
Abstract
BACKGROUND:
Local vibration has shown promise in improving skin blood flow and wound healing. However, the underlying mechanism of local vibration as a preconditioning intervention to alter plantar skin blood flow after walking is unclear.
OBJECTIVE:
The objective was to use wavelet analysis of skin blood flow oscillations to investigate the effect of preconditioning local vibration on plantar tissues after walking.
METHODS:
A double-blind, repeated measures design was tested in 10 healthy participants. The protocol included 10-min baseline, 10-min local vibrations (100 Hz or sham), 10-min walking, and 10-min recovery periods. Skin blood flow was measured over the first metatarsal head of the right foot during the baseline and recovery periods. Wavelet amplitudes after walking were expressed as the ratio of the wavelet amplitude before walking.
RESULTS:
The results showed the significant difference in the metabolic (vibration 10.06 ± 1.97, sham 5.78 ± 1.53, p < 0.01) and neurogenic (vibration 7.45 ± 1.54, sham 4.78 ± 1.22, p < 0.01) controls. There were no significant differences in the myogenic, respiratory and cardiac controls between the preconditioning local vibration and sham conditions.
CONCLUSIONS:
Our results showed that preconditioning local vibration altered the normalization rates of plantar skin blood flow after walking by stimulating the metabolic and neurogenic controls.
Introduction
Vibration therapy has been increasingly popular in sports training and rehabilitation over the last decade. These mechanical vibration stimuli have shown positive benefits, such as improved proprioception, postural balance, muscle strength, muscle oxygenation and skin blood flow [1,2]. Vibration therapy can be classified as the whole body vibration (WBV) and local vibration (LV). WBV requires the participant to stand on a vibrating platform, and LV refers to that the vibration is directly applied over a specific muscle [3]. WBV is more popular compared to LV, and has been widely investigated. The benefits of LV have not been widely studied [4,5].
LV has been showing promise in wound healing [1,6–8]. However, the potential mechanism of vibration therapy in wound healing has not been adequately discussed in the literature. Reflexive muscle contractions are often considered as one of the potential mechanisms for vibration-induced increases in muscle perfusion [9]. Another potential mechanism of vibration therapy is related to neurophysiological receptors and factors, including MCP-1, VEGF, and IGF-1 [10]. Some studies supported that the increase in blood flow after vibration may be induced by nitric oxide (NO) production caused by increased blood flow shear stress [11,12].
Skin blood flow (SBF) responses reflect the ability of the skin vasculature in response to mechanical stress [13]. An important role of skin microcirculation is to regulate blood flow to meet the metabolic demands of local cells [14]. Previous studies have demonstrated that assessing dynamics of skin blood flow can be a reliable method to study microvascular reactivity in various pathological conditions and corresponding control mechanisms in response to various stimuli (vibration in this study) [14,15]. The underlying physiologic mechanism of impaired microvascular reactivity can be assessed by using wavelet analysis of blood flow oscillations (BFO) [16,17]. A number of researchers used wavelet transforms and demonstrated that five characteristic frequencies are associated with metabolic endothelial (0.0095–0.02 Hz), neurogenic (0.02–0.05 Hz), myogenic (0.05–0.15 Hz), respiratory (0.15–0.4 Hz) and cardiac (0.4–2.0 Hz) activities [14,15,17–19]. The designation of each frequency of BFO to a specific physiologic control is based on a series studies conducted in the past two decades [16,17]. The respiratory (0.15–0.4 Hz) and cardiac (0.4–2.0 Hz) activities reflected on skin BFO are associated with heart beat and respiratory movements, respectively. The myogenic activity of BFO (0.05–0.15 Hz) reflects the activity of vascular smooth muscles of blood vessels (ie. vasomotion). The neurogenic activity of BFO (0.02–0.05 Hz) refers to the regulation of SBF from the sympathovagal system. The metabolic activity (0.0095–0.02 Hz) refers to the endothelial nitric oxide dependent control [14–19].
Previous studies from our group have explored using this new quantification method to investigate the regulatory mechanisms of skin blood flow in response to mechanical and thermal stresses [13–15]. For example, we used the wavelet-based spectrum analysis to assess the contribution of each blood flow control mechanism in response to local heating among older people and demonstrated that the increase of blood flow is mediated by metabolic control related to endothelial nitric oxide [14]. We also applied the wavelet analysis of blood flow oscillations to investigate the effects of thermal stress (local cooling and heating) on skin blood flow response to prolonged pressure and identified that the associated metabolic and myogenic activities of the skin mediated these responses [13]. Furthermore, in order to better understand the pathogenesis of diabetic foot ulcers, Jan et al. used the wavelet analysis of BFO to evaluate skin blood flow at the first metatarsal head in response to mechanical (300 mmHg pressure) and thermal stresses (local heating to 42 °C) and found that diabetes causes impairments of metabolic, neurogenic, and myogenic controls that contribute to microvascular dysfunction [15]. Theoretically, the wavelet analysis of skin blood flow oscillations could help to better understand the beneficial mechanism of vibration therapy [2].
Walking (the most common form of weight-bearing activity) results in a higher plantar stress to the plantar foot, which increases risk of foot ulcers [20]. Such increased plantar stress may cause foot ulcers, especially in people with diabetic neuropathy who have microvascular dysfunction and impaired sensation to plantar stress [21]. Thus, there is a need to minimize the effect of walking-induced ischemia on plantar tissue after walking in people at risk for foot ulcers. Preconditioning of plantar tissue could be a method to reduce ischemic damage caused by repetitive plantar stresses [22], which may reduce risk of foot ulcers. In our study, we evaluated the effects of preconditioning local vibrations on weight-bearing plantar tissue after walking using wavelet analysis of BFO [23]. Although our previous studies [23,24] demonstrated local vibration as a preconditioning intervention to alter plantar SBF after walking, the exact mechanisms mediating the blood flow response after local vibration remain unknown.
To the best of our knowledge, there are no studies using wavelet analysis of SBF to characterize skin blood flow control mechanisms in response to preconditioning vibrations to subsequent walking. Thus, there is a need to access how preconditioning vibration therapy alter plantar skin blood flow response to ischemic stresses caused by walking. The aim of this study was to use wavelet analysis of BFO to study skin blood flow control mechanisms in response to preconditioning vibrations on the plantar foot after walking. We hypothesized that metabolic endothelial control (ie. 0.0095–0.02 Hz of BFO) of the plantar foot is the responsible control mechanism in response to preconditioning local vibration to subsequent walking.
Methods
A double-blind, repeated measures design was used in this study. The participants and the person performed the analysis were blinded to the 100 Hz vibration and sham vibration conditions [23].
In order to examine the safety of the preconditioning local vibration protocol to the plantar tissue, people who were not at risk for foot ulcers were recruited for this study first. After establishing the feasibility and safety of using preconditioning local vibration to alter plantar skin blood flow to walking, this protocol would be used in people at risk for foot ulcers (e.g. diabetic patients with peripheral neuropathy and arterial diseases). The inclusion criteria were healthy young adults aged between 18 and 35 years. The exclusion criteria were cardiovascular diseases, diabetes mellitus, skin diseases, and any neurological diseases. Subjects who took vasoactive medicine, nitric oxide donors, beta or alpha-blockers, calcium channel blockers or antagonists were also excluded. All participants had detailed procedures introduced to them before participating in the experiment and signed the informed consent document. This study was approved by the University of Illinois at Urbana-Champaign, Institutional Review Board (#20322).
The laser Doppler flowmetry (LDF) (PeriFlux 5000, Perimed, Las Vegas, NV) was used to noninvasively measure SBF at the first metatarsal head. The first metatarsal head is a common site of foot ulcers due to the center of pressure trajectories during walking [21]. The LDF device delivered a low-power (1–2 mW) near infrared laser (780 nm wavelength) from a solid-state diode laser source. The sampling rate of LDF signals was 32 Hz. Before each experiment, the LDF was calibrated and warmed up for 30 minutes to ensure a reliable data collection. The local vibration was delivered by a custom assembled vibrator consisting of a voice coil motor, a controller, and a power supply [2]. The voice coil motor (YLM40-20, JDStek, CA, USA) was chosen because of its structural stability with high positioning resolutions and fast acceleration/deceleration and high speed capacity. The position sensor and controller (MS 15 TTLx20, RSF Elektronik, Tarsdorf, Austria) was used to control the voice coil motor with the resolution at 0.5 μm (1 mm for 2000 counts). The power supply was used to provide DC voltage between 24 and 48 V. The radius of vibrator head was 1 cm. In this study, the vibrator was used to apply vibrations at 0 Hz (sham control) and 100 Hz with the peak acceleration of 2g and the amplitude of 1 mm.
The room temperature was maintained at 24 ± 2 °C during the experiment. Subjects were ask to relax in the supine position for at least 30 minutes to stabilize the baseline blood flow level and acclimate to the room temperature. Then, plantar skin blood flow was measured for 10 minutes. The subject randomly received one of two vibration protocols (ie. 100 Hz vibration and sham vibration) for 10 minutes. The sham vibration protocol was blinded to the subject and was instructed as the one of two vibration frequencies to the subject. Then, the subject walked on a treadmill at a speed of 6 km/h for 10 minutes. During vibration and walking, plantar skin blood flow was not measured due to movement artifacts. After walking, the subject returned to lie on the mat table for another 10 minutes of skin blood flow measurement. The washout period was 30 minutes to minimize the carryover effect. Then, the subject repeated the procedures with the other vibration protocol.
In order to understand the mechanisms responsible for the difference of SBF in response to preconditioning local vibrations, we performed the wavelet analysis of SBF oscillations [14–19,25,26]. Its procedures are described briefly as follows. For a SBF signal x(u), the continuous wavelet transform is defined as
Physiological meanings of skin blood flow controls reflected in various characteristic frequencies
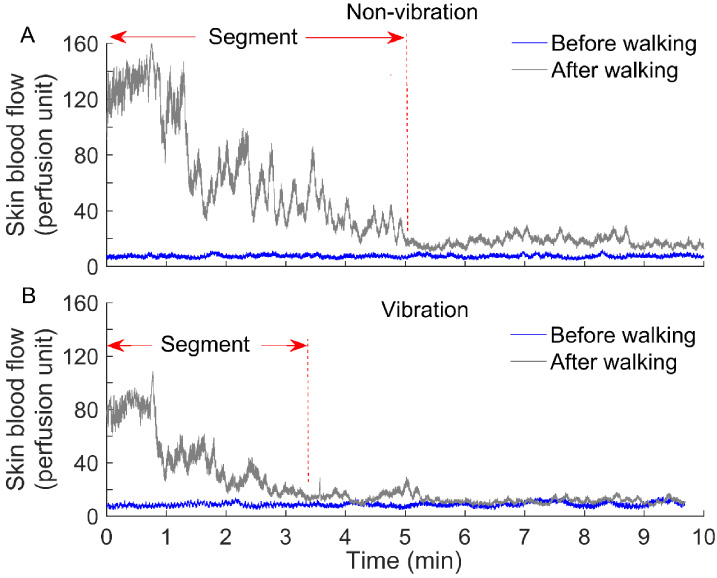
(A) The figure shows an example of skin blood flow before and after walking when no local vibrations were applied before walking. (B) The figure shows an example of skin blood flow before and after walking when local vibrations were applied before walking.
Ten healthy participants (10 females) were recruited in this study. The demographic data were (mean ± standard deviation): age, 25.0 ± 6.2 years; height, 163.7 ± 2.8 cm; weight, 60.3 ± 5.7 kg; and body mass index, 22.5 ± 2.2 kg/m2.
Figure 1 shows typical examples of plantar skin blood flow responses before and after walking under the preconditioning local vibration and non-vibration (sham vibration) protocols. Figure 2 shows the wavelet amplitudes of skin blood flow shown in the Fig. 1. The wavelet spectrum reveals characteristic frequencies embedded in skin blood flow oscillations.
Figure 3 shows the comparisons of the mean ratio of wavelet amplitude of the metabolic (0.0095–0.02 Hz of BFO), neurogenic (0.02–0.05 Hz of BFO), myogenic (0.05–0.15 Hz of BFO), respiratory (0.15–0.4 Hz of BFO) and cardiac (0.4–2.0 Hz of BFO) controls between the preconditioning local vibration and non-vibration conditions. The results show the significant difference in the metabolic (local vibration 10.06 ± 1.97, non-vibration 5.78 ± 1.53, p < 0.01) and neurogenic (local vibration 7.45 ± 1.54, non-vibration 4.78 ± 1.22, p < 0.01) controls. There are no significant differences in the myogenic, respiratory and cardiac controls between the preconditioning local vibration and non-vibration conditions (3).

(A) The wavelet spectrum of the skin blood flow signal shown in (A) reveals characteristic frequencies of skin blood flow oscillations. (B) The wavelet spectrum of the skin blood flow signal shown in (B) reveals characteristic frequencies of skin blood flow oscillations.

Comparisons of wavelet amplitudes of metabolic endothelial, neurogenic, myogenic, respiratory and cardiac controls of skin blood flow oscillations with (100 Hz, 2g, 1 mm amplitude vibration) and without (sham vibration) preconditioning vibrations. The results showed the significant difference in the metabolic (vibration 10.06 ± 1.97, sham 5.78 ± 1.53, p < 0.01) and neurogenic (vibration 7.45 ± 1.54, sham 4.78 ± 1.22, p < 0.01) controls.
This is the first study using wavelet analysis of SBF to characterize skin blood flow control mechanisms in response to preconditioning local vibrations to subsequent walking. Our results demonstrated that metabolic endothelial control (ie. 0.0095–0.02 Hz of BFO) and neurogenic control (ie. 0.02–0.05 Hz of BFO) mainly contributed to the decrease in SBF after walking when preconditioning local vibration was applied on the first metatarsal head before walking. The finding from this study supports our hypothesis that preconditioning local vibrations (100 Hz, 1 mm amplitude) on the first metatarsal head could alter plantar skin blood flow response after walking through stimulating the metabolic endothelial mechanism. This study also identified that the neurogenic control contributed to the SBF response to preconditioning local vibrations. Our finding could help provide insight how preconditioning local vibrations alter plantar skin blood flow responses after walking.
Comparisons of wavelet amplitudes of skin blood flow oscillations from our results show that the metabolic control plays an important role in preconditioning vibrations on altering plantar skin blood flow responses after walking. We compared SBF responses after walking in two conditions (with and without preconditioning local vibrations) and speculate that these preconditioning local vibrations might reduce plantar ischemia during walking [12,28]. The reason for this speculation is based on the principle of reactive hyperemia; when a smaller ischemic stress is applied in the same person, it causes a smaller reactive hyperemic response. In this study, a smaller reactive hyperemic response was observed in the preconditioning local vibration protocol that implies the ischemic stress caused during walking was perceived as a smaller ischemic stress by the preconditioned plantar tissue [29]. Vibration-induced shear force applied to the skin have been shown to stimulate capsaicin sensitive nerve fibers to release CGRP, VIP, and PACAP [30,31]. These factors stimulate endothelial cells to release nitric oxide (NO) [29]. NO, a powerful vasodilator, elicited a cutaneous vasodilatation [32], and then improve skin blood flow. Maloney-Hinds et al. investigated the relationship between SBF and NO production between healthy subjects and diabetic patients. Both groups showed an increase in SBF with 5 minutes of vibration at 50 Hz [12]. Johnson et al. evaluated the effect of whole body vibration on SBF and NO concentrations in diabetic patients and hypothesized that increases in SBF during WBV could be attributed to the action of NO on vascular tone [28]. Recently, a study from our group investigated SBF control mechanisms in response to different vibration frequencies and found that the SBF significantly increased after the high frequency vibration (100 Hz) compared to the low frequency (0 (sham) and 35 Hz) due to the metabolic regulation (0.0095–0.02 Hz of BFO). Our results also showed a decrease of neurogenic regulation in the preconditioning local vibration protocol. The neural activity caused by the local vibration is much unknown [2].
Our results showed a decrease in SBF after walking under the preconditioning local vibration protocol, which seems inconsistent with previous studies. However, our current study design was not the same with the previous studies. The results of peak SBF and recovery time measured in this study reflected the effects of preconditioning local vibrations on weight-bearing plantar tissue, not the immediate effect of blood regulation in response to local vibration. In the literature, including our previosu studies, local vibration can cause an immediate increase in SBF [2]. In this study, we demonstrated that using local vibrations to preconditioning plantar tissue before walking can significantly alter plantar skin blood flow responses after walking, that is, a smaller reactive hyperemic response. Based on the principle of reactive hyperemia, we demonstrated that such preconditioning local vibration might reduce the effect of ischemic stress caused during walking for eliciting a smaller reactive hyperemic response after walking. We speculate that preconditioning local vibration can cause an adaptation process of plantar tissue to walking induced ischemic stresses. Our results demonstrated that the metabolic endothelial control (IE. 0.0095–0.02 Hz of BFO) is responsible for such change in SBF [33]. As for the potential physiological mechanism of the vibration therapy, some researchers found that the oxygen consumption, heart rate, blood lactate, testosterone, and growth hormone concentration significantly increase after applying vibration intervention [34–37]. Furthermore, several studies have shown that the vibration-enhanced SBF resulted from an increase in endothelial-derived NO production [38–40]. Taken together, the evidence suggests that the local metabolic mechanism mediated by endothelial NO might be activated before walking, caused by the preconditioning local vibrations. To be more specific, the vibration-induced protection might improve the microcirculation before walking, thereby minimizing the tissue ischemia caused by subsequent walking. Thus, with preconditioning local vibrations, the peak SBF and total SBF were smaller after walking, which is consistent with the above assumption, that is, the reactive hyperemia was smaller.
Although preconditioning vibrations may change SBF responses after walking, there is still need to clarify if patients with DM could benefit from such preconditioning effects prior to walking exercise. In terms of the effects of walking on SBF, numbers of research studies accessed the effects of various intensities (speed and duration) of walking exercise on plantar SBF and tried to explain that how plantar SBF responds to various intensities of physical activity [41,42]. For example, Liau et al. found that both walking speed and walking duration factors significantly affect the complexity of center of pressure (COP) by using multiscale entropy analysis, which helps clinical practitioners understand the postural control mechanism to provide an appropriate exercise program for those who have risk of foot ulcers [41]. Meanwhile, Wu et al. observed that plantar SBF increased significantly more at faster walking speed/slow running (9 km/h) in healthy adults [43]. Our current study clarified the microvascular control mechanism on subsequent plantar tissue response to walking by using wavelet analysis of BFO in healthy individuals, which could be used to quantify the abnormal responses in diabetic patients and may provide clinical experts insight to prescribe a new therapy for people with DM who have impaired microvascular reactivity [44]. Poor blood flow supply is an important pathological factor causing the development of diabetic foot ulcers [45]. However, to the best of our knowledge, there is no study applying vibration as preconditioning condition in diabetic patients and analyzing the SBF oscillations of preconditioning vibrations effect on subsequent walking. Furthermore, it remains unclear that how SBF could response to preconditioning local vibrations during different walking speeds and durations. Preconditioning local vibration may reduce blood viscosity for improving SBF [46,47]. According to the Poiseuille’s equation, Blood Flow =
Conclusions
Spectral analysis of skin blood flow oscillations provides a new window for a real-time, non-invasive assessment of plantar skin blood flow response to walking-induced ischemic stress. Our results showed that the 10-min preconditioning local vibration at 100Hz at the first metatarsal head before walking can significantly alter plantar skin blood flow responses after walking by stimulating the metabolic endothelial (0.0095–0.02 Hz) and neurogenic (0.02–0.05 Hz) controls of blood flow oscillations.
Conflict of interest
The authors declare no conflict of interest.