
Abstract
Fibromyalgia (FMS), a predominantly female (85%) syndrome, affects an estimated 2% of the US population with skeletal muscle ache, fatigue, headache, and sleep disorder. The pathogenesis of FMS is unknown and there is no laboratory test for diagnosis. In this study, plasma levels of 25 cytokines and chemokines in 92 female patients with FMS and 69 family members were measured compared to 77 controls. Trans-endothelial migration of normal leukocytes in response to FMS plasma and the cytokine profile of human myoblasts were analyzed. High levels of MCP-1 (P < 0.001) and eotaxin (P < 0.01) were found in patients and family members compared to controls. Patients (56/92) treated with the single agent guaifenesin (>3 months) had higher levels of eotaxin than those not treated (P < 0.01). Diluted plasma from patients increased the migration of normal eosinophils and monocytes, but not neutrophils, through an endothelial/Matrigel barrier only when mast cells are included in the lower wells (P < 0.05). Furthermore, myoblasts can secrete MCP-1, eotaxin, and IP-10, while treatment with MCP-1 caused secretion of IL-1β, eotaxin and IP-10. FMS is associated with inflammatory chemokines, that MCP-1 and eotaxin may contribute to the symptoms of FMS, and that similar cytokine profiles found in family members support the idea that FMS has a genetic component. Furthermore, the chemokine profile associated with FMS has direct effects on the migration of eosinophils and monocytes in the presence of mast cells, and skeletal muscle itself may secrete
Introduction
Fibromyalgia (FMS) is a syndrome of unknown etiology characterized by chronic widespread joint and muscle pain and found predominantly in females (80%–90%). Work disability is a serious concern in FMS (1) with the potential for a large economic impact since FMS affects approximately 2% of the US population (2). The American College of Rheumatology’s criteria for FMS include diffuse soft tissue pain of at least 3 months duration and pain on palpation in at least 11 of 18 paired tender points (3). In half of all patients, symptoms appear after a flu-like illness or after physical or emotional trauma (4). Approximately 30% of patients with FMS are diagnosed as having concurrent depression or anxiety disorders (5). Patients are usually diagnosed between the ages of 20 and 50 years, but the incidence rises with age so that, by age 80, approximately 8% of adults meet the classification criteria established by the American College of Rheumatology (6). The pathogenesis of FMS is unknown, although abnormalities in the musculoskeletal system, the neuroendocrine system and the central nervous system have been proposed (7), as well as correlations to genotypes of the catechol-O-methyltransferase (8) and dopamine D4 receptor (9). The drug therapy for FMS is largely symptomatic, including muscle relaxants, pain medicines, antidepressants, and sleep medicines. The strategy in treating FMS is to decrease pain and to increase function without promoting polypharmacy. The main challenge in evaluating patients with suspected FMS is that there is no gold standard test for diagnosis. It is primarily a diagnosis of exclusion, established only after other causes of joint or muscle pain are ruled out.
Based on the hypothesis that immunological dysfunction plays an important role in FMS and that FMS has a family basis, our investigation assessed cytokine and chemokine plasma levels in patients with FMS and their family members and evaluated their presumable diagnostic value. High levels of eotaxin and MCP-1 were found in patients and family members compared to controls. Diluted plasma from patients increased the migration of normal eosinophils and monocytes, but not neutrophils, through an endothelial/Matrigel barrier only when mast cells are included in the lower wells. Furthermore, myoblasts can secrete MCP-1, eotaxin, and IP-10, while treatment with MCP-1 caused secretion of IL-1β, eotaxin and IP-10. These results suggest that FMS is associated with inflammatory chemokines, that eotaxin and MCP-1 may contribute to the symptoms of FMS, and that similar cytokine profiles found in family members support the idea that FMS has a genetic component.
Materials and Methods
Study Participants. Adv PS586B
The study population consisted of 92 patients with FMS (females, mean age 43 ± 15 years, range 16–69) fulfilling the American College of Rheumatology criteria of FMS, 69 family members (25 females, mean age 52 ± 15 years, range 20–73, and 44 males, mean age 56 ± 15 years, range 20–74). 56/92 (60%) of the patients with FMS were treated with guaifenesin (100–600 mg/day for at least 3 months) and the remainder had not been treated with guaifenesin for at least 3 months. Healthy controls consisted of 77 anonymous discard blood samples taken from the City of Hope Blood Bank (48 females, mean age 47 ± 9 years, range 27–67, and 29 males, mean age 42 ± 11 years, range 19–59). Patients and their family members were recruited from Fibromyalgia Treatment Center of Los Angeles. Before inclusion in the study, informed consent was obtained from patients and their family members. This study was approved by the City of Hope Institutional Review Board.
Plasma Sample.
Blood samples obtained from patients, their family members, and controls were coded and treated anonymously throughout the analysis. Plateletrich plasma (PRP) and platelet-free plasma (PFP) were prepared according to Aras et al. (10). Briefly, PRP was obtained by centrifugation at 1400 rpm for 15 min and PFP was obtained by double centrifugation, first at 1200 g for 15 minutes, and subsequently at 12,000 g for 12 minutes at 20°C. PRP and PFP were stored at −20°C for future use. PRP was used for cytokine multiplex analysis and PFP for transendothelial migration assays (TEM). The DuoSet® ELISA Development System Kits for Human MCP-3 and Eotaxin-3 from R&D Systems, Inc. (Minneapolis, MN) were used to determine the level of plasma MCP-3 and Eotaxin-3.
Cell Separation.
Neutrophils and peripheral blood mononuclear cells (PBMC) were isolated from citrated blood of single healthy donors by Ficoll-Hypaque (Pharmacia Biotech, Uppsala, Sweden) density gradient centrifugation as recommended by the manufacturer and the purity of neutrophils were greater than 95% in all cases. Eosinophils were collected and separated using Eosinophil Isolation Kit (Miltenyi Biotec Inc., Auburn, CA) from neutrophils according to the manufacturer’s protocol. Monocytes were collected and separated using Monocyte Isolation Kit II (Miltenyi Biotec Inc., Auburn, CA) from peripheral blood mononuclear cells. The purity eosinophils or monocytes were respectively stained with anti-CCR3-PE and CD16-PerCP-Cy5.5 or CD14-FITC and checked by using flow cytometry FACSCalibur (BD Biosciences, San Jose, CA 95131). Eosinophils are showed as CCR3+CD16− cells, and monocytes as CD14+ cells. Neutrophils, eosinophils, and monocytes were labeled with either 5 μM CFSE for 5 min at room temperature in PBS. After washed twice, neutrophils, eosinophils, and monocytes were suspended in migration medium (RPMI 1640 without phenol red, supplemented with 100 U/ml penicillin, 100 mg/ml streptomycin, 1 mM L-glutamine) with cells concentration of neutrophils 5 × 106/ mL, eosinophils 5 × 105/mL, and monocytes 2 × 106/mL.
Cell Lines.
Human umbilical vein endothelial cells (HUVEC) and endothelial growth medium (EGM) supplemented with Bovine Brain Extract (3 mg/ml) were obtained from Cambrex Bio Science Walkersville, Inc. (Chicago, IL) and cultured in 75-cm2 culture flasks and maintained in EGM at 37°C in 5% CO2 atmosphere. All experiments were performed on cells at passages 3–4 of their growth kinetics to ensure consistency.
The human mast cell line HMC-1 was kindly provided by Dr. J. H. Butterfield (Mayo Clinic, Rochester, MN) (11). HMC-1 were grown in IMDM with 10% FCS, 2 mM L-glutamine, 1.2 mM a-thioglycerol (Sigma, St. Louis, MO) and antibiotics at 5% CO2, 37°C. HMC-1 was used at cell concentration of 1 × 104/mL.
Myoblast and skeletal muscle cell medium BulletKit® (containing skeletal muscle cell basal medium, EGF, insulin, dexamethasone, Gentamicin sulfate, Amphotericin-B, and Bovine serum albumin) were purchased from Cambrex Bio Science Walkersville, Inc. Cells were seeded in 24-well plates at 10,000 cells/cm2, grown to confluency, treated with MCP-1, eotaxin, IL-13, or IFNg for 48 h, and supernatants harvested for cytokine multiplex analysis.
Cell Migration Assay.
Transendothelial migration (TEM) was quantified using the Transwell System (3-μm pore size, BD Falcon, Chicago, IL). HUVEC at 4 × 104 cells/insert were seeded in 100 μl EGM on Matrigel-coated membranes (6.5 mm diameter, polycarbonate membrane with 3-μm pores), and were placed in 24-well culture plates. HUVEC were cultured for 5 days to form a tight monolayer, and permeability measured with FITC-labeled albumin (12). TEM were used when albumin diffusion was <5% of equilibrium. Eight patient or healthy control PFPs were diluted 1:10 with migration medium. HMC-1 (1 × 104/mL) were suspended in 10% PFP migration medium and added to lower chambers in quadruplicate. CFSE (carboxy fluorescein diacetate succimidyl ester, Molecular Probes, Eugene, OR) labeled eosinophils (5 × 104 cells), monocytes (2 × 105 cells) or neutrophils (5 × 105 cells) were added to upper wells, incubated at 37°C for 3 h, and the inserts were removed by gently scraping the bottom surfaces of the filters several times to dislodge the cells adhering to the under-surface of the endothelial cell-covered filters. Cell numbers in the lower wells were measured at 495 nm on the Victor V plate reader (PerkinElmer, Woodbridge, Canada).
Cytokine Multiplex Analysis.
PRP and the supernatant of myoblasts were analyzed for 25 cytokines using Human Cytokine Twenty-Five-Plex Antibody Bead Kit (Biosource International, Camarillo, CA) as per the manufacturer’s protocol (13). Briefly, Biosource’s multiplex bead solutions were vortexed for 20 s and 25 μl was added to each well and washed twice with wash buffer. The samples were diluted 1:2 with assay diluent and loaded onto Millipore Multiscreen BV 96-well filter plate; 50 μl of incubation buffer had been added previously to each well. Serial dilutions of cytokine standards were prepared in parallel and added to the plate. Samples were incubated on a plate shaker at 600 revolutions/min in the dark at room temperature for 2 hours. The plate was applied to a Millipore Multiscreen Vacuum Manifold and washed three times with 200 μl of wash buffer. One hundred μl of biotinylated Anti-Human Multi-Cytokine Reporter was added to each well. The plate was incubated on a plate shaker for 1 hour. After washing three times with 200 μl of wash buffer, streptavidin-phycoerythrin (100 μl) was added to each well. The plate was incubated on a plate shaker for 30 min. The plate was applied to the vacuum manifold, washed three times, and each well was resuspended in 100 μl wash buffer and shaken for 1 min. The assay plate was transferred to the Bioplex HTF Luminex reader (Bio-Rad Laboratories, Inc., Hercules, CA) instrument for analysis. Cytokine concentrations were calculated using Bio-Plex Manager 3.0 software with a five parameter curve-fitting algorithm applied for standard curve calculations for duplicate samples.
Statistical Analysis.
Assay results are expressed as means ± SD or ± SE, as specified in the tables. Unpaired Student’s t tests were used for comparisons in Table 2. All P values are two-sided. The 25 assays were screened for association with the six groups of study subjects using an F test with 5 degrees of freedom. Assays with P < 0.002 were investigated jointly using recursive partitioning to discriminate cases with and without guaifenesin and controls. The assays identified were further investigated using logistic regression to discriminate cases from controls. Each of the assays noted in Figure 4 was identified by both methods. Correlations were performed by the Pearson correlation methods. Data were analyzed with SPSS software (release 10.0, SPSS, Chicago, IL), GraphPad Prism software (version 4.0, GraphPad Software, San Diego, CA) and R version 2.4.1 with the R part package version 3.1–34.
Results
Baseline Characteristics.
A total of 92 female patients and 69 of their family members (Table 1) were enrolled in the study between April 21, 2005 and August 10, 2006. The pedigrees of the patient population fell into the following main groups: those in which the patient but neither parent had FMS, those in which one parent and the patient had FMS, and those in which one parent and the patient had FMS, but a sibling did not. We also had a pedigree in which a patient, mother and maternal grandmother all had FMS. Many of the patients (56/92, 60%) were treated with the single agent guaifenesin for at least 3 months prior to analysis, while the remainders were simply recorded as not treated with guaifenesin. Guaifenesin, the physiological hydrolysis product of methocarbamol, like methocarbamol, is a muscle relaxant and anesthetic used to treat the symptoms of FMS (14).
Plasma Levels of Cytokines and Chemokines.
Table 2 shows the raw results for the analysis of 25 cytokines and chemokines in the patients stratified for guaifenesin treatment vs age and gender balanced controls. The top four (MCP-1, eotaxin, IL-13 and IP-10) have significant differences between the patient and control groups, while a few others, notably IFNγ and TNFα, scored significantly in logistic regression analyses. Although these results are of some interest in their own right, the greatest separation between groups was found for eotaxin and MCP-1 that are presented separately in Figure 1. Compared to controls, both eotaxin and MCP-1 are elevated for patients treated with or without guaifenesin. In the case of eotaxin, levels are significantly higher in patients treated with guaifenesin compared to those not treated with guaifenesin, while in the case of MCP-1, levels are elevated to the same extent in both groups. Although these results suggest that measurement of eotaxin and MCP-1 levels may separate FMS patients from FMS, it is also clear that 40–50% of the patients, whether treated with guaifenesin or not, will score as normal by this test alone. Therefore, further analysis of the data was warranted.
First, we considered the facts that the genes for the CC chemokines for MCP-1, MCP-3, and eotaxin are clustered on the long arm of chromosome 17 (15) and additional genes for eotaxin-2 and eotaxin-3 are found on chromosome 7. Analysis of the plasma levels of MCP-3 and eotaxin-3 for FMS patients without guaifenesin treatment vs healthy controls showed no elevations in these chemokines (Fig. 2). Thus, it is unlikely that FMS involves all family members of the eotaxin/MCP gene families.
Second, it has been speculated that there is a genetic component to FMS and that the onset of severe symptoms may be caused by a chronic illness or trauma. Therefore, it was of interest to analyze the eotaxin/MCP-1 profile of non-affected family members. In this analysis, we found significant elevations for both female and male unaffected family members compared to similar age and gender controls (Fig. 3). These results suggest that the family members have the cytokine/chemokine profile characteristic of FMS without exhibiting the symptoms of FMS. These results support the idea that most of the cytokine/chemokine profile is shared among family members, suggesting either a genetic predisposition to FMS and/or a shared inflammatory condition of unknown etiology. However, the trend in patients vs controls is also affected by guaifenesin treatment. For example, eotaxin is elevated to the same extent in patients taking guaifenesin as in unaffected family members vs controls, but IL-13 is highest in patients not taking guaifenesin vs those taking guaifenesin, unaffected family members, and controls (Table 2). In addition, a preliminary pedigree analysis (data not shown) reveals that >50% of the patient’s parents had levels of both MCP-1 and eotaxin elevated to the same extent as the patient, while the remaining families had an equal distribution of pedigrees with only one or none of these two cytokines elevated in either parent.
Third, as mentioned above, the elevated levels of eotaxin and MCP-1 alone are not sufficient to separate FMS patients from controls in more than 40–50% of the patients studied. However, the elevation of these two chemokines suggests an underlying inflammatory condition that had not previously been detected by standard approaches such as muscle biopsies. In the case of patients treated with guaifenesin, significant elevations (P < 0.001) were found for 2 cytokines; however, for patients not treated with guaifenesin, significant elevations (P < 0.001) were found for 4 (Table 2). Combining data for cytokines can add significance to the analysis as shown in Figure 4A where combined MCP-1 and IP-10 levels clearly distinguish female controls from females patients not on guaifenesin and female family members, and in Figure 4B where combined eotaxin, TNFα, MCP-1 and IFNγ distinguish female controls from female patients on guaifenesin and female family members. The logistic regression analysis gave a predicted probability >70% or >80% for patients without or with guaifenesin treatment, respectively.
Fourth, previous studies have suggested that MCP-1 is an adipokine whose expression is increased in obesity (16–18) and the circulating levels of MCP-1 and IL-8 are related to obesity-related parameters body mass index (BMI) (19). To investigate the role of BMI in the plasma elevation of MCP-1 and eotaxin, FMS patients are divided into two groups, obese (BMI ≥ 25 kg/m2) and non-obese (BMI < 25 kg/m2). There were no significant differences in the MCP-1 or eotaxin levels between the two groups (Table 3). Furthermore, there was no significant correlation between BMI and MCP-1 in the obese group (r = −0.006, P =0.972). These data indicated that obesity is unlikely to be the reason of high plasma level of MCP-1 in FMS patients.
Effect of FMS Plasma on Cell Migration.
The ability of diluted plasma from patients or controls on the migration of normal eosinophils, monocytes and neutrophils through an endothelial cell/Matrigel barrier (HUVEC migration assay) was tested. For all three types of cells there was no difference between diluted normal or patient PFP (Fig. 5). In spite of this negative result, we realized that the assay includes only one cellular component of the physiological migration barrier, namely endothelial cells. A second cellular component is tissue resident mast cells that line the vascular bed and connective tissue and have potent interactions with migrating leukocytes. We therefore, repeated the migration assay with a human mast cell line HMC-1 in the lower chamber to simulate their potential interaction with the migrating leukocytes. In this assay system, we found a significant enhancement of migration due to the presence of diluted patient PFP for eosinophils and monocytes, but not for neutrophils (Fig. 5). These results strengthen the idea that elevated levels of eotaxin and MCP-1 can cause increased migration of their target cells, namely eosinophils and monocytes, and that the increased migration may require tissue resident mast cells which may act as a physiological amplifier or mediator for eotaxin and MCP-1 function. Notably, several studies suggest a role for activated mast cells in FMS (20).
Cytokine Production by Human Myoblasts.
Human myoblasts were tested for their ability to release MCP-1, eotaxin or IP-10 after stimulation with several cytokines. These cells can secrete significant amounts of MCP-1 when stimulated with IL-13 and IFNγ, eotaxin when stimulated with MCP-1, IL-13, and IFNγ, and IP-10 when stimulated with IFNγ, and to a lesser extent, MCP-1 (Fig. 6). When myoblasts were treated with MCP-1, eotaxin or IFN-γ, but not IL-13, they secreted significant amounts of IL-1β which may sustain a fever-like condition within the muscle. Thus, at least in vitro, myoblasts may be both the target and the source of the cytokines that sustain the immune response in the musculoskeletal system of FMS patients.
Discussion
FMS was originally called fibrositis, referring to regional pain syndromes associated with profound fatigue and sleep disturbance (21). Relatives of FMS patients have a high frequency of FMS symptoms, especially for female family members. Possible genetic associations include polymorphisms in the serotonin transporter promoter (22), the catechol-O-methyltransferase gene (8) and dopamine D4 receptor (9). Studies on the related disease, Chronic Fatigue Syndrome (CFS), uncovered polymorphisms in genes relating to serotonin production (23). These findings are of interest because one of the common treatments for FMS involves the broad class of selective serotonin reuptake inhibitors.
Our analysis of the cytokine and chemokine profiles in FMS patients and their unaffected family members supports the idea of a genetic component to FMS, since almost identical profiles for FMS patients vs unaffected family members compared to controls were found. Our studies suggest that the involvement of the immune system may be a likely source of pain in FMS. The possible involvement of mast cells as suggested by our in vitro studies, raises the possibility that serotonin production, one of the main mast cell effectors, is involved in the pathology of FMS.
Elevated eotaxin levels in FMS suggest that, like chronic asthma, where the production of eotaxin and the migration of eosinophils into the airways leads to prolonged activation of mast cells in the absence of IgE stimulation (24), migration of eosinophils into skeletal muscles may occur. Although we did not observe eosinophilia in the blood samples of our FMS cohort, it is a distinct possibility that low numbers of eosinophils migrate into their skeletal muscles in response to locally produced eotaxin and caused sustained activation of mast cells there. It is likely that a chronic condition of this nature would be missed in a routine muscle biopsy. It is noteworthy that treatment of myoblasts with MCP-1 produces high levels of eotaxin, suggesting that skeletal muscles themselves may be responsible for the production of eotaxin.
Eosinophilia myalgia syndrome (EMS) shares many symptoms with FMS, but is more severe. EMS characterized by peripheral eosinophilia, severe myalgia, dyspnea, pneumonitis, and skin sensitivity was linked to ingestion of large doses of (perhaps contaminated) dietary L-tryptophan supplements (25, 26). L-tryptophan, a precursor of serotonin, has been used for a variety of conditions associated with decreased production of serotonin. It is worth speculating that EMS is a form of FMS made more severe by overt eosinophilia and that a neuromuscular disorder is a root cause of both syndromes. For example, eosinophil granule proteins are known to be cytotoxic to a variety of mammalian tissues, including peripheral nerve cells (27).
MCP-1 is postulated to play pivotal roles in diseases characterized by mononuclear cell infiltration, including rheumatoid arthritis and bronchial asthma (28, 29). In this study we have found elevated levels of MCP-1 in the plasma of FMS patients and evidence for its production by myoblasts in response to stimulation by IL-13 and IFN-γ. In other studies on skeletal muscles, MCP-1 secretion is increased in the injured state (30) and in inflammatory myopathies (31), perhaps explaining why trauma is a frequent inducer of FMS. In addition, MCP-1 reduced insulin-stimulated glucose uptake in skeletal muscle (32). Thus, MCP-1 production may be related to the abnormalities in muscle energy metabolism and muscle tissue oxygenation found in biopsy specimens of tender areas taken from FMS patients (33). Furthermore, MCP-1 may play a role in pain production in nociceptive neurons (34, 35). Thus, skeletal muscle may be one source of the inflammatory chemokines MCP-1 and eotaxin, that in turn, sustain the activation of mast cells in their vicinity, maintaining chronic inflammation and pain in the skeletal muscle.
The suggestion that MCP-1 may be elevated simply because a portion of the FMS patients were obese was also examined; however, there was no evidence for this. On the other hand, MCP-1 has been shown to be elevated in patients with metabolic disease (36) and atherosclerosis (37, 38).
There are also some possible conflicting findings in our results. Notably, both eotaxin and MCP-1 levels are elevated in FMS patients, but eotaxin is a natural antagonist for CCR2, the main receptor for MCP-1 (39). Thus, the production of eotaxin may be an attempt to offset the deleterious effects of high MCP-1 on skeletal muscle. This possibility may be supported by the dichotomy seen in eotaxin levels between patients treated or not with guaifenesin. Since eotaxin levels are significantly elevated in treated vs untreated patients, the effect of the drug may be to counteract the effects of high MCP-1 levels. Similarly, IP-10, the natural antagonist for both eotaxin and MCP-1, may be produced to offset the effects of both chemokines (40).
In conclusion, the FMS cohort studied here is associated with elevated levels of inflammatory chemokines, MCP-1 and eotaxin may contribute to the symptoms of FMS, parents of these FMS patients share the expression profile, and myoblasts are a potential source of eotaxin and MCP-1. Therefore, reduction of eotaxin and MCP-1 levels or blockade of their receptors may be a reasonable treatment strategy for FMS. We also found evidence that treatment with guaifenesin accentuates eotaxin production and reduces IL-13 and IFNγ levels. While only a few studies have shown elevated cytokine levels in FMS (41, 42), our data suggests that elevated chemokine levels may play a causative role in FMS and should be investigated further.
Baseline Characteristics of FMS Patients and Family Members a
Plasma Level of 25 Cytokines/Chemokines in Female FMS Patients and Family Members a
Lack of Effect of Obesity on Plasma Levels of MCP-1 and Eotaxin in FMS Cohort a
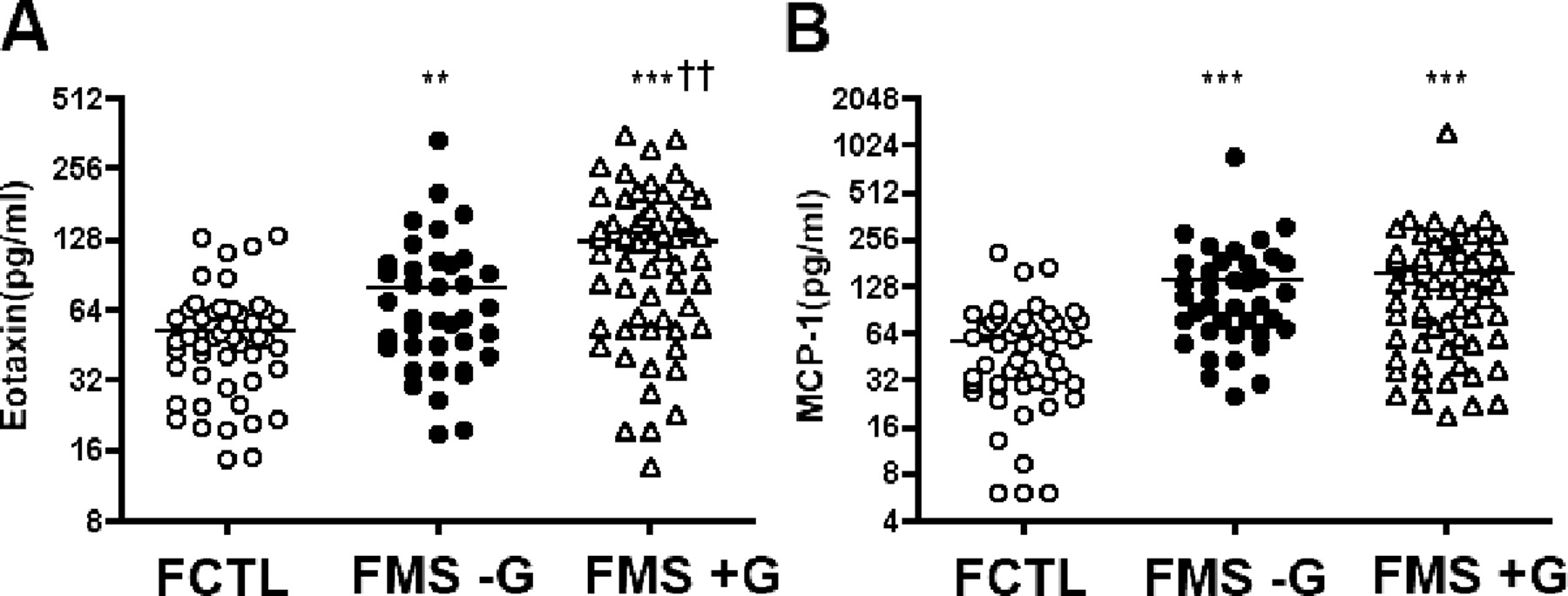
Plasma levels of eotaxin and MCP-1 in female FMS patients. Eotaxin (A) and MCP-1 (B) levels of female FMS patients with/without guaifenesin treatment. FCTL: female healthy controls, n = 48; FMS -G: female FMS patients without guaifenesin treatment, n = 36; FMS +G: female FMS patients with guaifenesin treatment, n =56; **P < 0.01, ***P < 0.001 in comparison with female controls; ††P < 0.01 in comparison with FMS -G.
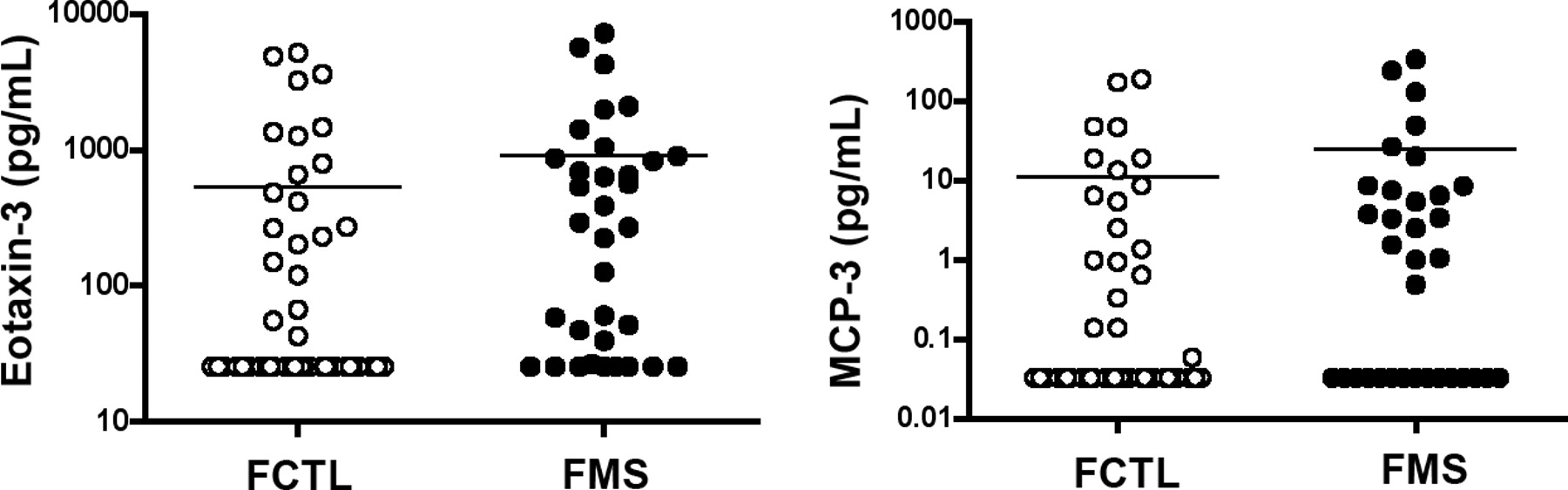
Plasma levels of MCP-3 and eotaxin-3 in FMS patients not treated with guaifenesin. FCTL: female controls, n =42; FMS: female FMS patients without guaifenesin treatment, n = 34.
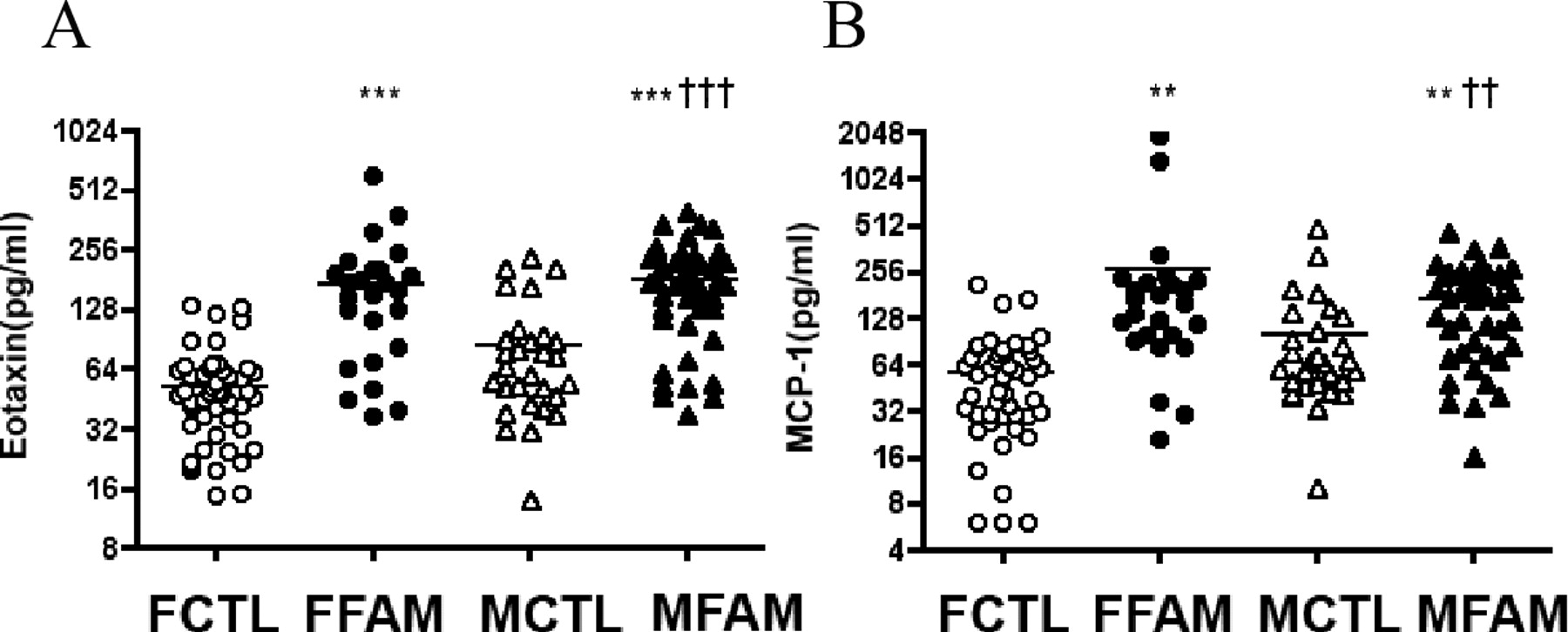
Plasma levels of eotaxin and MCP-1 in family members of FMS patients. Eotaxin (A) and MCP-1 (B) levels of family members of FMS patients. FCTL: female healthy controls, n = 48; FFAM: female family members of FMS patients, n = 25; MCTL: male healthy controls, n = 29; MFAM: male family members of FMS patients, n = 44. **P < 0.01, ***P < 0.001 in comparison with female controls; ††P < 0.01, †††P < 0.001 in comparison with male controls.
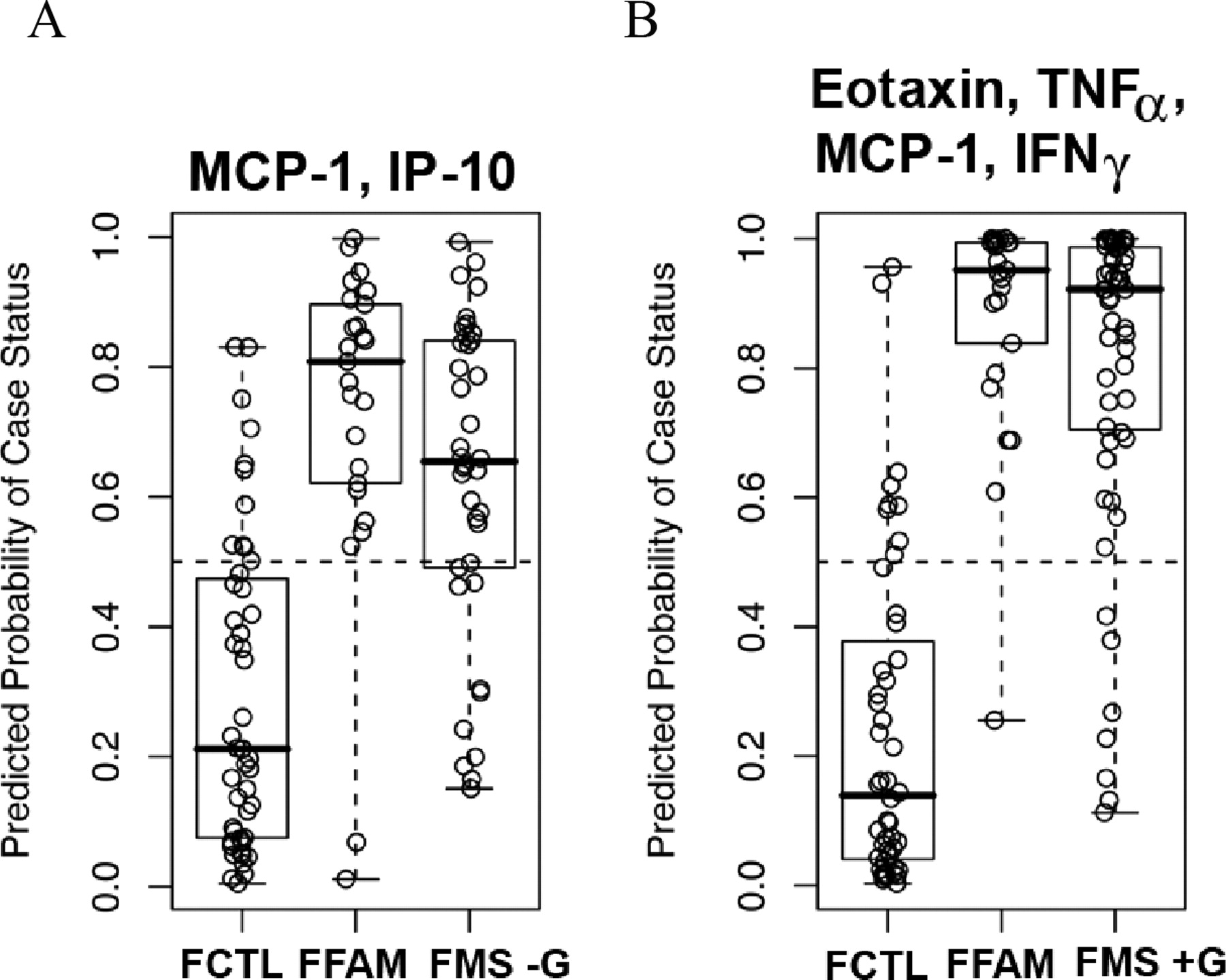
Predicted probability analysis in FMS patients and their family members. Predicted probability of case status of female family members and FMS patients not treated with guaifenesin using combined MCP-1 and IP-10 levels (A). Predicted probability of case status of female family members and FMS patients treated with guaifenesin using combined MCP-1, eotaxin, TNFα and IFNγ levels (B).
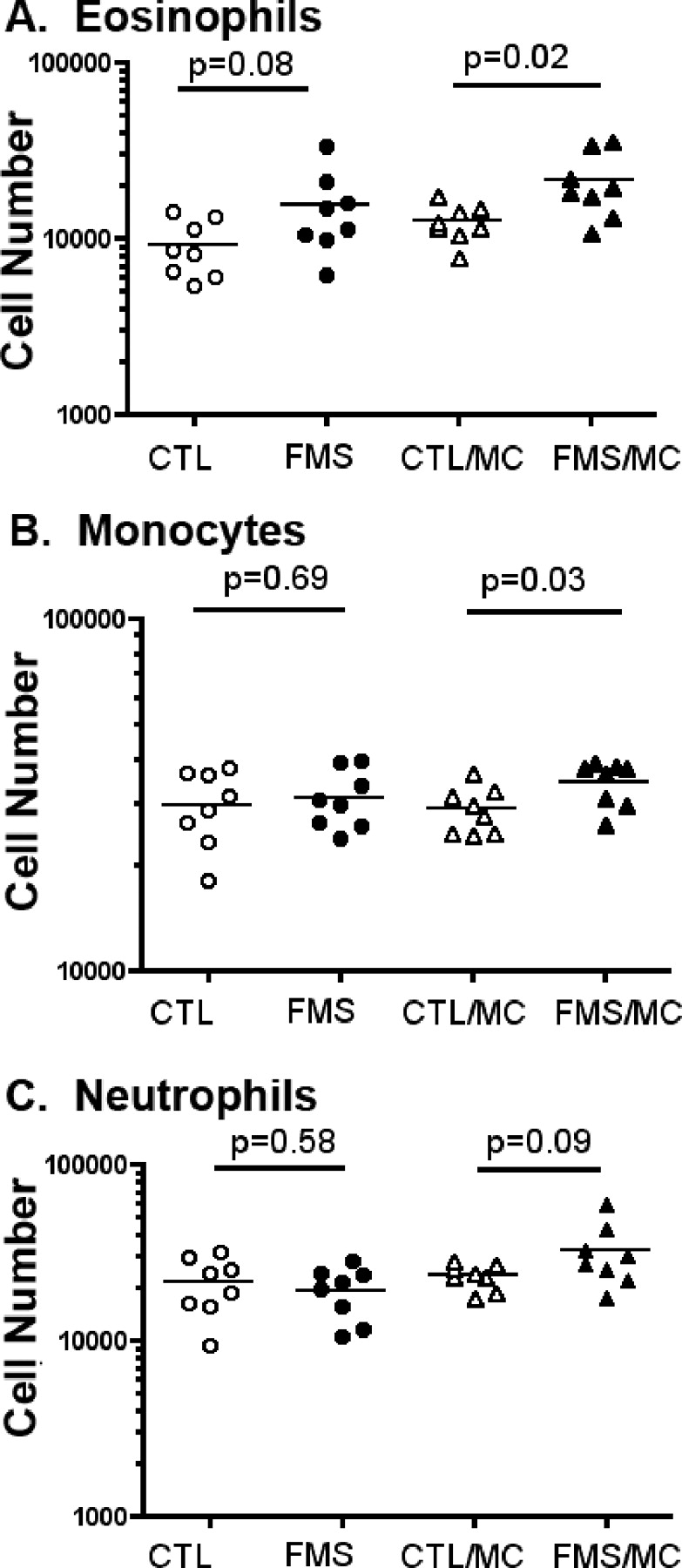
Effect of FMS plasma and mast cells on eosinophils and monocytes transendothelial migration. Migration of eosinophils (A), monocytes (B), or neutrophils (C) towards diluted control or FMS plasma, with/without added mast cells. CTL: 10% control PFP migration medium in lower chamber, n = 8; FMS: 10% FMS PFP migration medium in lower chamber, n = 8; CTL/MC: 10% control PFP migration medium +HMC-1 (10,000 cells/mL) in lower chamber, n = 8. FMS/MC: 10% FMS PFP migration medium +HMC-1 (10,000 cells/mL) in lower chamber, n =8. P values were calculated between groups under the bar.
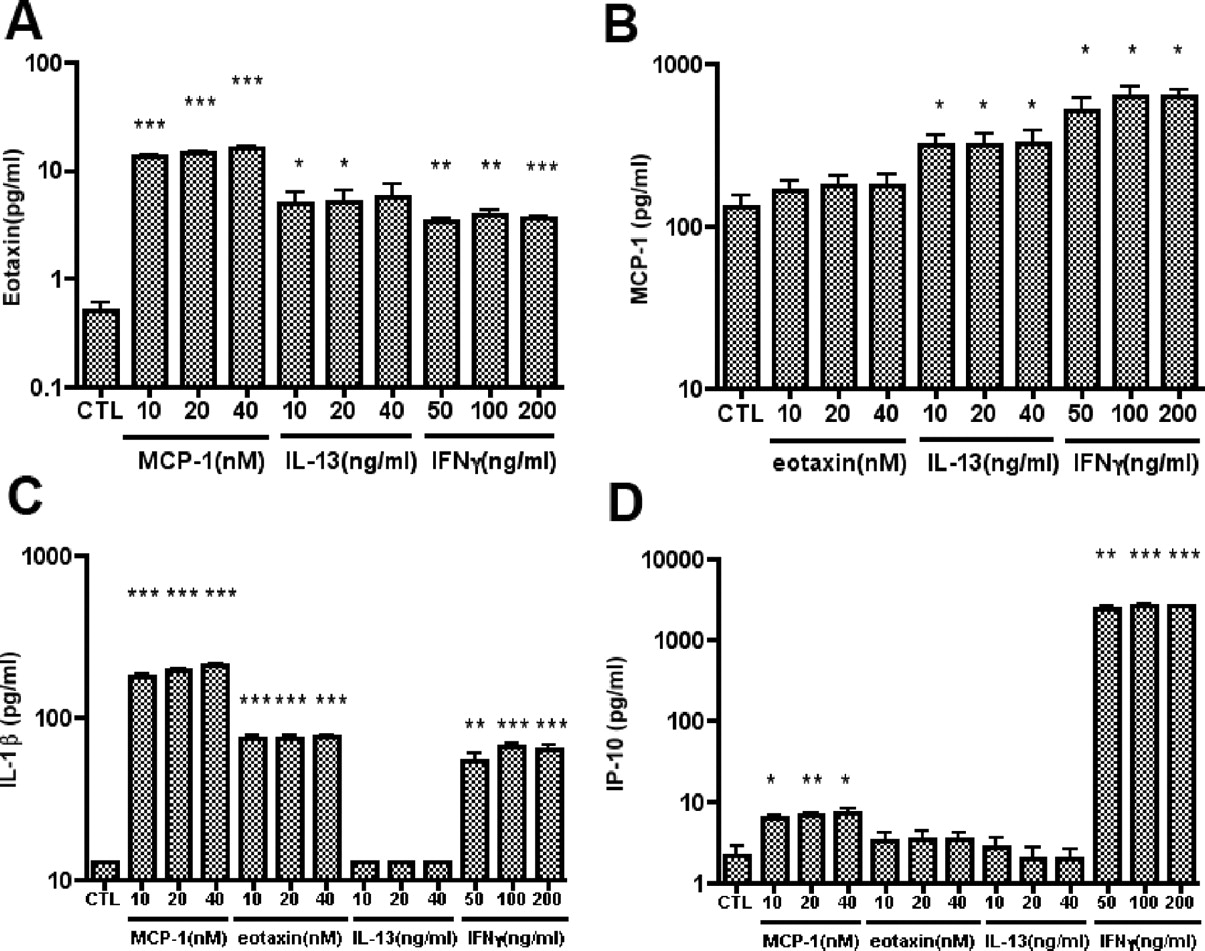
Eotaxin, MCP-1, IL-1β or IP-10 secretion profiles of human myoblasts after stimulation with cytokines. Confluent myoblasts were treated with MCP-1, eotaxin, IL-13 or IFNγ at the doses indicated for 48 h and 25 cytokines levels measured (only four are shown here). CTL: untreated control. *P < 0.05, **P < 0.01, ***P < 0.001 in comparison with controls (n = 3).
Footnotes
The research was funded by a grant from Los Angeles Fibromyalgia Foundation (USA) and in part by a General Clinical Research Center grant number M01 RR00043 from NIH (USA).
Acknowledgements
We thank Dr. Arthur D. Riggs for his critical reading of the manuscript. We thank Drs. Christine Chen and Elizabeth Lobo in our laboratory for their support, Dr. Shu Mi in the Clinical Immunobiology Correlative Studies Laboratory at City of Hope for her support in the cytokine and chemokine assays.