
Abstract
The murine in vivo model of acute myocardial infarction is increasingly used to investigate anesthetic-induced preconditioning (APC) and postconditioning (APOST). However, in mice the potency of different volatile anesthetics to reduce myocardial infarct size (IS) has never been investigated systematically nor in a head to head comparison with regard to ischemic preconditioning (IPC) and postconditioning (IPOST). Male C57BL/6 mice were subjected to 45 min of coronary artery occlusion (CAO) and 180 min of reperfusion. To induce APC, 1.0 MAC isoflurane (ISO), sevoflurane (SEVO) or desflurane (DES) was administered 30 min prior to CAO for 15 min. In an additional group, ISO was administered 45 min prior to CAO for 30 min. To induce APOST, 1.0 MAC ISO, SEVO or DES was administered for 18 min starting 3 min prior to the end of CAO. IPC was induced by 3 or 6 cycles of 5 min ischemia/reperfusion, 40 or 60 min prior to CAO, respectively. IPOST was induced by 3 cycles of 30 sec reperfusion/ischemia at the beginning of reperfusion. Area at risk (AAR) and IS were determined with Evans Blue and TTC staining, respectively. IS (IS/AAR) was 50 ± 4% (mean ± SEM) in the control group and was significantly (*P < 0.05) reduced by 3×5 IPC (26 ± 3%*), 6×5 IPC (26 ± 4%*), IPOST (20 ± 2%*), ISO APOST (19 ± 1%*), SEVO APOST (15 ± 1%*), DES APOST (14 ± 2%*) and SEVO APC (27 ± 6%*). ISO APC significantly reduced IS compared to control when administered 30 min (33 ± 4%*), but not when administered 15 min (48 ± 6%). DES APC significantly reduced IS compared to control and to SEVO APC (7 ± 1%*). Within the paradigm of preconditioning, the potency of volatile anesthetics to reduce myocardial infarct size in mice significantly increases from ISO over SEVO to DES, whereas within the paradigm of postconditioning the potency of these volatile anesthetics to reduce myocardial infarct size in mice is similar.
Introduction
Considerable evidence has accumulated from laboratory (1–4) and clinical (5, 6) investigations that volatile anesthetics induce myocardial preconditioning and postconditioning and confer protection against the sequelae of myocardial ischemia/reperfusion injury. Numerous experimental in vivo studies have been published investigating the mechanisms of anesthetic-induced preconditioning (APC) and postconditioning (APOST) in dogs, rabbits and rats (conf. (7, 8)). Mice promise to be used increasingly to investigate the mechanisms underlying APC and APOST as this species provides the striking possibility of over-expression or disruption of specific genes. However, published data on APC and APOST in mice are scarce.
Isoflurane (9, 10) and desflurane (11) have recently been demonstrated to induce preconditioning against myocardial infarction in mice in vivo. The extent of infarct size reduction by desflurane was 86% (11) and markedly exceeded the infarct size reduction by isoflurane (33%) (10). It is currently unclear whether different experimental protocols in different laboratories account for this discrepancy in magnitude of infarct size reduction or whether there is a different potency of volatile anesthetics to induce myocardial preconditioning.
Studies investigating APC and APOST in mice using different volatile anesthetics cannot be compared since to our knowledge there is no study reporting a head to head comparison of the potency of volatile anesthetics to reduce infarct size in the murine in vivo model of acute myocardial infarction. Therefore, the goal of the current study was to compare the infarct-sparing potency of isoflurane-, sevoflurane- and desflurane-induced pre- and postconditioning at 1.0 minimum alveolar concentration (MAC) with regard to ischemic pre- and postconditioning.
Methods
Animals.
Male C57BL/6 mice (8–12 weeks) were used for all experiments (Charles River Laboratories, Sulzfeld, Germany). The animals were housed under controlled conditions (22°C, 55–65% humidity and 12-h light-dark cycle) and were allowed free access to tap water and standard laboratory chow.
All experimental procedures and protocols used in this investigation were reviewed and approved by the Animal Care and Use Committee of the Government of Lower Franconia, Bavaria, Germany. All experiments conformed to the Guiding Principles in the Care and Use of Animals of the American Physiological Society and were in accordance with the Guide for the Care and Use of Laboratory Animals (12).
Instrumentation and Surgical Procedure.
Instrumentation for hemodynamic measurements and ligature of the left coronary artery (LAD) was performed as described previously (13). Briefly, after induction of anesthesia with pentobarbital (60 mg/kg) and endotracheal intubation, the mice were mechanically ventilated with a mixture of 50% air/50% oxygen using a rodent ventilator (SAR 830/AP, CWE Inc., Ardmore, PA, USA). A 3-lead needle-probe ECG was attached and a saline filled PE-10 catheter was inserted into the right common carotid artery and the right jugular vein, respectively. After left thoracotomy at the 4th intercostal space, the LAD was exposed and a 6–0 silk suture was passed around the LAD. Coronary artery occlusion (CAO) was achieved using the hanging weight system (14) and was verified by paleness of the myocardial area at risk, changes in color of the LAD distal to the ligature from bright red to violet, and ECG ST-segment elevation. Reperfusion was verified by reversion of these criteria.
After completion of the surgical procedures all animals were allowed a time-matched equilibration period. Myocardial ischemia was induced by coronary artery occlusion (CAO) for 45 min followed by 180 min of reperfusion.
Experimental Protocols.
The experimental protocol of each group is illustrated in Figure 1.
In a first set of experiments, the animals were randomly assigned to 9 groups. The CON group received no further treatment prior to and after CAO. The IPC 3×5 group received 3 cycles of 5 min ischemia/5 min reperfusion, 40 prior to CAO. In the APC ISO, APC SEVO and APC DES groups, 1.0 MAC isoflurane (Forane®, Abbott, Wiesbaden, ermany; 1.3 Vol-% (15)), 1.0 MAC sevoflurane (Sevorane®, Abbott, Wiesbaden, Germany; 3.4 Vol-% (16)) and 1.0 MAC desflurane (Suprane®, Baxter, Unterschleiβheim, Germany; 7.5 Vol-% (15)), respectively, was administered 30 min prior to CAO for a 15 min duration.
In the IPOST group, three cycles of 30 sec reperfusion/ 30 sec CAO were applied at the beginning of reperfusion. In the APOST ISO, APOST SEVO and APOST DES groups, 1.0 MAC isoflurane, 1.0 MAC sevoflurane and 1.0 MAC desflurane, respectively, was administered for 18 min, starting 3 min prior to the end of CAO.
In a second set of experiments, the animals were randomly assigned to 2 additional groups. To investigate whether infarct size reduction by three cycles of ischemic preconditioning is maximum for ischemic preconditioning, the preconditioning stimulus was doubled to 6 cycles of 5 min ischemic preconditioning 60 min prior to CAO (IPC 6×5). To investigate whether isoflurane induces preconditioning after prolongation of administration duration, 1.0 MAC isoflurane was administered 45 min prior to CAO for 30 min in the APC ISO 30′ group.
In all animals receiving volatile anesthetics, the concentration of the volatile anesthetic was gradually increased from 0.0 to 1.0 MAC and gradually decreased from 1.0 to 0.0 MAC over a time period of 2 min.
Measurement of Myocardial Infarct Size.
Myocardial infarct size (IS) and area at risk (AAR) were determined as described previously (17). Briefly, after reperfusion, the LAD was re-occluded and 1 ml Evans Blue (0.1 g/ml; Sigma-Aldrich, Taufkirchen, Germany) was slowly injected into the carotid artery to delineate the AAR. After injection of a lethal dose of pentobarbital (150 μg/g i.p.) the heart was rapidly removed. The left ventricle was dissected and cut into 8 transverse slices of 1 mm thickness, using an acrylic heart matrix (Aster Industries, McCandles, PA, USA). All slices were incubated with 2% triphenyltetrazolium chloride (TTC, Sigma Aldrich, Taufkirchen, Germany), fixed overnight in 10% formalin, weighed and digitally photographed (Finepix S3 Pro, Fujifilm, Tokyo, Japan). The photographs were then analyzed with a picture analysis software (Adobe Photoshop CS 8.0.1; Adobe Systems Inc., San Jose, CA, USA) and infarcted area (IA), AAR and normal zone (NZ) were quantified by an investigator blinded to the treatment protocol. The resulting fractions of IA, AAR and NZ of each slice were multiplied by the weight of the slice. Infarct size was calculated by the following formula: infarct size = weight of infarcted area/ weight of area at risk × 100 (IS =IA/AAR × 100). Animals with an AAR less than 20% of the left ventricle were excluded from further analysis.
Data Acquisition and Statistical Analysis.
Hemodynamic parameters, ECG, and body temperature were continuously recorded at a sampling rate of 1000 Hz and analyzed on a personal computer (Fujitsu Siemens, Augsburg, Germany) using hemodynamic data acquisition and analysis software (Notocord® hem 3.5, Croissy sur Seine, France).
Statistical analysis of data within and between groups was performed with one-way and two-way analysis of variance (ANOVA) followed by post hoc Duncan test using SPSS 16.0.1 software (The Apache Software Foundation, Forest Hill, MD, USA). Changes were considered statistically significant if P was less than 0.05. All data are expressed as mean ± SEM.
Results
A total of 88 mice were assigned to the ischemia-reperfusion experiments. Three animals were excluded from the study due to an AAR less than 20% (1 in IPC 3×5, 1 in IPOST) or due to pump failure during coronary artery occlusion (1 in APC ISO).
Hemodynamic parameters at baseline (Table 1), body weight and area at risk (Table 2) were not significantly different between groups.
Three cycles of ischemic preconditioning significantly reduced myocardial infarct size compared to control (Table 2 and Fig. 2). Fifteen minutes of isoflurane application did not reduce IS. In contrast, sevoflurane-induced preconditioning significantly reduced infarct size compared to control. Fifteen minutes of desflurane-induced preconditioning further reduced IS compared to control and to sevoflurane-induced preconditioning.
Six cycles of ischemic preconditioning significantly reduced myocardial IS compared to control (Table 2). However, compared to three cycles of ischemic preconditioning IS was not further reduced.
Preconditioning with 30 min administration of isoflurane significantly reduced IS compared to control and to preconditioning with 15 min administration of isoflurane (Table 2).
Ischemic and anesthetic-induced postconditioning all significantly reduced myocardial infarct size compared to control (Table 2 and Fig. 3). IS reduction was not different between the IPOST, APOST ISO, APOST SEVO and APOST DES groups.
Discussion
The present investigation systematically compares isoflurane-, sevoflurane- and desflurane-induced pre- and postconditioning with regard to ischemic pre- and postconditioning in the murine in vivo model of acute myocardial infarction. In conclusion, the results demonstrate that the potency of volatile anesthetics to induce preconditioning is significantly different, whereas their potency to induce postconditioning is not.
The sensitivity of murine myocardium to preconditioning was first reported by Guo et al. (18). In this study, ischemic preconditioning consisting of 6 cycles of 4 min ischemia-reperfusion prior to coronary artery occlusion reduced infarct size by 75%. In several subsequent studies infarct size reduction using different protocols of ischemic preconditioning was confirmed, whereas IS reduction ranged from 38% to 76% (14, 19–22). Infarct size reduction by ischemic preconditioning reported in the current investigation is in line with previously published data: ischemic preconditioning with 3 cycles of 5 minutes ischemia-reperfusion reduced infarct size by 47%. Increasing the preconditioning stimulus to 6 cycles of 5 min ischemia-reperfusion did not further decrease myocardial infarct size compared to 3 cycles. Thus, we conclude that in our experimental model ischemic preconditioning (IPC) reduces myocardial infarct size to a maximum of approximately 50%, an effect that cannot be further increased.
Infarct size reduction after 15 min administration of sevoflurane, discontinued 15 min prior to CAO, was similar compared to IPC. Preconditioning with desflurane resulted in a significantly smaller infarct size compared to sevoflurane-induced preconditioning and to ischemic preconditioning. This is in line with data obtained in rabbits (23): desflurane reduced myocardial infarct size by 70%, whereas infarct size reduction by sevoflurane was only 26%. It is of note that in mice anesthetic-induced preconditioning with desflurane results in greater infarct size reduction than ischemic preconditioning.
In the current study, isoflurane administered for 15 min did not reduce myocardial infarct size, whereas 30 min of isoflurane administration significantly reduced infarct size. The magnitude of infarct size reduction was similar compared to ischemic preconditioning and to 15 min of sevoflurane preconditioning. This observation might be of particular interest for murine studies on myocardial function and infarct size. More than often volatile anesthetics are used to maintain anesthesia for pharmacological or surgical interventions (conf. (24–31)). Isoflurane does not reduce myocardial infarct size when administered 15 min. Thirty minutes of isoflurane application and 15 min of sevoflurane or desflurane administration, however, induce preconditioning and should not be used for mouse anesthesia in cardiac investigations since myocardial infarct size might be reduced by the anesthetics.
In the current study, ischemic postconditioning reduced myocardial infarct size by 61%. In previous IPOST studies in mice infarct size reduction ranged from 33% to 44% after 3 × 60 sec, 3 × 20 sec and 3 × 10 sec of ischemic postconditioning, respectively (20, 30, 31). The difference in infarct size reduction might be explained by different durations of coronary artery occlusion and reperfusion, and by different mouse strains used in these studies.
Comparable to preconditioning, sevoflurane-induced postconditioning reduced myocardial infarct size to a similar extent compared to ischemic postconditioning. In contrast to preconditioning, infarct size reduction by isoflurane- and desflurane-induced postconditioning was not different from sevoflurane-induced postconditioning and ischemic postconditioning.
It is currently unclear why isoflurane, sevoflurane and desflurane reduce myocardial infarct size to a significantly different extent when administered prior to, but not after ischemia/reperfusion injury. Recent data from the rabbit model suggest that anesthetic-induced preconditioning is a threshold phenomenon (32). Above the threshold, infarct size reduction could not be increased neither by prolongation of desflurane administration nor by increase of MAC. In the current study, 30 min isoflurane preconditioning and 15 min sevoflurane preconditioning are stimuli above the threshold. For this reason, and because equal duration of isoflurane, sevoflurane and desflurane postconditioning reduces infarct size to the same extent, it seems unlikely that different durations of isoflurane, sevoflurane and desflurane to reach equilibrium are responsible for the different effects on infarct size in preconditioning. More likely, different signal transduction cascades are responsible for preconditioning and postconditioning, and these cascades may be activated differently by different volatile anesthetics. Further studies are needed to elucidate the underlying pathways and their detailed interaction with volatile anesthetics.
The results of the present study should be interpreted within the constraints of potential limitations. The left ventricular area at risk for myocardial infarction is an important determinant of the myocardial infarct size. However, the AAR was not different among experimental groups. TTC staining requires sufficient reperfusion to yield valid results (33). Mean arterial blood pressure trended to be lower in the APC DES group compared to the APC ISO and APC DES groups. However, since this difference was not significant it is unlikely that false positive TTC staining accounts for the significant infarct size reduction by desflurane preconditioning compared to isoflurane and sevoflurane preconditioning. A different impact on oxygen supply/demand ratio mediated by hemodynamic effects might contribute to IS reduction by volatile anesthetics. However, in the current study heart rate and mean arterial blood pressure were not different compared to CON and to baseline conditions during ischemic pre- and postconditioning and during the application of volatile anesthetics. Thus, it is unlikely that hemodynamic effects have confounded the results. However, coronary venous oxygen content was not measured, and myocardial oxygen consumption was not directly quantified in this investigation. Therefore, alterations in myocardial oxygen metabolism during and after administration of volatile anesthetics cannot be completely excluded as factors involved in the reduction of infarct size.
In summary, this study provides a comprehensive characterization of isoflurane-, sevoflurane- and desflurane-induced preconditioning and postconditioning in the murine in vivo model of acute myocardial infarction in relation to ischemic pre- and postconditioning. The application of sevoflurane for the duration of 15 min prior to or after coronary artery occlusion reduces infarct size to a similar extent compared to ischemic pre- and postconditioning, respectively. Compared to sevoflurane, isoflurane is less and desflurane is more efficacious within the paradigm of preconditioning, whereas all volatile anesthetics are equally efficacious within the paradigm of postconditioning.
Hemodynamic Parameters a
Body Weight and Infarct Size a
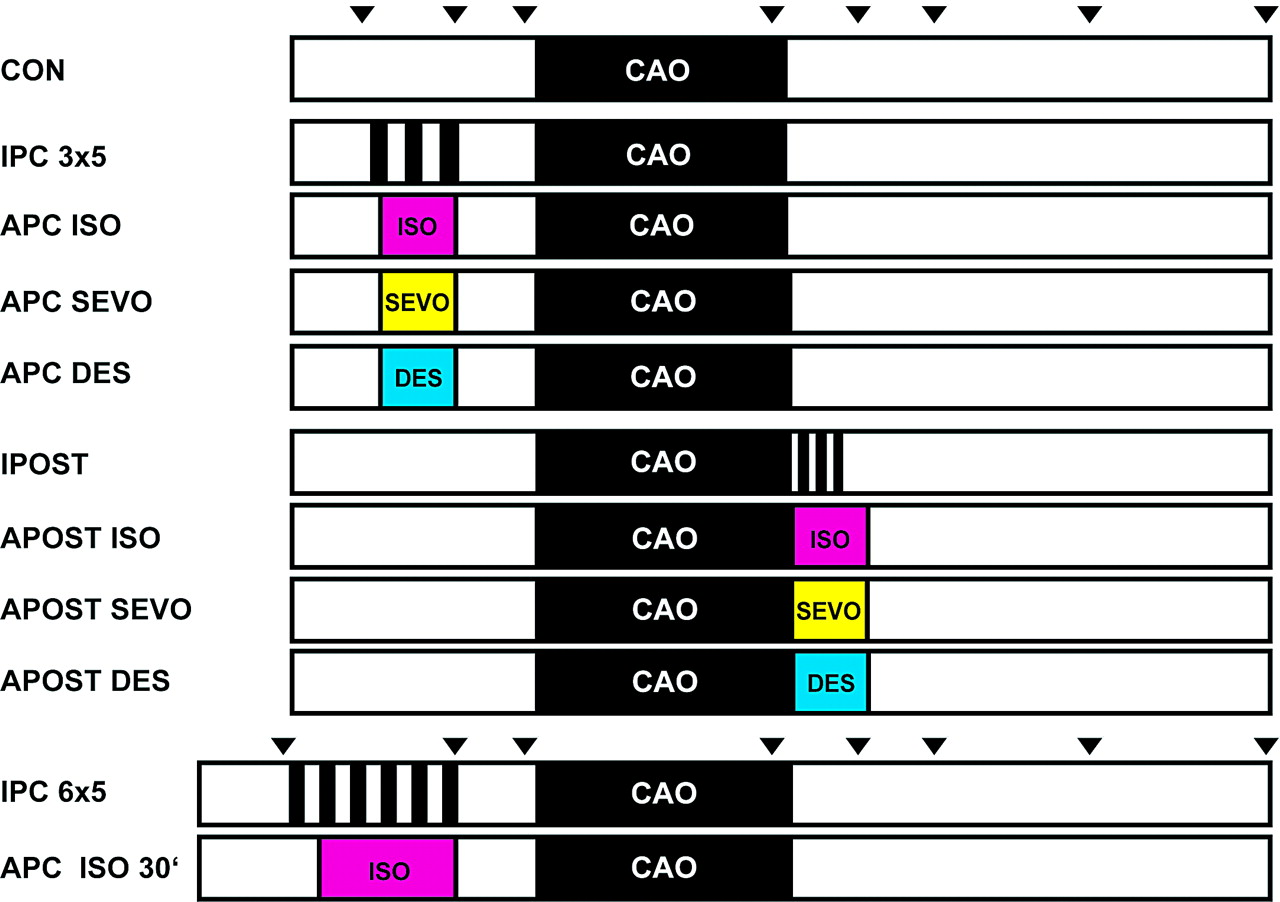
Schematic diagram illustrating the experimental protocol. After preparation and time-matched equilibration, all animals received 45 min coronary artery occlusion (CAO) and 180 min reperfusion. Group CON received no further treatment prior to CAO. Ischemic preconditioning (IPC 3×5) was induced by 3 cycles of 5 min ischemia/reperfusion. Anesthetic-induced preconditioning was performed with 15 min administration of 1.0 MAC isoflurane (APC ISO), sevoflurane (APC SEVO) and desflurane (APC DES), respectively. To induce ischemic postconditioning (IPOST), three cycles of 30 sec reperfusion/ischemia were applied at the beginning of reperfusion. Anesthetic-induced postconditioning was performed with 18 min application of 1.0 MAC isoflurane (APOST ISO), sevoflurane (APOST SEVO) and desflurane (APOST DES), respectively, starting 3 min prior to the end of CAO. In two additional groups, ischemic preconditioning was induced with 6 cycles ischemia/reperfusion (IPC 6×5), and isoflurane was administered for 30 min to perform anesthetic-induced preconditioning (APC ISO 30′). Triangles indicate time points of analysis of hemodynamic data as presented in Table 1. A color version of this figure is available in the online journal.
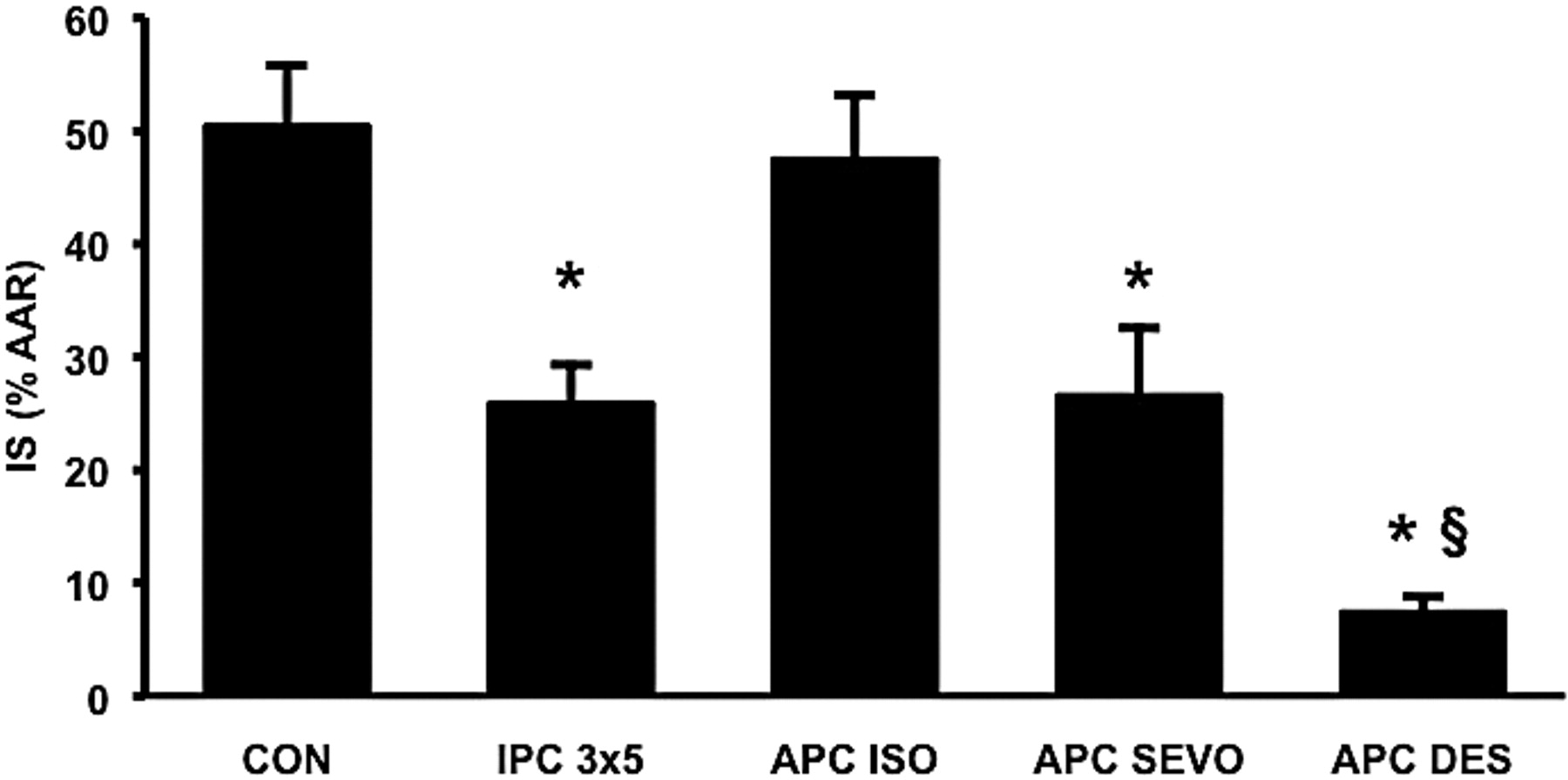
Influence of ischemic and anesthetic-induced preconditioning on myocardial infarct size. Mice received ischemic preconditioning (3 ×5 min ischemia/reperfusion, IPC 3×5, n =7) or anesthetic preconditioning (APC) with 1.0 MAC isoflurane (APC ISO, n = 7), sevoflurane (APC SEVO, n = 8) and desflurane (APC DES, n = 8). Volatile anesthetics were administered for 15 min. Infarct size (IS) is expressed as a percentage of the left ventricular area at risk (AAR). Data are mean ± SEM. * Significantly (P < 0.05) different vs. CON. §Significantly (P < 0.05) different vs. IPC 3×5 and APC SEVO.
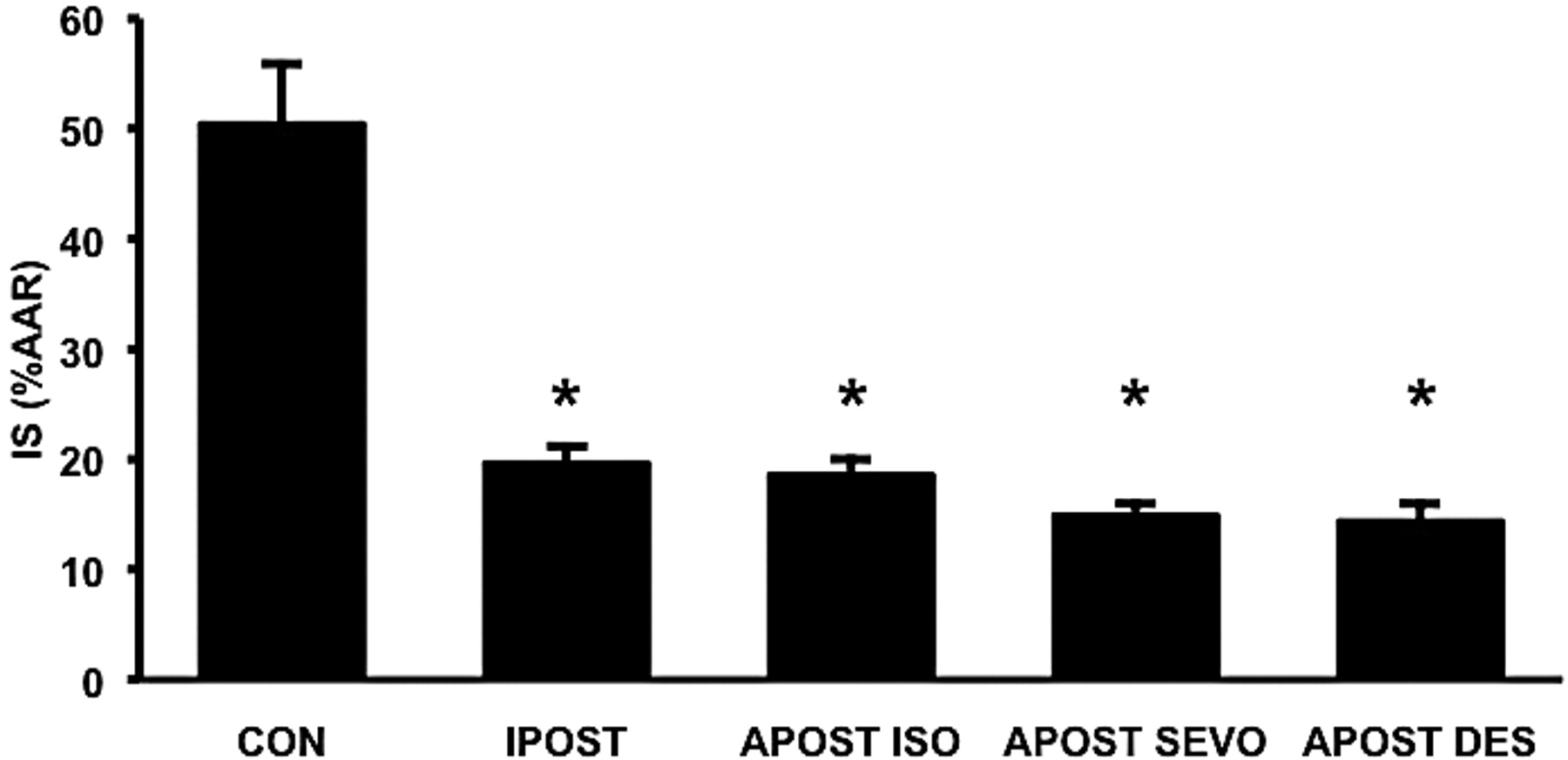
Influence of ischemic and anesthetic-induced postconditioning on myocardial infarct size. Mice received ischemic postconditioning (3 × 30 sec reperfusion/ischemia, IPOST, n = 7) or anesthetic postconditioning (APOST) with 1.0 MAC isoflurane (APOST ISO, n = 8), sevoflurane (APOST SEVO, n = 8) and desflurane (APOST DES, n = 8). Volatile anesthetics were administered for 18 min. Infarct size (IS) is expressed as a percentage of the left ventricular area at risk (AAR). Data are mean ± SEM. Note that CON data are the same as in Figure 2. * Significantly (P < 0.05) different vs. CON.
Footnotes
This work was supported in part by grant 01 KS9603 from the Ministry for Education and Research of the Federal Republic of Germany and the Interdisciplinary Centre for Clinical Research (IZKF) of Würzburg, Germany.
Acknowledgements
The authors thank Mrs. Katerina Pech BS for excellent technical assistance.