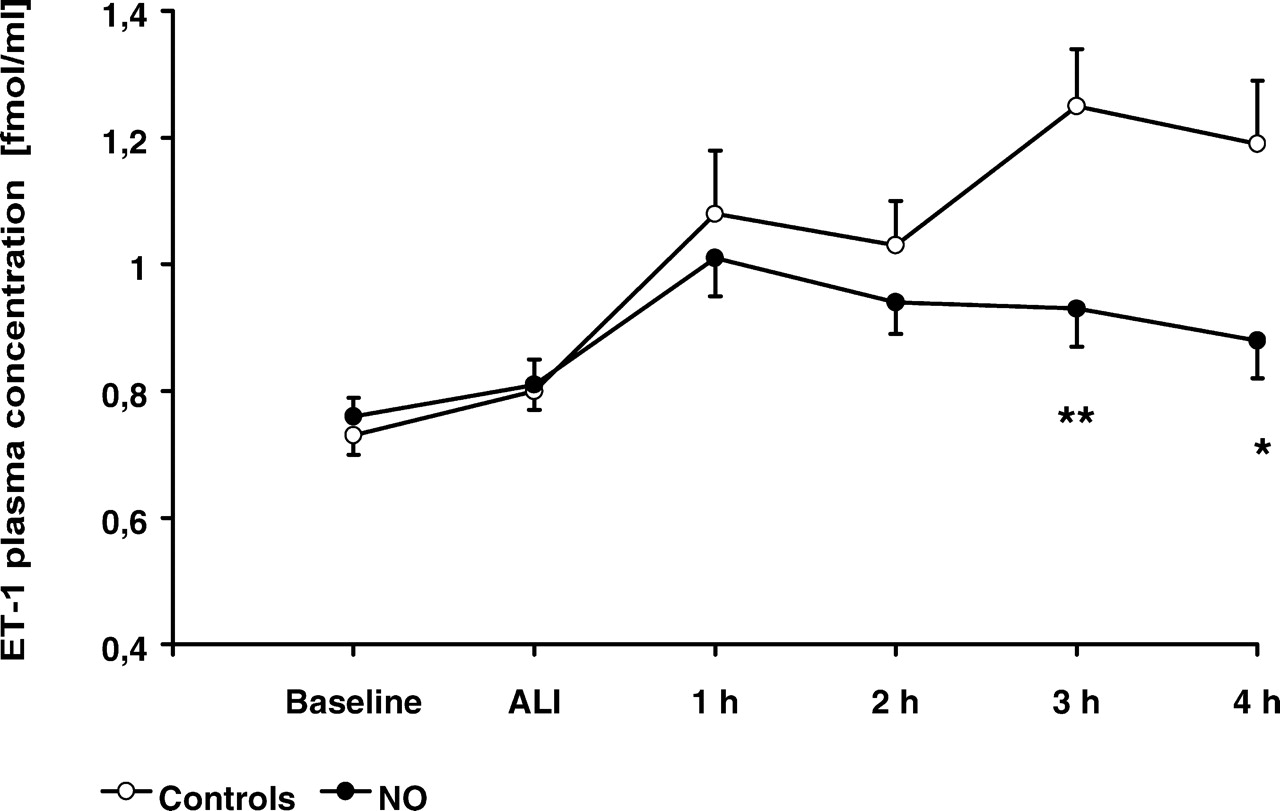
Arterial ET-1 plasma levels in iNO group (n = 8) and controls (n = 8) during the protocol. Continuous inhalation of NO during acute lung injury induced a decrease in ET-1 release that was significant at 3 hrs and 4 hrs (* P < 0.05 vs. controls; ** P < 0.01 vs. controls).
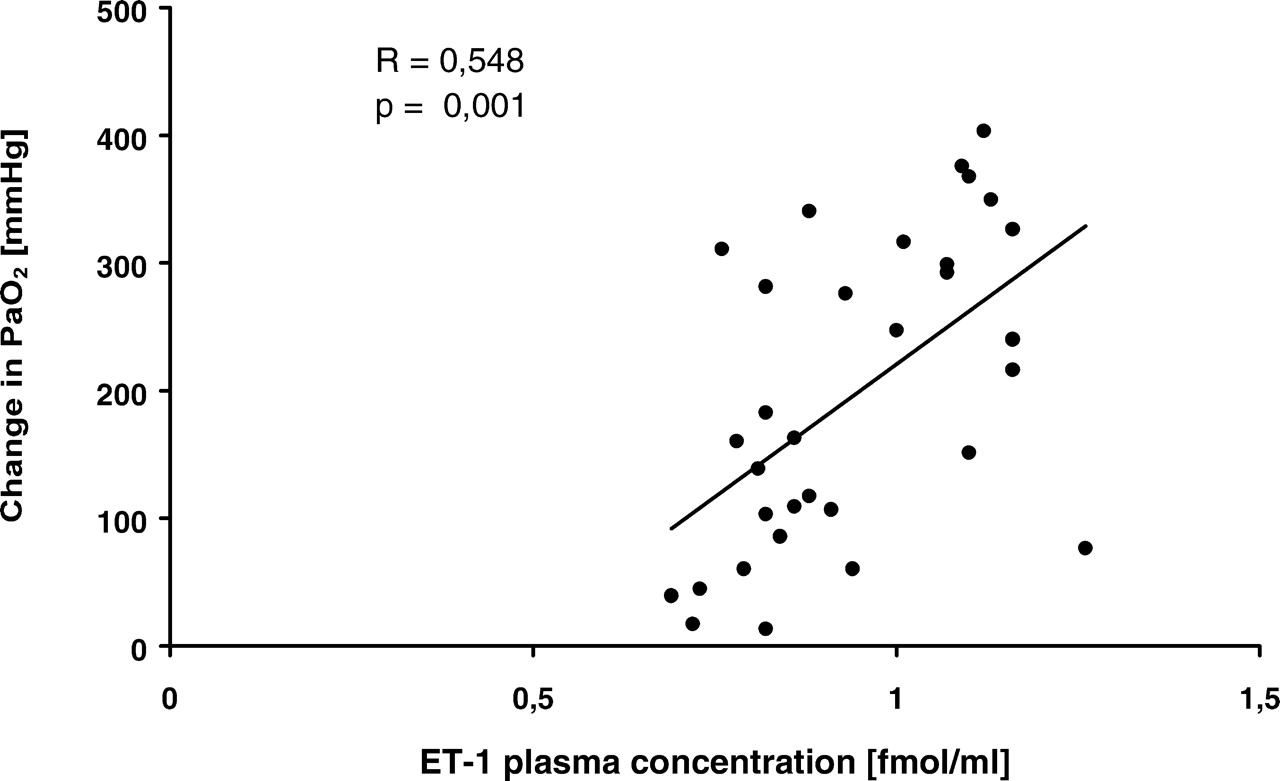
Relationship between iNO-induced improvements in PaO2 and ET-1 plasma levels. In each animal of the iNO group, we included results from four measurements obtained in hourly intervals during the protocol resulting in a total of n =32 data points. Changes in PaO2 are defined as the difference from the values measured at the onset of ALI. A moderate statistically significant relationship is present. Correlation coefficient R and significance level p are indicated.

Relationship between iNO-induced improvements in QS/QT and ET-1 plasma levels. In each animal of the iNO group, we included results from four measurements obtained in hourly intervals during the protocol resulting in a total of n =32 data points. Changes in QS/QT are defined as difference from the values measured at the onset of ALI. An inverse moderate statistically significant correlation is demonstrated. Correlation coefficient R and significance level p are indicated.
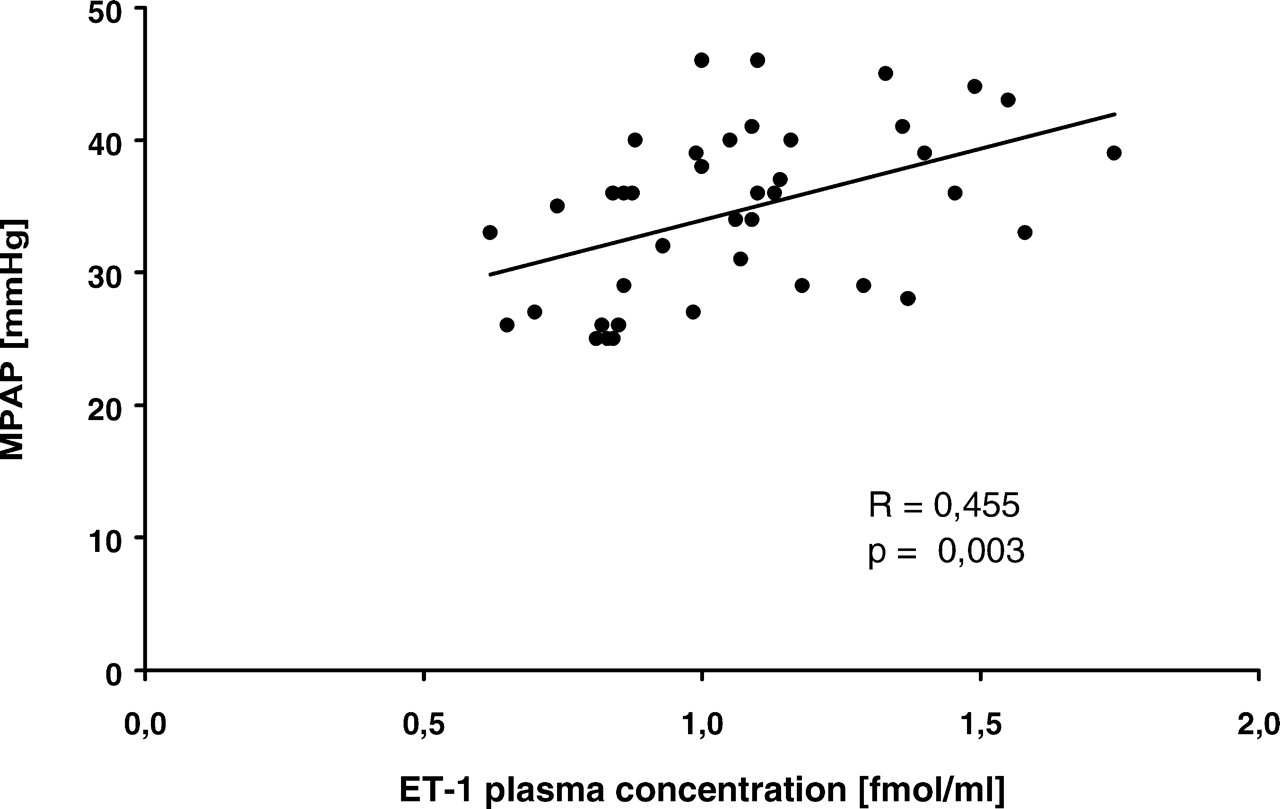
Relationship between MPAP and ET-1 plasma levels in controls. In each control animal, we included results from five measurements obtained at the onset of ALI and at the following 4 hrs during the protocol resulting in a total of n = 40 data points. A moderate statistically significant correlation is demonstrated. Correlation coefficient R and significance level p are indicated.
Footnotes
Supported by a grant from the Deutsche Forschungsgemeinschaft (DFG KA 1212/4–1).
1
These authors contributed equally to this study.
Acknowledgements
We thank Daniela Bayerl for her excellent assistance in the analysis of ET-1.