
Abstract
Protective effect of hydrogen (H2) gas on cardiac ischemia-reperfusion (I/R) injury has been demonstrated previously. This study was designed to test the hypothesis that hydrogen-rich saline (saline saturated with molecular hydrogen), which is easy to use, induces cardioprotection against ischemia (30 min) and reperfusion (24 h) injury in rats. Adult male Sprague-Dawley rats underwent 30-min occlusion of the left anterior descending (LAD) coronary artery and 24-h reperfusion. Intraperitoneal injection of hydrogen-rich saline before reperfusion significantly decreased plasma and myocardium malondialdehyde (MDA) concentration, decreased cardiac cell apoptosis, and myocardial 8-hydroxydeoxyguanosine (8-OHdG) in area at risk zones (AAR), suppressed the activity of caspase-3, and reduced infarct size. The heart function parameters including left ventricular systolic pressure (LVSP), left ventricular diastolic pressure (LVDP), +(dP/dt)max and −(dP/dt)max were also significantly improved 24 h after reperfusion. It is concluded that hydrogen-rich saline is a novel, simple, safe, and effective method to attenuate myocardial I/R injury.
Introduction
Currently, restoring blood flow in an acutely occluded vessel represents the most effective, long-term clinical therapy for acute myocardial infarction (AMI) (1). Although restoration of blood flow is critical, the reintroduction of molecular oxygen triggers a cytotoxic cascade during which reactive oxygen species (ROS) are generated by the mitochondria. This burst of reactive oxygen species irrevocably drives downstream signaling networks that lead to cellular necrosis and apoptosis, which is named lethal reperfusion injury (2). Reperfusion injury accounts for up to 50% of the final size of the infarct (3), providing an important potential target for protection of the heart.
The central role of ROS in reperfusion injury has been well demonstrated in recent studies showing that inhibitors of mitochondrial respiratory complexes I and III prevent reperfusion ROS generation and improve cellular viability (4–6). However, therapy to reduce free radicals during early reperfusion failed to relieve this pathological cascade of oxidative damage after reperfusion injury (7, 8). A recent article demonstrated that molecular hydrogen (H2) is a novel antioxidant agent which confers protection in focal brain ischemia reperfusion injury (9). This observation was echoed by others in different organs such as in I/R injury in intestine (10), liver (11), and heart (12) through the inhibition of oxidant stress. In a neonatal hypoxia–ischemia rat model, we have demonstrated that inhalation of hydrogen reduced apoptosis of brain cells (13).
In the current study, we tested whether hydrogen-rich saline, which is easy to use, safe, and economical, confers cardioprotection against myocardial ischemia reperfusion injury in rats. We evaluated specifically the reduction of infarction, the oxidative stress, and improvement of functions at 24 h after intraperitoneal injection of hydrogen-rich saline.
Materials and Methods
All the protocols were approved by the Second Military Medical University, China, in accordance with the Guide for Care and Use of Laboratory Animals published by the US NIH (publication No. 96–01). Adult male Sprague-Dawley rats weighing 250–280 g were used in all experiments. The animals were housed in individual cages in a temperature-controlled room with a 12-h light/dark cycle and free access to food and distilled water.
Hydrogen-Rich Saline Production.
Hydrogen was dissolved in physiological saline for 6 h under high pressure (0.4 MPa) to a supersaturated level using hydrogen-rich saline-producing apparatus produced by our department. The saturated hydrogen saline was stored under atmospheric pressure at 4°C in an aluminum bag with no dead volume. Hydrogen-rich saline was sterilized by gamma radiation and freshly prepared every week, which ensured that a concentration of 0.6 mmol/L was maintained. Gas chromatography was used to confirm the content of hydrogen in saline by the method described by Ohsawa et al. (9).
In Vivo Coronary Artery Occlusion.
Rats were intraperitoneally anesthetized with chloral hydrate (300mg/ kg). The rats were intubated and ventilated with a small-animal ventilator. Briefly, the hearts were exposed through a left thoracotomy in the fourth intercostal space. The pericardium was opened, and a 5.0-prolene suture was tightened around the proximal left anterior descending (LAD) coronary artery (before the first branch of diagonal artery); after 30 min of ischemia, the tube for the myocardial reperfusion was removed. Then, the muscle layer and the skin were closed separately and the animals were allowed to recover.
Experimental Protocol.
Animals were randomly assigned to four groups: Sham, Sham+H2, Control, and H2. There were 18 animals in Sham, Control, and H2 group: 6 for the measurement of infarct size, 6 for histological and immunohistochemical studies, and 6 for the measurement of the caspase-3 activity and MDA concentration. The Sham+H2 group (n = 6) was just for the measurement of hemodynamic parameters. In the Sham group, the ligature was placed under the LCA without occlusion for 30 min. In the Sham+H2 group, the ligature was placed under the LCA without occlusion for 30 min and hydrogen-rich saline (5ml/ Kg) was intraperitoneally injected into rats 25 min after placing the ligature. In the Control group, the LAD was reversibly occluded for 30 min and saline water (5ml/Kg) was intraperitoneally injected at 5 min before the reperfusion. In the H2 group, the LAD was reversibly occluded for 30 min. Hydrogen-rich saline (5ml/Kg) was intraperitoneally injected into rats 5 min before the reperfusion. The reperfusion was continued for 24 h in all experiments.
Hemodynamic Measurements.
Hemodynamic measurements were adapted from our previous study (14). Rats were intraperitoneally anesthetized with chloral hydrate (300mg/Kg) 24 h after ischemia reperfusion. A small incision was made to the right of the midline in the neck. The right carotid artery was identified and a PE 50 catheter was introduced into the artery. The proximal end of the catheter was connected to a low pressure transducer. The inserted tip of this catheter was advanced down until it reached the left ventricular lumen and the left ventricular pressure (LVP) signal was obtained. The pressure signals were monitored, analyzed, and recorded in real time. Heart rate (HR), LVSP, LVDP, and ±(dP/dt)max were all calculated from the continuously obtained LVP signal.
Since we used fluid-filled catheters to get the signal, end-diastolic pressure was difficult to measure accurately; LVDP represents minimum diastolic pressure here.
Infarct Size Determination.
The suture around the coronary artery was retied 24 h after reperfusion and 2% Evans blue dye was infused into the heart through the apex to mark the AAR as unstained (not blue) tissue. The hearts were excised and placed in a −20°C freezer for 30 min. Frozen hearts were then cut into 2-mm thick slices parallel to the atrioventricular groove. Sections were thawed and incubated in a 1% tetrazolium chloride (TTC) phosphate-buffered solution (pH 7.4) at 37°C for 15 min and fixed in 10% formalin to increase the contrast of the Evan’s blue and TTC staining. Tissue sections were compressed to a uniform 2-mm thickness by placing them between two glass plates separated by a 2-mm space. The viable tissue was stained red with TTC, while the dead tissue (infarcted tissue) was unstained. The infarct size was calculated as a percentage volume of the infarct area (white area) versus the AAR (non-blue area).
Determination of MDA Concentration in Plasma and Myocardium.
Plasma MDA concentration, a presumptive marker of oxidant-mediated lipid peroxidation, was quantified to estimate the extent of lipid peroxidation in the AAR myocardium (15). Arterial blood samples (0.6ml) were collected after 24 h of reperfusion. MDA product has a long half-life in plasma, and its levels are therefore cumulative. These samples were immediately centrifuged at 2500 rpm and 4°C for 10 min, and the plasma was stored at −80°C until analyzed. To measure the MDA concentration in AAR, 2 ml of 1% Evan’s blue dye was infused into the heart through the apex to mark the AAR as unstained (not blue) tissue. Then, the AAR was saved for analysis, and the samples were stored at −80°C until assayed. In brief, transmural tissue from AAR was homogenized in buffer and centrifuged. After determining protein concentration, the MDA concentration was measured using a commercial kit (Jianchen Biological Institute, China) and expressed as μmol/g protein.
Caspase-3 Activity.
Caspase-3 activity was determined using a Fluorometric Assay Kit (BIOVISION Research Products, 980 Linda Vista Avenue, Mountain View, CA), according to the manufacturer’s instructions. In brief, 20–200μg cell lysates of AAR were incubated in a 96-well plate with 2×Reaction Buffer (50μl). The reaction was started by adding 1mM DEVD–APC substrate (5μl). After incubation in the dark at 37°C, the plate was read in a fluorometer equipped with a 400-nm excitation filter and a 505-nm emission filter. Fold-increase in caspase-3 activity was determined by comparing these results with the level of the uninduced control.
Histological and Immunohistochemical Studies.
The hearts were harvested, sectioned, and immersion-fixed in 4% buffered paraformaldehyde. The paraffin was cut into 4-μm thick serial sections. The standard deparaffinization protocol was used.
Hematoxylin–Eosin (H&E) Staining.
Tissues were stained with hematoxylin–eosin. Slides were then assessed in a blinded fashion by a pathologist and scored for the following: myodegeneration, cardiomyocyte hydropic changes, neutrophilic infiltrate, hemorrhage, lymphohistio-cytic infiltrate, and acute myocardial necrosis.
In Situ Apoptosis Assay.
TUNEL staining was performed on paraffin-embedded sections by using the in situ cell death detection kit (Roche). According to standard protocols, the sections were dewaxed and rehydrated by heating the slides at 60°C. Then, these sections were incubated in a 20-μg/ml proteinase K working solution for 15 min at room temperature. The slides were rinsed three times with PBS before they were incubated in TUNEL reaction mixture for 1 h at 37°C. Dried area around sample by filter paper and added Converter-AP on samples for 1 h at 37°C. After rinsing with PBS (5 min, three times), sections were coloured in dark with nitroblue tetrazolium (NBT) and 5-bromo-4-chloro-3-indolylphosphate (BCIP). Four slide fields were randomly examined using a defined rectangular field area with magnification (×40). One hundred cells were counted in each field. The data were represented as the percentage of TUNEL-positive cells of total cell nuclei per field.
Immunohistochemistry for Myocardial 8-OHdG.
The paraffin sections were deparaffinized in xylene, rehydrated using various grades of ethanol, and pretreated with 10 μg/ml proteinase K (to permeabilize the nucleus) for 30 min at 37°C. Nonspecific binding of immunoglobulins was blocked by incubating the sections in 10% BSA for 20 min. Then, the sections were incubated with primary goat polyclonal anti-8-OHdG antibody (Alpha Diagnostics) (1:200, overnight at room temperature), and secondary rabbit anti-goat lgG-HRP conjugated Cat #30220. Four slide fields were randomly examined using a defined rectangular field area with magnification (×40). 8-OHdG positive cells were counted in each field. The data were represented as the number of 8-OHdG positive cells per field.
Statistical Analysis.
All results were expressed as means ± SEM. For comparison of changes in hemodynamic parameters between groups, two-way ANOVA followed by Student-Newman-Keuls tests were utilized. For comparison of infarct size, MDA concentration, caspase-3 activity, apoptosis, and 8-OHdG, differences between groups were determined with a one-way ANOVA followed by Student-Newman-Keuls tests. A value of P < 0.05 was considered to denote statistical significance.
Results
Hemodynamic Measurements.
The result of AN-OVA revealed significant interactions between hydrogen-rich saline and myocardial ischemia reperfusion on all the hemodynamic parameters (P < 0.05). As displayed in Figure 1, the hemodynamic parameters remained unchanged with hydrogen-rich saline alone (Sham+H2 group). The intraperitoneal injection of hydrogen-rich saline, however, decreased the I/R-induced degrading of hemodynamic parameters including LVSP, LVDP, +(dP/dt)max, and − (dP/dt)max. All of the hemodynamic parameters, except LVDP, in both the Control and H2 groups were significantly lower than those in the Sham or Sham+H2 groups. There were no significant differences in LVDP between the H2 group and Sham group (P > 0.05). No statistical difference was found for heart rate after 24 h of ischemia reperfusion (data not shown).
Measurement of Infarct Size.
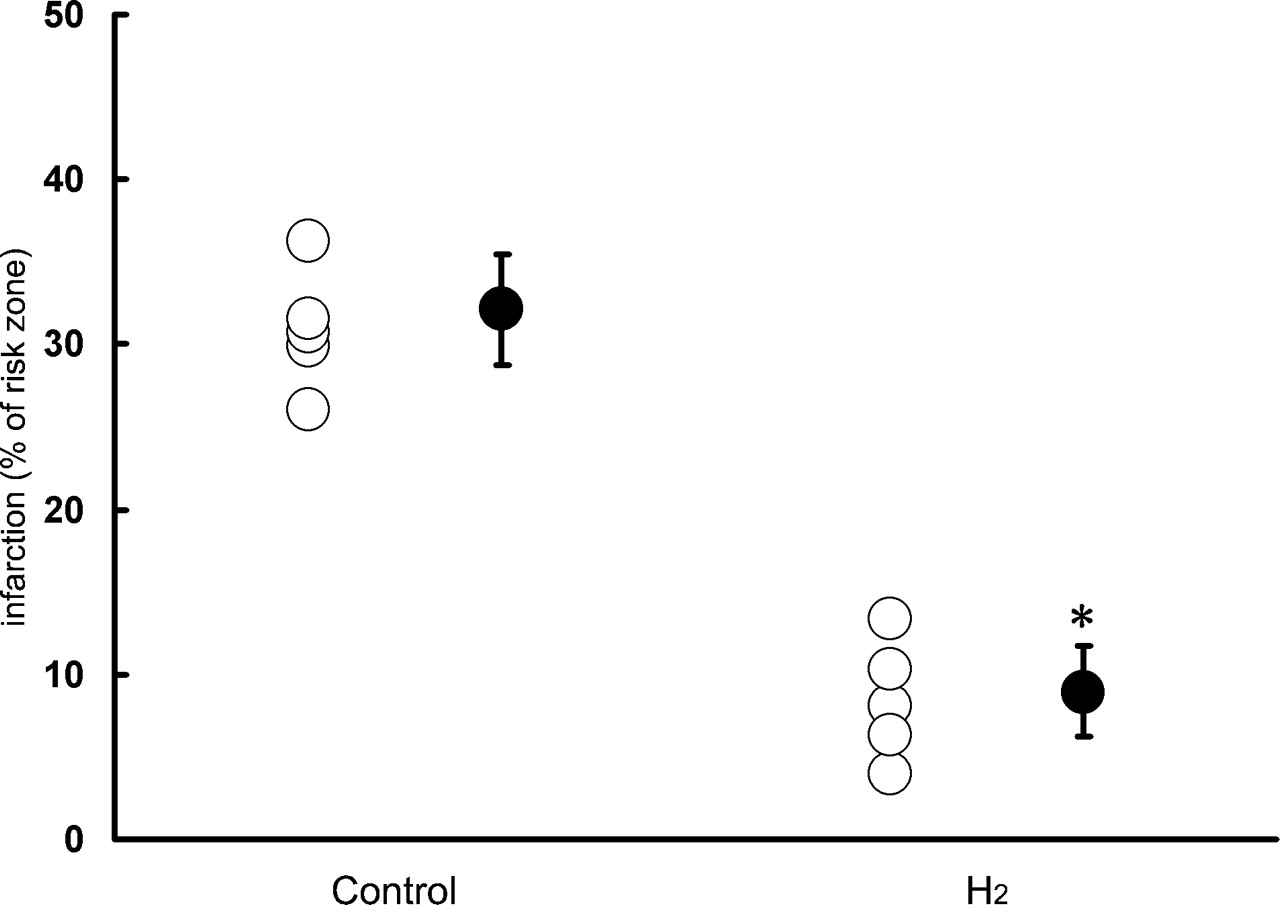
The infarct size in the H2 group was significantly smaller than in the Control group (9.8 ± 3.6% vs. 32.1 ± 3.4%, * P < 0.01), as shown in Figure 2 and Figure 3. There was no significant difference in AAR/LV between the Control group and H2 group (62 ± 4.7% vs. 58 ± 3.9%).
Plasma and Myocardium MDA Concentration after Reperfusion.
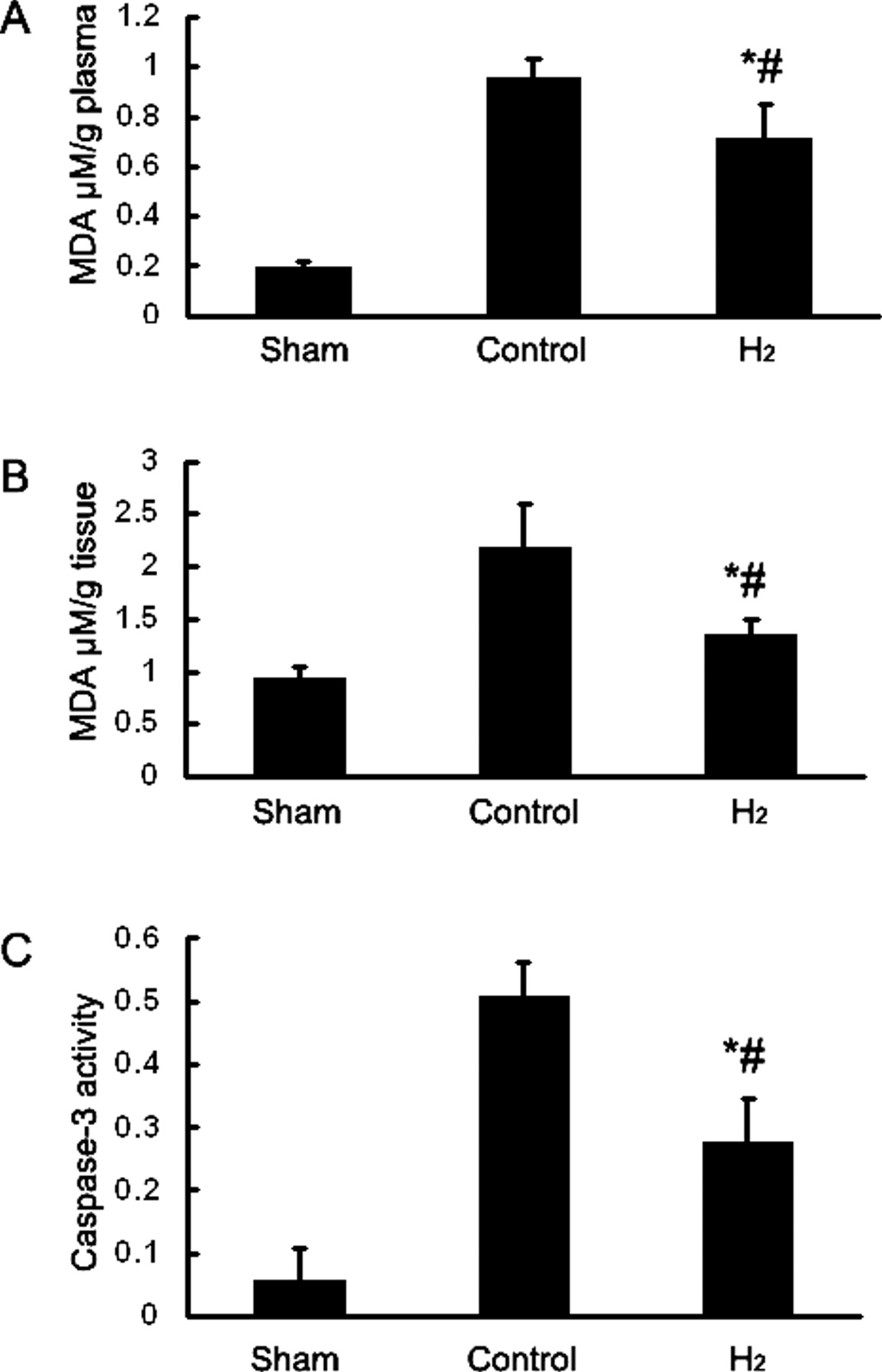
The plasma MDA concentration was measured at 24 h of reperfusion (Fig. 4A). Plasma MDA concentration at 24 h of reperfusion in the H2 group was significantly lower than that of the Control group. The myocardium MDA concentration was also measured at 24 h of reperfusion (Fig. 4B). Myocardium MDA concentration at 24 h of reperfusion in the H2 group was significantly lower than that of the Control group.
Caspase-3 Activity.
The caspase-3 activity is shown in Figure 4C. I/R significantly increased caspase-3 activity relative to the nonischemic myocardium. H2 comparably reduced caspase-3 activity relative to the Control group.
Histopathological Examination by H&E Staining.
Blinded histological analysis of heart sections stained with H&E was scored 24 h after reperfusion (Fig. 5). Rats in the H2 group displayed a reduced degree of myocardial neutrophilic infiltrate, necrosis, hemorrhage, and spindle-shaped interstitial cells as compared with rats in the Control group.
Detection of Apoptotic Cell Death.
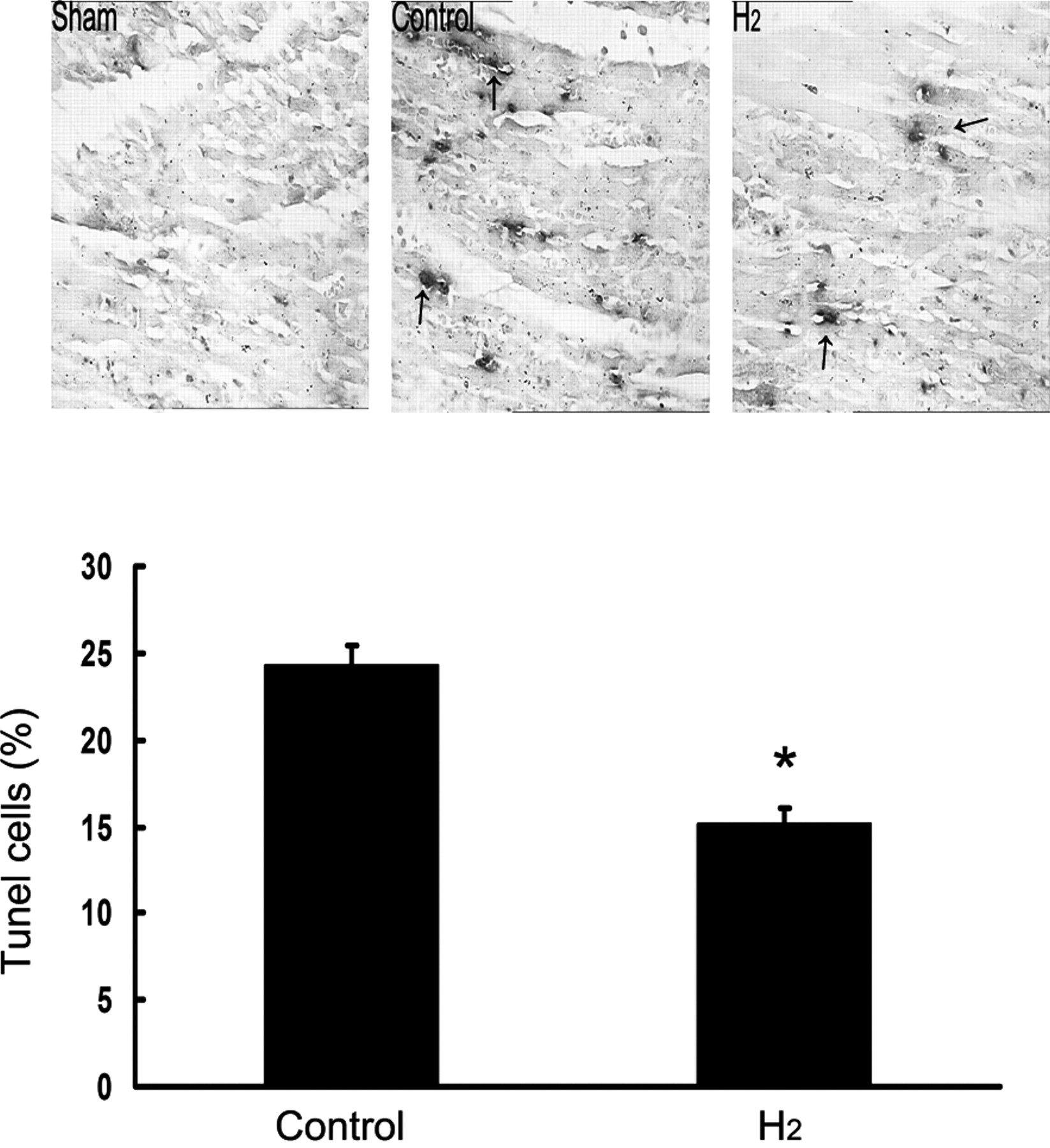
As shown in Figure 6, the number of TUNEL-positive cells was increased in the AAR myocardium in the Control group. H2 comparably decreased the frequency of TUNEL-positive cells relative to the Control group (15 ± 1% vs. 24 ± 1%, * P < 0.05 vs. Control group).
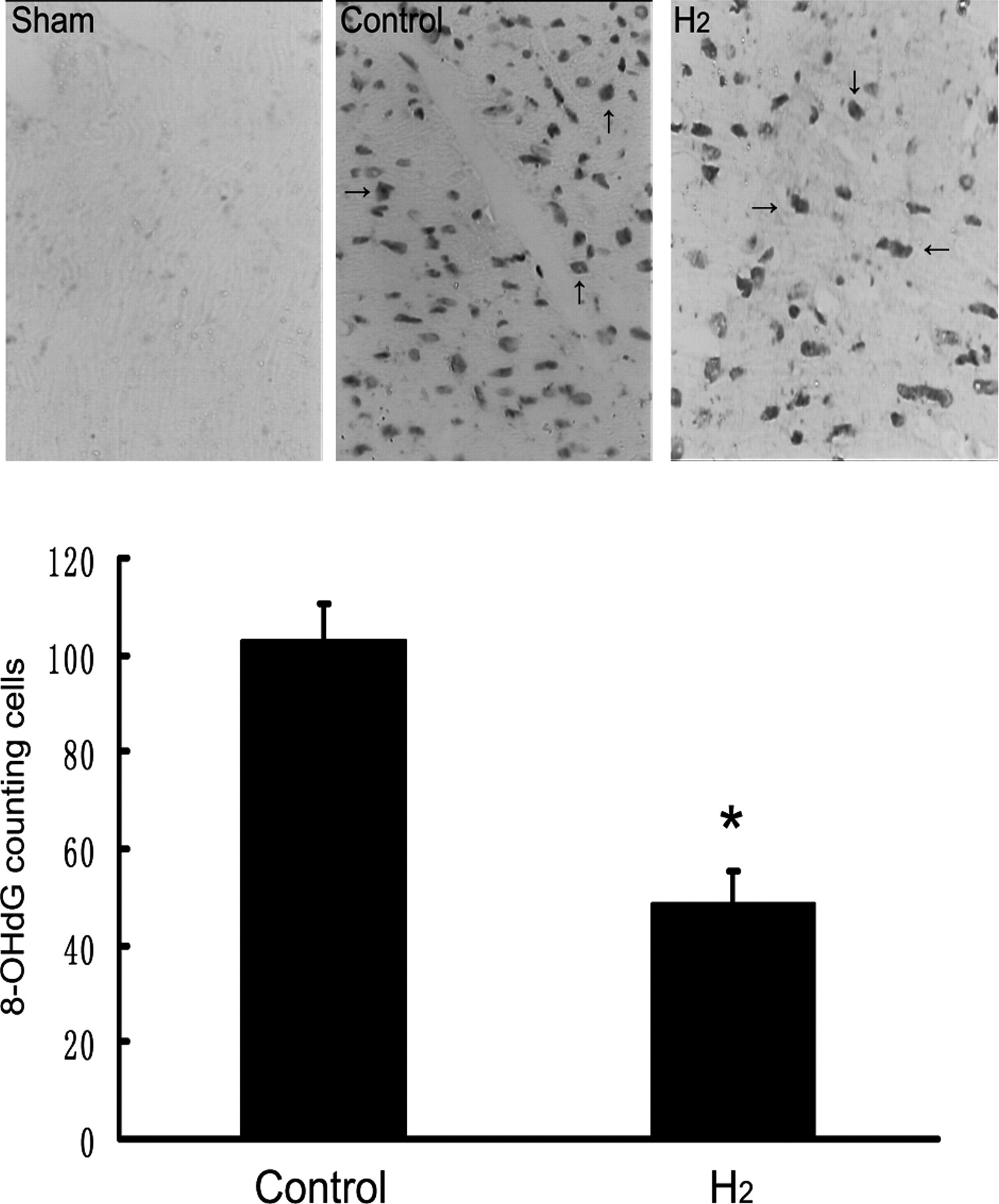
Detection of 8-OHdG Positive Cell Death.
As shown in Figure 7, the numbers of 8-OHdG positive cells were increased in the AAR myocardium in the Control group. H2 comparably decreased the number of 8-OHdG positive cells relative to the Control group (49 ± 7 vs.103 ± 8, * P < 0.01 vs. Control group).
Discussion
As we are aware, this is the first study demonstrating that hydrogen-rich saline significantly improved post-ischemic functional recovery of rat hearts. The improvement in post-ischemic functional recovery was paralleled by a significant reduction in infarct size, decreased plasma and myocardium MDA concentration, attenuation of cardiac cell apoptosis and DNA oxidative stress in AAR. Histological analysis revealed a substantial decrease in hemorrhage and necrosis as well as a decrease in the number of leukocytes within the ischemic zone. This cardiac improvement may result from radical oxygen species (ROS) scavenging effect of molecular H2, as previously reported in a brain injury model (9).
ROS are produced on reperfusion of ischemic myocardium, and are considered a major cause of lethal reperfusion injury (17–19). Radical oxygen species O2− and H2O2 are detoxified by antioxidant defense enzymes, unlike ·OH and ONOO−, which so far no enzyme could detoxify. Recently it was demonstrated that hydrogen gas selectively reduces these two detrimental ROS (9). Since the hydrogen molecule is electrically neutral and much smaller than the oxygen molecule, it easily penetrates membranes and enters cells and organelles such as the nucleus and mitochondria. This is particularly important, as the latter is the primary site of generation of reactive oxygen species after reperfusion and is notoriously difficult to target (20). Since the heart is one of the most highly perfused tissues, it is possible that the intramyocardial H2 concentration increases immediately following intraperitoneal injection of hydrogen-rich saline. 8-OHdG is formed from deoxyguanosine in DNA by hydroxyl free radicals and might serve as a sensitive biomarker of intracellular oxidative stress in vivo (21). Our findings show that hydrogen-rich saline reduced the level of 8-OHdG positive cells in AAR. Meanwhile, we found reduced MDA concentration in both the plasma and myocardium in the H2 group. In the current study, one may speculate that at the onset of reperfusion, H2 reduces ROS generation and preserves mitochondrial membrane potential, maintains ATP synthesis, prevents DNA damage, and decreases lipid peroxidation, and thus protects the heart. One of the intensive mechanisms underlining the protective effect may be the inhibition of the opening of the permeability-transition pore. At the time of reperfusion after prolonged ischemia, abrupt high accumulation of calcium and overproduction of reactive oxygen species trigger the opening of the pore (22, 23). The resulting collapse of the membrane potential, uncoupling of the respiratory chain, efflux of pro-apoptotic factors, and hydrolysis of ATP may ultimately cause irreversible damage. Although it has been reported that necrosis, as a major form of pathological cell death, leads to a destruction of a large portion of cardiomyocytes after myocardial ischemia and reperfusion, an attenuation of myocardial apoptosis has been associated with an inhibition in extension of infarct size at late phase of reperfusion (24). Consistent with previous reports, in the present study we find treatment with hydrogen-rich saline inhibited activation of down-stream caspase-3 and reduces apoptosis cardio-myocytes, providing evidence that limitation in reperfusion injury can be achieved by hydrogen-rich saline when it is only applied at 5 min before reperfusion.
Recently, supplementation with hydrogen-rich pure water via gastric intestine has shown beneficial effects on lipid and glucose metabolism in humans by providing protection against oxidative stress (25). Hydrogen-rich water decreases superoxide formation caused by ischemia–reperfusion in the brain slices of mice (26). Our laboratory proved neuroprotective effects of hydrogen saline in a neonatal hypoxia-ischemia rat model (27). In this study, intraperitoneal injection of hydrogen-rich saline 5 min before reperfusion had a similar effect compared to inhalation of H2. The improved heart function and reduced infarct size demonstrated the preserved state of heart after ischemic insult, along with a reduction of oxidative stress and less cell death. Therefore, the current study supports other observations and for the first time indicates that hydrogen-rich saline is an effective alternative pharmacological strategy in myocardial ischemia reperfusion management. Our results indicate hydrogen-rich saline may induce protective effects through the anti-oxidative stress and apoptotic pathways.
Use of flammable hydrogen gas is associated with hazards due to violent reactions of hydrogen with oxidizing elements such as chlorine and fluorine. Hydrogen is a highly diffusible gas and reacts with hydroxyl radical to produce water (16), and thus is an ROS scavenger. Hydrogen gas cannot be produced by the human body since mammalian cells lack the hydrogenase activity (28). However, it is continuously produced by colonic bacteria in the body and normally circulates in the blood (29), so it is physiologically safe for humans to inhale hydrogen at a relatively low concentration. Medical use of hydrogen in the past was limited to test the effects of antibiotic therapy (30). Previously, other therapeutic strategies for scavenging reactive oxygen species seemed promising in animal models, but most of them failed in human clinical trials (31). Hydrogen-rich saline may, on the basis of our observation, offer a simple, easy to use, safe, and economic novel approach for future cardiac protection.
The changes of LVDP, LVSP, +(dP/dt)max and − (dP/dt)max after 24 h of ischemia reperfusion. Results are expressed as means ± SEM (n = 6, * P < 0.01 relative to Sham group, # P < 0.05 relative to Control group). Representative photographs of serial heart sections obtained from rats subjected to myocardial ischemia–reperfusion injury in the presence or absence of hydrogen-rich saline injection. A color version of this figure is available in the online journal. Infarct size as a % of AAR. Individual points are represented by open circles and group means by filled-in circles. H2-dependent reduction in infarct size is expressed as a percentage volume of the infarct area versus the AAR (n = 6 for each group, * P < 0.01 compared to Control group). (A) Plasma MDA concentration at the end of 24 h of reperfusion. H2 significantly reduced MDA concentration (n = 6, * P < 0.05 compared to Control group; # P < 0.01 relative to Sham group). (B) Myocardium MDA concentration at the end of 24 h of reperfusion. H2 significantly reduced MDA concentration (n = 6, * P < 0.05 compared to Control group; # P < 0.05 relative to Sham group). (C) Caspase-3 activity in the Sham, Control, and H2 groups at the end of 24 h of reperfusion (n=6, * P < 0.05 compared to Control group; # P < 0.01 relative to Sham group). Representative H&E-stained histological images after 30 min of LCA ischemia and 24 h of reperfusion. Rats in the Control group displayed a high degree of hemorrhage and infiltrating leukocytes within the ischemic zone. Histopathology was attenuated in the myocardial sections of rats treated with hydrogen-rich saline. A color version of this figure is available in the online journal. Detection of apoptotic cell death by TUNEL staining in the Sham, Control, and H2 groups at the end of 24 h of reperfusion. Relative to the Control group, H2 significantly reduced the number of TUNEL-positive cells (blue staining). Values are mean ± SEM; * P < 0.01 compared to Control group, n = 6 for each group. Oxidative DNA damage assessed by 8-OHdG immunoreactivity. Staining was localized to nuclei of myocardium in AAR. Shown are, at the end of 24 h of reperfusion, 8-OHdG positive cells in the Sham, Control, and H2 groups. Relative to the Control group, H2 significantly reduced the number of 8-OHdG positive cells (brown staining) per field. Values are mean ± SEM; * P < 0.01 compared to Control group, n =6 for each group.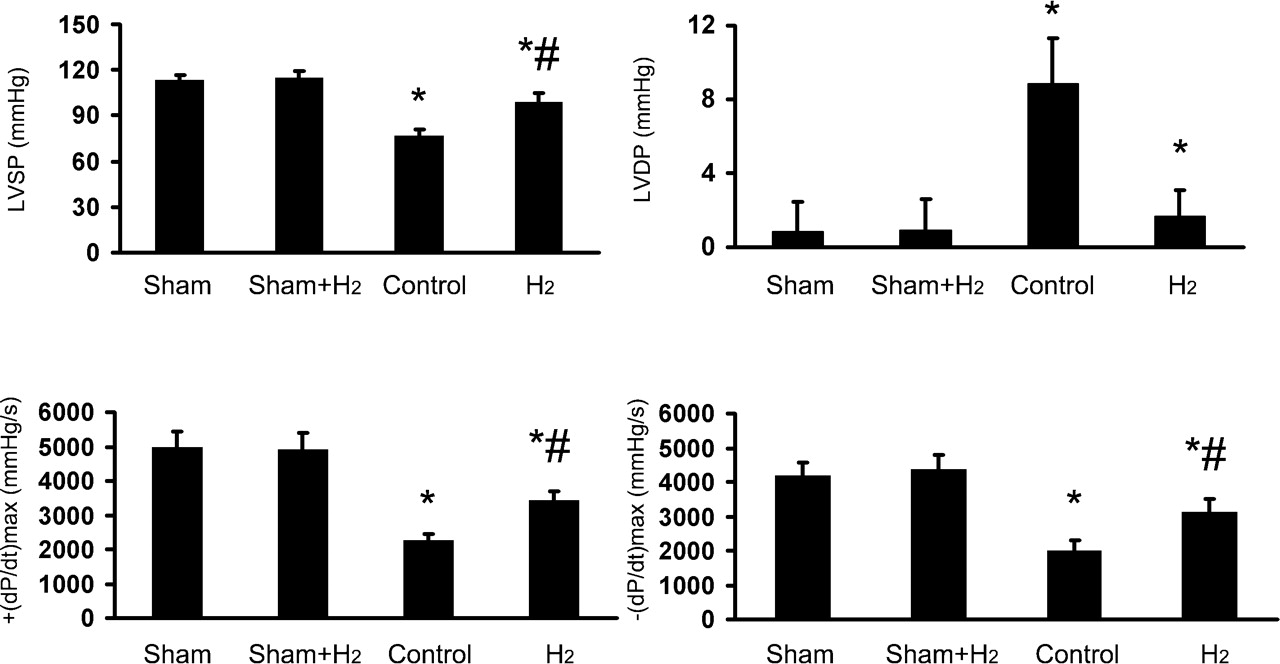


Footnotes
This study was supported by grant from the National Natural Science Foundation of China (No. 30500579).