
Abstract
BACKGROUND:
Saliva is a complex fluid that lubricates the oropharynx and facilitates chewing, swallowing, and vocalization. Viscoelasticity is critical for the ability of saliva to fulfill these functions. Xerostomia, or a sensation of dry mouth, occurs in 17–26% of the population. Although many equate xerostomia with hyposalivation, high-risk patients frequently report oral dryness in the absence of decreased salivary flow.
OBJECTIVE:
This study aims to determine if xerostomia is associated with alterations in the rheological properties of saliva in addition to decreased salivary production.
METHODS:
The study population included patients with post-radiation xerostomia, patients with anticholinergic-induced xerostomia and healthy controls. Salivary volumetric flow rate was measured, shear viscosity was measured using oscillatory rheometry, and extensional viscosity was measured using capillary thinning methods. Groups were compared using descriptive statistics and univariate analysis.
RESULTS:
A total of 36 subjects were included: 15 with post-radiation xerostomia, 9 with anticholinergic-induced xerostomia and 12 controls. Salivary volumetric flow was significantly decreased in post-radiation and anticholinergic-induced patients compared to controls. On capillary thinning testing, saliva from xerostomia patients had significantly greater extensional viscosity compared to controls. However, saliva from the three groups showed no significant difference in the complex viscosity or the storage or loss modulus of saliva with oscillatory rheology.
CONCLUSIONS:
Xerostomia is associated with decreased salivary volumetric flow and quantitative changes in the rheologic properties of saliva.
Keywords
Introduction
Saliva is a dilute fluid composed primarily of water, electrolytes, and a mixture of mucins, lipids, proteins and other bioactive molecules which maintain homeostasis in the oral cavity and pharynx. It is secreted by acinar cells and consists of serous, mucinous, or mixed secretions depending on the salivary gland [1]. Its many functions include lubrication of oral, laryngo-pharyngeal and upper esophageal mucosa, maintenance of dental integrity, taste perception, food bolus formation, and facilitation of mastication, swallowing, voicing and speech [2].
Saliva fulfills these functions due to its viscoelastic flow behavior. Viscoelasticity describes complex fluids that demonstrate both fluid-like (i.e. viscous) and solid-like (i.e. elastic) behaviors. Fluid viscosity can be defined as the magnitude of energy dissipated during flow, while elasticity is related to amount of energy stored by the fluid. The macromolecules in saliva affect its rheological properties and define its ability to act as a lubricant. Characterizing these properties of saliva is crucial to furthering our understanding of commonly reported symptoms in the clinic, including xerostomia, globus sensation, dysphagia and dysphonia.
Xerostomia occurs in 17–26% of the population [3]. It is associated with a variety of problems including oral discomfort, burning sensations, thirst, dental caries, oral infections, dental erosion, impairment of oropharyngeal functions, loss of appetite, and fear of eating [2,4]. The most common cause of xerostomia is medication-induced [5]. As salivary glands are innervated by the parasympathetic nervous system, anticholinergic medications can be highly xerogenic [5,6]. Furthermore, xerostomia is a common source of morbidity following head and neck radiotherapy due to exposure of major and minor salivary glands to radiation. Several studies have found xerostomia to be the most common late side effect of head and neck irradiation and a major cause of reduced quality of life in head and neck cancer survivors [7,8].
Although many equate xerostomia with hyposalivation, high-risk patients frequently report oral dryness, thick mucus sticking to the throat, and associated symptoms in the absence of decreased salivary flow [9,10]. Changes to mucin structure, such as reduced glycosylation, have been suggested as possible mechanisms for xerostomia independent of hyposalivation [11,12]. In this study, we aim to examine whether alterations in salivary rheology of patients with xerostomia contribute to the clinical presentation of xerostomia.
Materials and methods
Experimental design
The protocol for this prospective clinical study was approved by the Institutional Review Board of the University of Pennsylvania. Subjects were recruited from Otolaryngology and Radiation Oncology clinics. Healthy controls were selected from the population of adult patients without xerostomia as a problem listed in their medical record or identified on their review of systems. Exclusion criteria for controls included history of autoimmune conditions, head and neck cancer, human immunodeficiency virus infection, amyloidosis, tobacco use within the past 3 months.
Inclusion criteria for post-radiation xerostomia subjects were adult patients with (1) history of conventional radiation or intensity-modulated radiation therapy (IMRT) to the head and neck region; (2) completion of treatment >12 months prior to enrollment as this is the demonstrated timeframe for onset of chronic radiation-associated xerostomia [13], and (3) subjective complaint of oral dryness. Inclusion criteria for subjects with anticholinergic-induced xerostomia were adult patients actively on anticholinergic medications with a total score of 3 or higher on the Anticholinergic Drug Scale (ADS) [14] and a subjective complaint of oral dryness. All subjects completed the Xerostomia Questionnaire (XQ), a validated instrument to measure patient-reported xerostomia [15]. Demographic data were collected including age, sex, and total radiation dose. Saliva was collected from both subjects and controls via the unstimulated whole mouth saliva method [16]. After fasting for over 1 hour, patients allow saliva to accumulate in the floor of their mouth and spit it out into specimen containers every 60 seconds for 5 minutes. The volume of saliva was calculated from the sample mass assuming a specific gravity of 1.0, and flow rate was determined in units of mL/minute.
Saliva samples were stored at 35 °C for transport, and rheometric testing was conducted at room temperature. Testing was completed within 60 minutes of collection of saliva samples to ensure integrity of the fluid. Both shear and extensional rheological properties of saliva samples were measured. Shear measurements were performed in steady and oscillatory modes using a strain-controlled TA ARES G2 rheometer equipped with a 25 mm, 0.04 rad cone geometry at 25 °C. Samples were initially sheared at 10 s−1 for 60 seconds and allowed to equilibrate for 5 minutes before being measured. Oscillatory measurements were performed in the linear viscoelastic regime with a strain of 10%. Measurements were performed at least twice on each sample to ensure that evaporation was insignificant.
Extensional viscosity measurements were performed using capillary thinning methods. Samples were extruded from a nozzle with internal diameter 2.5 mm. Flow rate was imposed using a syringe pump at 0.0002 mL/s, sufficiently slow such that flow inertia was negligible in the pinch-off process. Images were captured at 3000 fps with a resolution of 1024 × 1024 pixels using a Photron Fastcam SA1.1 high-speed camera. The evolving diameter of the neck during capillary pinch-off was measured using an edge-detection code in MATLAB. Video was taken for three drops of each sample to ensure repeatability. Capillary pinch-off time was defined as the time from necking to fracture (Fig. 3).
Statistical analysis
Continuous variables were compared with Kruskal–Wallis one-way analysis of variance, and categorical variables were compared with Fischer’s exact test. A p < 0.05 was considered significant.
Results
Demographic and volumetric results
A total of 46 patients were recruited, including 13 control patients, 13 patients with anticholinergic-induced xerostomia, and 18 patients with post-radiation xerostomia (Table 1). A total of 8 patients were excluded from analysis due to low saliva volume that prohibits rheologic measurement, including 1 control, 4 anticholinergic, and 3 post-radiation patients. The remaining 36 patients are summarized in Table 1. There were no statistically significant differences in sex (p = 0.216) or age distribution between the groups (p = 0.129). Patients with xerostomia from both groups reported significantly higher XQ scores (p < 0.001) and had decreased salivary volumetric flow compared to controls (p = 0.022).
Demographics, salivary flow rate, and capillary pinch-off time. Controls had a significantly lower XQ score, higher salivary volumetric flow rate, and lower capillary pinch-off time compared to post-radiation or anticholinergic patients
Demographics, salivary flow rate, and capillary pinch-off time. Controls had a significantly lower XQ score, higher salivary volumetric flow rate, and lower capillary pinch-off time compared to post-radiation or anticholinergic patients
The oscillatory rheology testing showed no significant difference in the complex viscosity or the storage or loss modulus of saliva between the three groups (Figs 1 and 2). In testing of extensional viscosity, control patients had an average capillary pinch-off time of 21.1 ms (95% CI: 6.7–35.5 ms); post-radiation xerostomia patients had an average pinch-off time of 39.6 ms (19.3–59.9 ms); and anticholinergic-induced xerostomia patients had an average pinch-off time of 58.1 ms (22.4–93.8 ms). Compared to controls, both xerostomia groups demonstrated a statistically significant difference in pinch-off time (anticholinergic, p = 0.020; post-radiation, p = 0.049). Figure 3 demonstrates capillary thinning of saliva from a post-radiation patient compared to a control patient. The majority of control samples had a pinch-off time less than 10 milliseconds (Fig. 4).

Complex viscosity of saliva. Saliva has an average complex viscosity of approximately 0.1 Pascal-seconds across all samples at frequency 𝜔 = 10 rad s−1. In all groups, saliva shears thin, demonstrating decreasing viscosity with increasing oscillatory frequency.
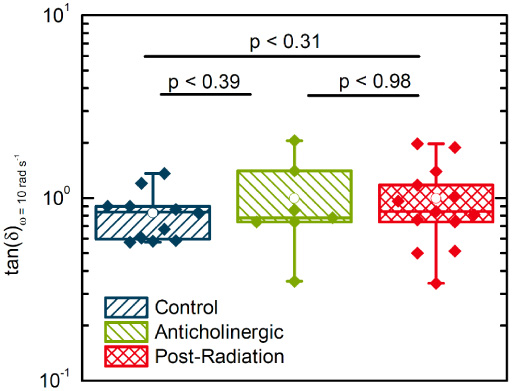
Viscoelasticity of saliva. Saliva from all groups is viscoelastic with tan(𝛿) of approximately 1. There was no significant difference in the loss modulus or storage modulus of saliva between the three groups.
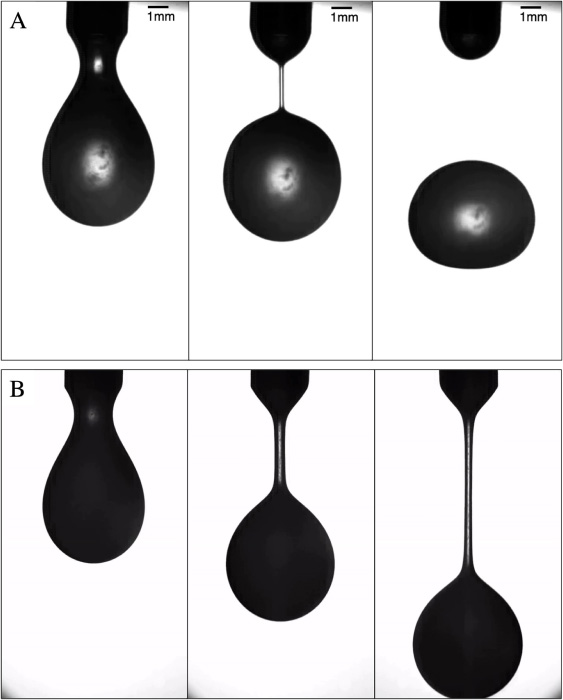
Demonstration of capillary thinning method, for control sample (A) and post-radiation sample (B). Saliva drops from time of extrusion to formation of liquid neck (0 ms for a and b) and fracture (10 ms for a; >60 ms for b); this duration is defined as pinch-off time.
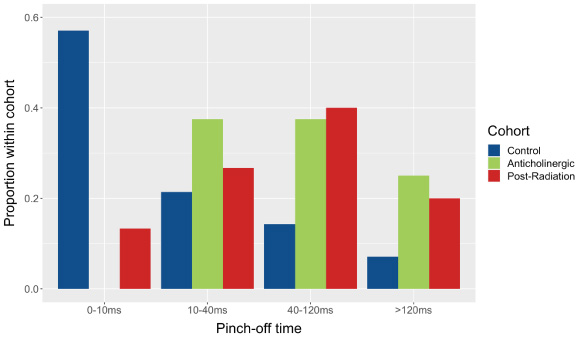
Histogram of pinch-off testing. Capillary pinch-off time of the samples on extensional viscosity testing were categorized into four bins: 0–10 ms, 10–40 ms, 40–120 ms, and greater than 120 ms or untestable.
Several samples were too thick to demonstrate capillary thinning in a reasonable amount of time, including 1 control, 2 anticholinergic, and 3 post-radiation patients. These samples are displayed in the Fig. 4 histogram within the >120 ms group, but were not included in the statistical comparison of means displayed in Table 1. These samples were also not included in the oscillatory rheology data presented in Figs 1 and 2.
Xerostomia, the subjective sensation of dry mouth, and hyposalivation, the objective measure of decreased salivary production, are frequently assumed to be equivalent. However, not all patients with xerostomia demonstrate hyposalivation [9], and not all patients with hyposalivation experience xerostomia [17,18]. Because of these observations, we hypothesize that changes in the chemical or material properties of saliva may contribute to the sensation of dry mouth.
Few studies have examined the rheological and material properties of saliva in health or disease. In the literature, it has been established that healthy saliva generally demonstrates weak shear thinning viscosity [19], and that the viscosity and viscoelasticity of saliva differ based on the method of stimulation [20,21]. Furthermore, Zussman et al. found that salivary relaxation time, a measure of extensional viscosity, varies between parotid, submandibular/sublingual and whole mouth samples and between subjects based on age [22]. There have been no studies on the flow behavior of saliva in subjects with xerostomia using rigorous rheometric techniques.
We found that patients with xerostomia have both decreased salivary volumetric flow and specific rheologic differences in saliva compared to controls. Patients with anticholinergic-induced xerostomia and those with post-radiation xerostomia demonstrate a comparable decrease in both subjective ratings of xerostomia and volumetric flow. While saliva remains viscoelastic between these disease states in our study, we demonstrated that extensional viscosity of saliva is significantly increased in patients that report xerostomia compared to controls. Due to the exclusion of samples with pinch-off time >5 minutes and the effect of outliers in the control cohort, the difference between mean capillary pinch-off times may be greater than reported in this data set.
The advantage of using objective rheological testing is that we can differentiate between different components of viscoelasticity. Specifically, changes in extensional rheology likely affect the ability of saliva to act as a lubricant as it determines surface adhesion in the oral cavity [23,24]. These properties are essential for mouthfeel and the normal swallowing process. In a study evaluating the human perception of shear and extensional viscosity, human perception was found to be more sensitive in discriminating extensional viscosity compared to shear viscosity [25]. This provides a potential explanation for the viscid sensations reported in xerostomic patients, as they may be associated with increased extensional viscosity of saliva. Notably, extensional and shear viscosity were equivalent between post-radiation and anti-cholinergic groups, suggesting that different etiologies of xerostomia may cause similar changes, in addition to inducing hyposalivation. Compositional analysis, such as measurements of water and lipid content, may further help elucidate how rheologic properties change in xerostomic patients. Importantly, this work may better inform the development of salivary substitutes and medications to increase salivary stimulation.
Limitations of this study include a small sample size that makes these results difficult to generalize to the broader population of patients with xerostomia. While not found to be statistically significant, the age difference between patients in disease vs. control groups may also play a role in the rheologic findings of this study. Dual rheologic testing requires collection of a significant volume of saliva, which eliminated severely xerostomic patients unable to produce an adequate sample. In addition, the methodology for extensional viscosity testing utilized here was could not be used for several samples of saliva from xerostomia patients, as their saliva was too thick to demonstrate capillary thinning. Utilizing a filament stretching rheometer, which does not rely on gravity, may better capture these patients and demonstrate a statistically stronger result, as it can be assumed that these samples had extensional viscosities greater than the upper limit of this study.
Conclusion
The development of rationally designed treatments for pathologic saliva has been hindered by a lack of understanding of the mechanisms of salivary dysfunction. This study demonstrates that xerostomia in medication-induced and post-radiation patients is associated with both decreased salivary volumetric flow and changes in the rheologic properties of saliva. Importantly, rheologic changes in xerostomia are best described by changes in extensional viscosity as opposed to shear viscosity. Treatment of salivary abnormalities in medication-induced and post-radiation patients will be facilitated by a more nuanced understanding of the rheology of saliva in both health and disease.
Footnotes
Funding
This work was funded by the University of Pennsylvania Department of Otorhinolaryngology-Head and Neck Surgery Faculty Pilot Grant.
Author contributions
SKR contributed to conception of this work; data acquisition, analysis, and interpretation; and drafting the work. BB and RPS contributed to the conception of this work; data acquisition, analysis, and interpretation; and revision of intellectual content of the manuscript. AC contributed to the conception of this work, data acquisition, analysis, and interpretation; and drafting the work. PA and NM contributed to the conception of this work and substantive revision of intellectual content of manuscript.
Competing interests
The authors have no competing interests or patents pertaining to the results presented in this paper.