
Abstract
Background:
Microcatheter directed blood reperfusion is an endovascular salvage option for acute cerebral artery occlusions. It has not been investigated whether this technique may be associated with hemolysis.
Objective:
Analysis of hemolysis during blood infusion through different microcatheters and infusion rates to assess related risks.
Methods:
Four microcatheters with different inner diameters were perfused with blood samples at three infusion rates. Hemolytic markers including lactate-dehydrogenase (LDH) and haptoglobin were analyzed. Samples before and after blood infusion were compared using Student’s t-test. Flow-related degree of hemolysis was analyzed with regression analysis. Resulting shear stress was calculated and correlated with LDH and haptoglobin.
Results:
Significant increase of LDH and decrease of haptoglobin was found after blood reperfusion through small microcatheters at progressive flow rates (
Conclusions:
Progressive hemolysis occurs during blood perfusion of small lumen microcatheters at increasing flow rates. This phenomenon may be related to turbulent flow, exposure time and increased shear stress. Larger microcatheters did not induce hemolysis and may be the preferred choice for stroke reperfusion.
Introduction
Acute cerebral artery occlusions may be associated with immediate life threatening conditions [1]. Particularly reperfusion of acute stroke is time critical to prevent irreversible damage [2]. Various medical and endovascular options including vacuum assisted thrombectomy and stent retrievers are available to achieve arterial revascularization. Recent clinical trials have demonstrated excellent results for endovascular stroke management [3–9]. With endovascular techniques, initial recanalization across an acute cerebral artery obstruction may be achieved rapidly, whereas removal of the underlying obstruction takes 30–45 min [7,9,10]. In order to ‘buy time’ for preservation of viable brain tissue – particularly in challenging situations – where initial vacuum- or stent retriever assisted revascularization fails, reperfusion with oxygenated blood beyond arterial occlusions was suggested as an adjunct neuroprotective strategy. Once rapid tissue reperfusion has been achieved with temporary blood reperfusion, definitive endovascular reconstruction to resolve the underlying arterial occlusion may be commenced on a less time-critical basis [2,10,11].
Limited clinical case series have stated that microcatheter directed blood reperfusion of acute arterial occlusions is safe [2,10,11]. However, it has never been investigated whether this technique may be associated with mechanical blood trauma and hemolysis. Even low level hemolysis is associated with release of free hemoglobin and related antioxidant action [12]. Additional general blood cell damage such as platelet activation and white blood cell dysfunction may result. Scavenging of nitric oxide [13], damage to the glycocalyx and endothelial cells, and impairment of the vascular smooth muscle tone may result from hemolysis [14]. If hemolysis occurred in acute stroke management, further ischemia or hemorrhage might develop within the ischemic tissue. Consequently this study was performed to investigate whether hemolysis occurs after blood reperfusion with different microcatheters and infusion rates in an in-vitro model.
Methods
This in-vitro study was approved by the institutional review board (HREC–H0014127). Experiments were conducted on four different microcatheters at infusion rates of 1-, 2- and 3 ml/s.
For each of the 4 microcatheters 90 ml venous blood were drawn from a single test person to reduce variability. 90 IU Heparin, dissolved in 0.9 ml of 0.9% saline solution were added to the blood and mixed gently. 20 ml of blood were directly transferred into Vacutainer test tubes to obtain two baseline biochemical and hematological measurements.
The remaining 70 ml of heparinized blood was transferred into the 150 ml syringe of an angiographic power injector (Avidia, Imaxeon, Rydalmere, Sydney NSW 2116, Australia) at 37°C. The power injector was connected to the hub of the microcatheters without connection tubing to reduce dead space. All microcatheters had straight-tip configurations and were 150 cm long with one exception (Penumbra 5MAX, 132 cm length). Inner luminal diameters were different for all microcatheters (Table 1).
Specification of microcatheter details investigated for blood reperfusion
Specification of microcatheter details investigated for blood reperfusion
Notes: Except for the Renegade HI-FLO microcatheter, injection pressure limits were not provided by the manufacturers.
Air was completely purged from the injector syringe and microcatheters were completely filled with blood from the syringe prior to infusion. 10 ml aliquots were injected through each microcatheter at flow rates of 1-, 2- and 3 ml/s. Experiments were repeated twice for each infusion rate and microcatheter according to sample size analysis. To prevent pressure related microcatheter disruption, injection pressure was limited to 5171 kPa on the power injector with an initial continuous rise of 0.3 s for all microcatheters and infusion rates. Injected samples were collected in 10 ml syringes and subsequently divided into Vacutainers for immediate biochemical analysis. Injection duration and volumes were recorded. The following biochemical parameters were analyzed:
Means and standard deviations were calculated for baseline and post-perfusion measurement parameters for all microcatheters and flow rates. A paired Student’s t-test was performed for significance between baseline-values and corresponding samples after blood infusion for each microcatheter and infusion rate. Significant difference was accepted when
Whole human blood was considered a non-Newtonian power-law fluid with a density of 1050 kg/m3 [14]. Consequently the viscosity of blood is a decreasing function of shear rate [15] and obeys power law characteristics:
K and n were determined by non-linear regression of experimental data published by Castellini et al. [15], as 3.23E−03 and 0.567, respectively.
A modified Reynold’s number as derived by Metzner and Reed for time-independent non-Newtonian fluids was used to determine flow regime [16]:
Shear rate at the catheter wall (laminar region) was calculated using the Rabinowitsch–Mooney relationship [16]:
For turbulent flow of non-Newtonian fluids obeying power law characteristics (as is the case with blood), the Dodge and Metzner chart was used to determine the friction factor in the equation provided by Wilson and Thomas [16]:
ϵ is a measure of surface roughness, and for smooth tubes the ratio of
Linear regression analysis was performed between mean shear stress, LDH- and haptoglobin measurements. Correlation coefficients (r) were estimated. Sample size calculation for two-sided analysis was
Except for lactate-dehydrogenase and haptoglobin, coagulation, electrolyte and hematologic parameters were unchanged before and after blood reperfusion at all infusion rates for the 4 microcatheters (
Summary of means for baseline and post-microcatheter infusion measurements including standard deviation for electrolytes, hematology and coagulation parameters
Summary of means for baseline and post-microcatheter infusion measurements including standard deviation for electrolytes, hematology and coagulation parameters
Notes: None of the evaluated microcatheters and flow rates have demonstrated significant differences among baseline and test samples (
Mean baseline LDH concentration from all experiments was 163 ± 23 U/l. Significant increase of LDH was found after perfusion of the Excelsior SL-10 and Vasco+21 microcatheters at all three infusion rates (
Means and standard deviations of LDH- and haptoglobin concentrations before and after blood perfusion through the four microcatheters at flow rates of 1-, 2- and 3 ml/s
Means and standard deviations of LDH- and haptoglobin concentrations before and after blood perfusion through the four microcatheters at flow rates of 1-, 2- and 3 ml/s
Notes: These differences were significant (
Linear regression analysis showed progressive increase of LDH with higher flow rates for the Excelsior SL-10 and Vasco+21 microcatheters. Correlation between flow rates and LDH levels was
Mean baseline haptoglobin concentration was 1.80 ± 0.07 g/l. Significant reduction of haptoglobin was found after blood infusion through the Excelsior SL-10 and Vasco+21 microcatheters at all three infusion rates (
LDH/haptoglobin relationship
Regression analysis between LDH and haptoglobin for all samples before and after blood perfusion and for all catheters and infusion rates demonstrated a negative relationship (
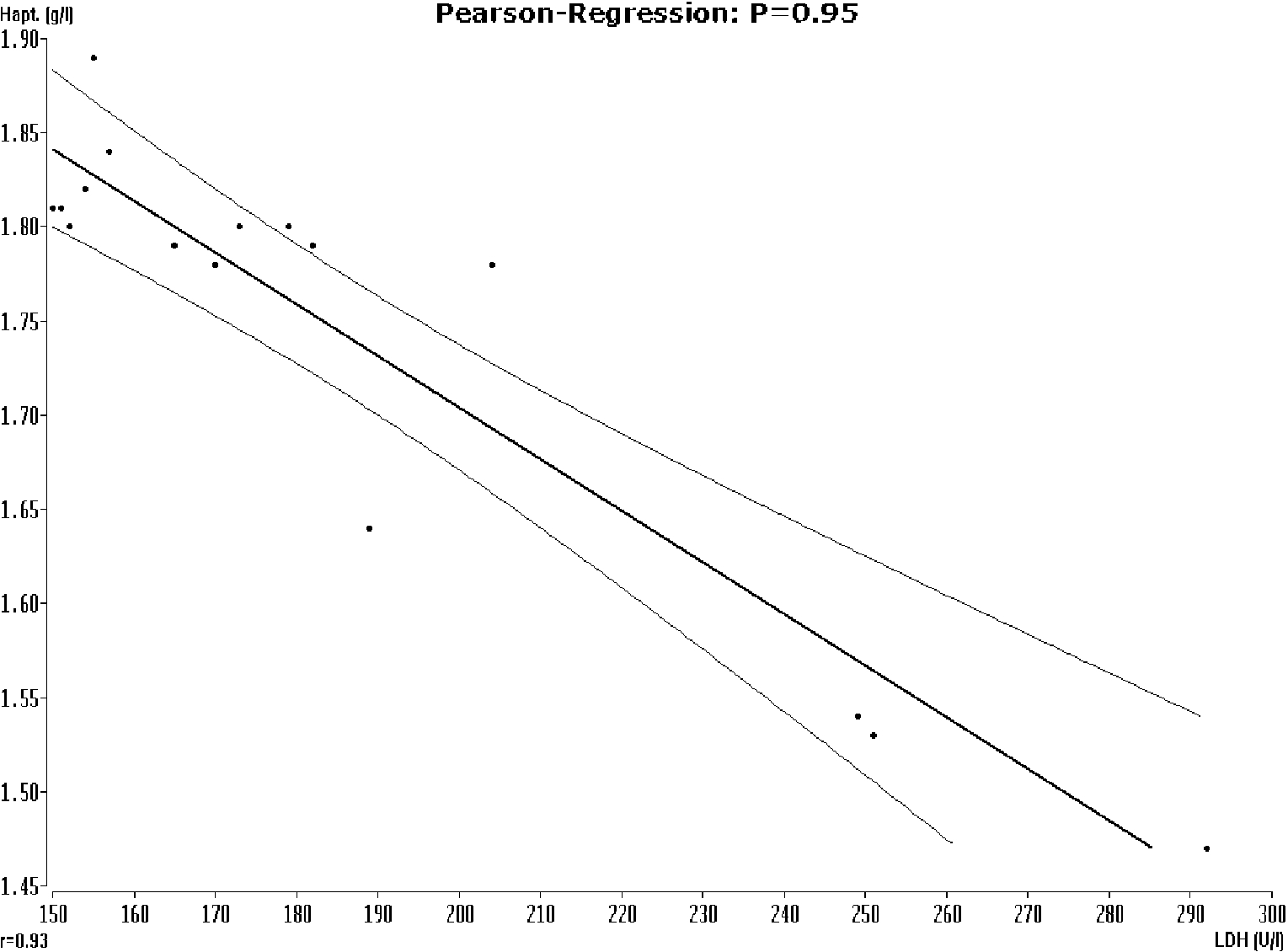
Linear regression between mean haptoglobin and LDH levels for all samples before and after blood perfusion of all microcatheters and infusion rates, demonstrating a negative relationship between LDH and haptoglobin (
At the selected uniform pressure limit of 5171 kPa, the full selected blood volume of 10 ml was delivered in expected time for the Vasco+21, Renegade HI-FLO and Penumbra 5MAX microcatheters at flow rates of 1 ml/s (10 s infusion time), 2 ml/s (5 s infusion time) and 3 ml/s (3.3 s infusion time).
The preset pressure limit was exceeded with the Excelsior SL-10 microcatheter during blood infusion at rates of 2- and 3 ml/s. The power injector aborted blood infusion when 6 ml of blood had been infused at a rate of 2 ml/s, and when 4 ml were infused at a flow rate of 3 ml/s. Subsequently infusion was repeated immediately to obtain sufficient sample volumes for biochemical analysis. The Excelsior SL-10 microcatheter reliably delivered 10 ml of blood within 10 s at an infusion rate of 1 ml/s without reaching the pressure limit of 5171 kPa. No microcatheter or hub connector rupture occurred during the experiments.
Flow velocities, modified Reynold’s numbers and shear stress
Flow velocities in microcatheters ranged between 0.6 and 21.6 m/s and modified Reynold’s numbers between 7753 and 718,917, which means that for all experiments, the flow regime was turbulent [17]. Resulting shear stress ranged from 0.9 to 657 Pa. Resulting velocities, modified Reynold’s numbers and shear stress for each microcatheter/flow rate combination are summarized in Table 4. Positive correlation was found between LDH levels and shear stress (
Infusion rate related blood flow velocities, modified Reynold’s numbers and shear stress within the 4 microcatheters
Infusion rate related blood flow velocities, modified Reynold’s numbers and shear stress within the 4 microcatheters
indicates that the predefined pressure limit was exceeded.
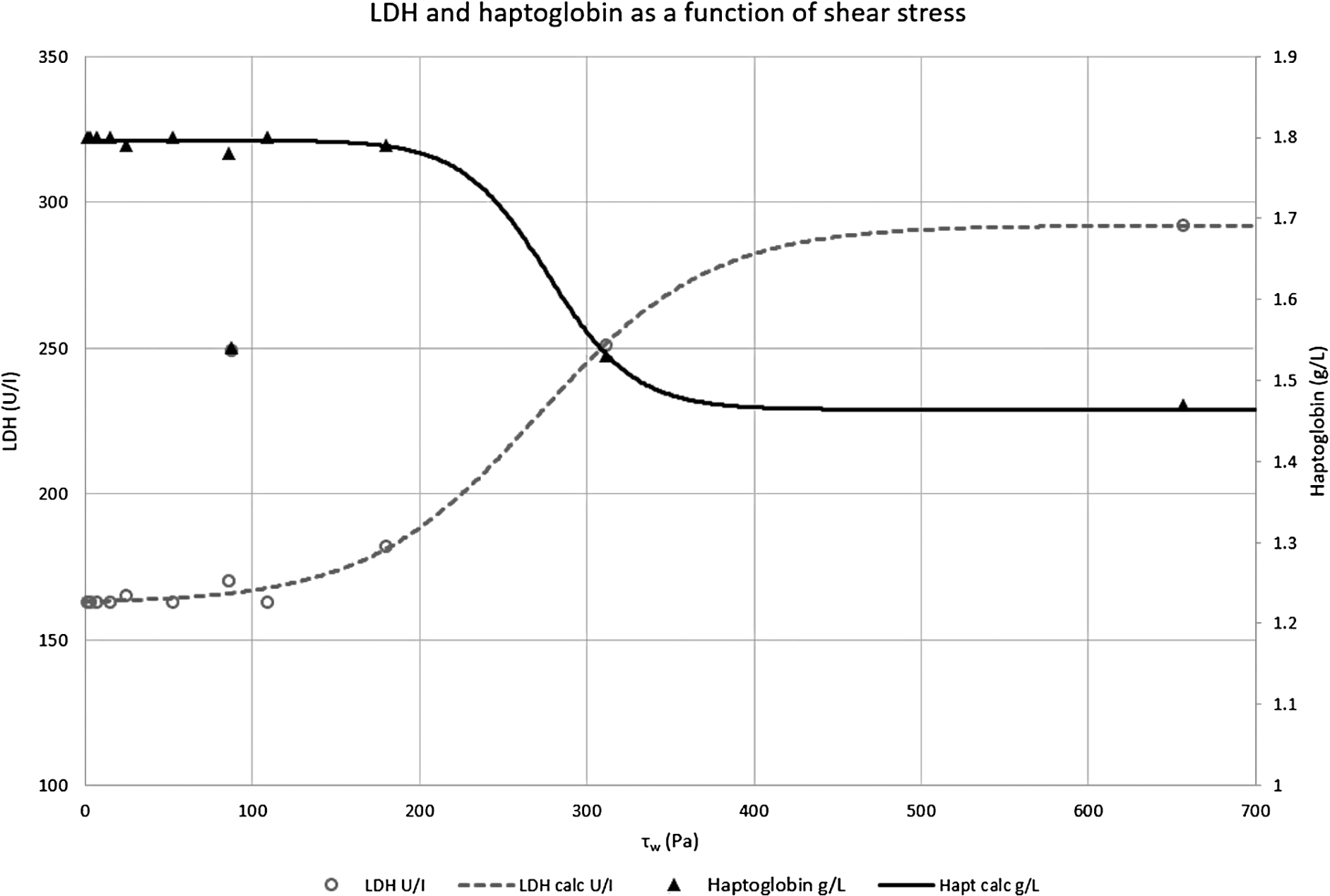
Stacked line graph with markers for LDH (U/l) and haptoglobin (g/l) concentrations in relation to shear stress. Below 100 Pa, no significant change in LDH levels or haptoglobin concentration is evident. Above 100 Pa however, the changing concentrations indicate progressive hemolysis of blood cells, until degradation is complete. Correlation between shear stress, LDH and haptoglobin was
The only effective treatment for arterial occlusions, particularly in acute stroke is rapid recanalization of the occluded vessel by restoring physiological blood flow [1,3]. Time to recanalization is critical to prevent irreversible deficits [2,10,11]. Previous studies have demonstrated that recanalization frequently occurs too late, resulting in infarcts with lifelong disability or death [18]. In stroke settings it has recently been demonstrated that endovascular transarterial procedures are associated with high rates of arterial recanalization and superior to conservative management approaches [4–9]. However, definitive recanalization with mechanical thrombectomy can be challenging in certain clinical situations, resulting in delayed reperfusion of penumbral tissue [2].
To reduce the critical reperfusion time in challenging situations, an adjunct blood reperfusion technique has been proposed [2,10,11]. Heparinised arterial blood from an aortic or iliac artery sheath is reinfused through a microcatheter positioned with its tip distal to the arterial occlusion. Once blood supply to the ischemic territory has been temporarily reconstituted, the underlying thromboembolic occlusion may subsequently be treated by means of thrombolysis, angioplasty or mechanical thrombectomy. Such a microcatheter reperfusion technique may consequently be used when initial vacuum-, respectively, stent retriever assisted thrombectomy fails in order to ‘buy more time’ for definite and sustainable treatment of the underlying condition. Previous publications have suggested that such microcatheter directed perfusion of ischemic brain territories with oxygenated blood through arterial occlusions is clinically feasible and safe [2,10,11]. However, this technique may be associated with significant blood trauma and hemolysis, which may result in hemorrhage or progressive ischemia within the affected brain tissue. Such effects have not been investigated previously.
Markers of hemolysis
Changes in LDH and serum haptoglobin levels are considered the most sensitive general tests to determine mechanical hemolysis [19]. Consequently this study was focused on investigation of these two basic biochemical markers. The correlation found between LDH and haptoglobin (
Effects of mechanical hemolysis
It has previously been revealed that blood trauma may result from non-physiological flow conditions such as elevated shear forces, turbulence, cavitation, prolonged contact and collision between blood cells and foreign surfaces [14]. These factors are associated with a variety of damage mechanisms: overstretching or fragmentation of erythrocytes causing release of free hemoglobin, activation or dysfunction of platelets and leukocytes, increased concentrations of inflammatory mediators and complement activation. Even low levels of hemolysis have been shown to increase RBC aggregation at low shear conditions [20]. Consequently even low level hemolysis is considered an important warning sign of other potential blood cell damage such as platelet activation, white blood cell dysfunction and other serious complications such as scavenging of nitric oxide, damage to glycocalyx and endothelial cells, and impairment of the vascular smooth muscle tone [14]. In consequence, hemolysis associated with microcatheter directed blood reperfusion may promote platelet aggregation, hypercoagulation and intravascular thrombosis [14]. Beside complete cellular destruction, damage can also be induced to the RBC membrane on a sublethal level, resulting in decreased deformability and increased aggregability, again resulting in an increased risk of intravascular thrombosis. This phenomenon however may be reversible to a certain extent depending on duration and intensity of damage [21]. A decrease in cell deformability results in a reduced capacity for RBC’s to enter small capillaries and a reduced contact of the cell surface with the surrounding vessel wall, compromising microcirculation and oxygen delivery to surrounding tissue [22].
When RBC membranes have been overstretched or fragmented by non-physiological blood flow conditions, plasma free hemoglobin (PfHb) and heme enter the circulation. PfHb is cleared by the Hb scavengers, haptoglobin and CD163. Additionally LDH is released when red blood cells are destroyed [23]. The resulting products from hemolysis together with interleukin-10 release, induced by the Hb clearing mechanism exert an antioxidant, anticoagulant, and vasodilating effect, thus compensating for the adverse effects caused by PfHb and heme [19]. However, on saturation of free Hb scavengers, PfHb binds nitric oxide (NO) derived from the vascular endothelium in a fast and irreversible way [24]. NO depletion then results in elevated vascular resistance, increased thrombin formation, fibrin deposition, platelet activation and -aggregation [25]. In summary PfHb causes endothelial dysfunction and vasomotor instability by reducing nitric oxide bioavailability [13].
Shear stress and modified Reynold’s number associated with blood reperfusion
The mechanisms of mechanical cell damage during catheter reperfusion have been described by different investigators [26,27], identifying positive and negative pressure, wall impact forces, blood non-endothelial surfaces, time of exposure and blood–air interference as responsible parameters for blood trauma. RBC’s seem to have a high tolerance to most of these forces, except for shear stress [28]. Physiologic intravascular shear stress ranges from 0.1–5 Pa, sublethal damage is reported to appear from 21–43 Pa, lethal damage to RBC occurs from 150 Pa, and above. The thresholds for platelet and leucocyte activation are, respectively, ∼10 and 7.5 Pa [29]. Beside shear stress, duration of exposure is another factor related to cellular damage [29]. One hour of exposure to wall shear stress exceeding ∼40 Pa was found to damage endothelial cells leading to their destruction [14].
It has been described that exposure time related to laminar shear stress may result in almost five orders of magnitude for hemolysis and shear stresses up to 500 Pa, where exposure times varied between 60 and 300 s [27]. In the present study however, exposure times varied only between 3.3 and 10 s, consequently limiting the effect of exposure time on results.
Table 4 shows the values for velocity, modified Reynold’s numbers, and shear stress, for all combinations of catheters and flow rates evaluated. According to these calculations, shear stress within the Excelsior SL-10 microcatheter ranged between 87 and 657 Pa. These forces would subsequently be considered within or close to the lethal range for RBC damage [29], reflected by significant hemolysis in all analyzed re-perfused blood samples with this microcatheter. The Vasco+21 microcatheter demonstrated a lower shear stress range between 24–180 Pa. These forces are within the reported range of sublethal–lethal RBC damage [29] and again significant hemolysis was found after blood reperfusion at all infusion rates. With the Renegade HI-FLO microcatheter shear stress was further reduced and ranged between 15–109 Pa. Despite exceeding the reported sublethal shear stress-level of RBC damage [29], no associated hemolysis was found in all corresponding samples after blood reperfusion. Shear stress within the Penumbra 5 MAX catheter remained below the sublethal level [29] at all infusion rates (0.9–6.6 Pa) and consequently no hemolysis was found.
Turbulent flow is associated with significantly increased hemolysis when compared with laminar flow at the same wall shear stress level [17]. Furthermore, in turbulent flow there are additional effects due to the interaction of the smallest sized eddies (Kolmogorov-sized eddies) with the red blood cells. Assuming dissipation of eddies occurs instead via cell–cell interactions mediated by the plasma, turbulent velocity fluctuations, normally ascribed to turbulent (Reynold’s) stresses, give rise to viscous shear stresses [30]. These effects were not investigated with our experimental design.
Study limitations
This in-vitro study is associated with certain limitations. In a clinical setting thromboembolic occlusions usually occur at branch bifurcations. Microcatheter directed whole blood reperfusion, however, is generally targeting a single branch only. Consequently other occluded branches may not benefit from reperfusion. In this experiment venous blood has been used to study effects on hemolytic markers. We have not investigated whether arterial blood samples may be affected from a loss of oxygen saturation, even though this appears unlikely. In this experiment the microcatheters were directly connected to the power injector without connecting tubing. In a clinical setting this approach would be impractical and the additional tubing length may impact the extent of hemolysis. The current assessment of haemolysis is incompletely defined by shear stress considerations alone. Additional factors, such as cell-wall interactions, roughness of the microcatheter luminal wall, surface charge, time of exposure, etc. may be relevant for hemolysis but were not assessed in this investigation. When using microcatheter assisted blood reperfusion in vivo, an increased postobstructive endovascular pressure related to high flow rates may potentially cause proximal dislodgement of thrombus with transfer of embolic material into different arterial branches. However, since cerebral autoregulation in ischemic stroke is associated with vasodilation, distal vascular resistance and pressure would be decreased [31]. This lack of vascular resistance and the persistent trans-occlusive pressure gradient should contribute to a decreased risk of proximal clot migration during whole blood reperfusion. Even though results of this study have not demonstrated coagulation disorders in vitro, the use of heparinized blood may be associated with an increased risk of hemorrhage, particularly in stroke cores where the blood brain barrier may have already been irreversibly damaged. Apart from such considerations, blood reperfusion may help to locally clear vaso- or neurotoxic substances that have accumulated within the ischemic territory and which may otherwise promote hemorrhagic complications [2]. Current revascularization techniques with stent retrievers frequently generate instant reperfusion channels [4,6–9] and the ADAPT technique seems to provide the fastest stroke recanalization time [5]. In consequence microcatheter directed blood reperfusion should be reserved for complex or challenging cases, where initial revascularization with stent retrievers of vacuum assisted clot extraction fails, in order not to delay definitive and efficiently proven treatment options.
Conclusions
Microcatheters with inner luminal diameters of less than 0.69 mm seem to induce excessive hemolysis during whole blood reperfusion. Apart from other factors, such as exposure time, the combination of microcatheter diameter and perfusion rate seems to determine the resulting shear stress, and associated hemolysis under turbulent flow conditions. This study indicates that significant hemolysis may occur at shear stress values greater than 100 Pa, which is in agreement with previous findings [28]. Microcatheters with diameters of 0.69 mm or more did not induce significant hemolysis at flow rates up to 3 ml/s. Depending on required flow rates, larger lumen microcatheters consequently may be the preferred choice for autologous blood reperfusion in acute stroke settings.