
Abstract
The ability to repair bone defects of polycaprolactone–chitosan scaffolds containing 20% chitosan (PCL-20%CS) fabricated using the melt stretching and multilayer deposition (MSMD) technique was assessed and compared with commercial scaffolds. Two calvarium defects of 11 mm in diameter were created in each of the fifteen New Zealand white rabbits. The PCL-20%CS scaffolds were implanted in one site (group A) while another site was performed with PCL–tricalcium phosphate (TCP) scaffolds containing 20% TCP (PCL-20%TCP) fabricated by fused deposition modeling technique (FDM) (group B). At two, four and eight weeks thereafter, new bone regeneration within the defects was assessed using histomorphometric and micro-computed tomography (µ-CT) analysis. The result of histological sections demonstrated that chronic inflammatory reaction was generally detected along scaffolds of group A, but it was not found in group B. Over 8 weeks, the µ-CT analysis indicated that the average amount of new bone of group A was slightly less than that of group B (
Introduction
Composite scaffolding is a combination of two or more biomaterials aiming for synergistic properties. Poly ε-caprolactone (PCL) and chitosan (CS) are very popular biomaterials used for that purpose, due to their unique properties. Poly ε-caprolactone has been approved by the Food and Drug Administration (FDA) as a medical and drug delivery device, with extensive support both in vitro and in vivo studies [1,2]. PCL is degraded by an hydrolytic mechanism under physiological conditions and produces a less acidic environment when compared to other polyesters [2]. However, since it possesses hydrophobic properties, PCL normally takes more than 24 months for complete degrading [2], which is not commensurate with the bone remodeling process. Chitosan is the second most abundant natural polysaccharides obtained by alkaline deacetylation of chitin, derived from exoskeletons of crustaceans. Chitosan has been widely used as a biomaterial for many years due to its biocompatibility and bioactivity. It is known that the bioactivity of CS is mainly due to its cationic amine groups which can interact with anionic glycosaminoglycans (GAGs), proteoglycans and other negatively charged molecules on the surfaces of cells [3–6]. In addition, the major effects of chitosan on accelerating wound healing and promoting growth and differentiation of osteoblast cells have been reported for several years [7–12]. Recently, our research team developed the novel technique of melt stretching and multilayer deposition (MSMD) specifically for fabricating the PCL–CS three-dimensional (3D) scaffolds. MSMD processing is a melt blending technique without any porogens and solvents, therefore it is considered clean. The scaffolds including pure PCL scaffolds and PCL–CS scaffolds containing 10% and 20% CS by weight are successfully fabricated using this technique [13]. The PCL–CS scaffolds are specifically designed for enhancing osteoconductive property. A microgroove pattern, typically found on the surfaces of those scaffolds is proved to support attachment of osteoblasts [13]. An interconnecting pore system of those scaffolds is designed to be appropriate for new bone regeneration. In addition, the mechanical testing indicated that the scaffolds are suitable for withstanding forces occurring in real circumstances of the reconstruction in oral and maxillofacial region [14]. Regarding the economical consideration, the cost of the scaffolds is significantly cheaper than importing scaffolds, therefore, MSMD is the main technique for fabricating biodegradable scaffolds in our future studies.
According to our study [13], the PCL-20%CS scaffolds achieved the most superior results for supporting osteoblast proliferation, followed by PCL-10%CS scaffolds and pure PCL scaffolds, respectively. In addition, the following experiments indicated that the cells cultured on the PCL-20%CS scaffolds could produce more mineralized matrixes than those with other proportions. However, the efficacy of PCL-20%CS scaffolds for enhancing new bone formation in vivo has not yet been evaluated. In this study, ability of those scaffolds for repairing bone defects is evaluated using rabbit models and compared with that of commercial scaffolds. The benchmark is the PCL–tricacium phosphate (TCP) scaffold containing 20% TCP by weight (PCL-20%TCP) fabricated by fused deposition modeling technique (FDM), which is currently available on the market. FDM is a computer-controlled method for designing and fabricating the 3D scaffolds. Various types of the FDM scaffolds including pure PCL, PCL–hydroxyapatite (HA) and PCL–TCP have been used for several studies [15–25]. Efficacy of those scaffolds has been proven to support proliferation and differentiation of the osteoprogenitor cell and in vivo bone formation. The major advantage of the PCL–TCP scaffolds is that a calcium-rich layer forming on their surfaces during dissolution of TCP serves as a template for hydroxyapatite growth. Hence, osteoblasts can grow and differentiate on the apatite layer to form an extracellular matrix. In addition, it is claimed that the surrounding bone comes in direct contact with the surface of the layer [26]. The aim of this study is to comparatively assess new bone regeneration within the rabbit’s calvarial defects enhanced by the PCL-20%CS and the PCL-20%TCP scaffolds.
Materials and methods
The scaffolds and study groups
The study groups included group A: PCL-20%CS scaffolds and group B: PCL-20%TCP scaffolds (
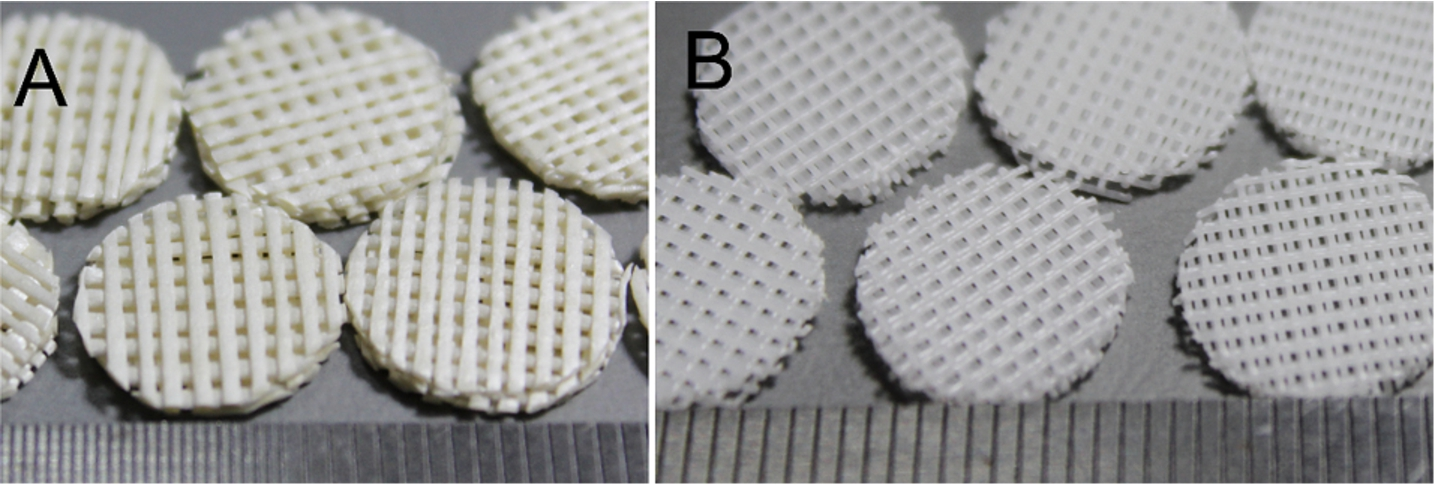
Pictures of the testing scaffolds (A) PCL-20%CS scaffolds and (B) PCL-20%TCP scaffolds. (Colors are visible in the online version of the article;
Fifteen adult male New Zealand white rabbits weighing 2.5–3.0 kg were included in this study according to standard animal care protocols at the Animal Housing Unit, Faculty of Science, Prince of Songkla University. The implantation procedures in the rabbits were performed under general anesthesia using an intravenous injection of 1 mg/kg diazepam. Each rabbit was placed in the prone position and mid-sagittal skin incisions over the skulls were performed after injection of local anesthesia. After sub-periosteal dissection, bi-cortical defects (11 mm in diameter) were created at both sides of its calvarium. The scaffold specimen of group A was randomly implanted in one side of its calvarium and the other side was implanted with the scaffold specimen of group B (Fig. 2), and then the skin flap was closed with 4/0 absorbable sutures. All rabbits received postoperative antibiotic prophylaxis with 0.1 ml/kg cephalexine for 3 days. At the time points of 2, 4 and 8 weeks after the operation, the surgical wounds were clinically assessed. Healing and any complications of the surgical sites were evaluated and descriptively recorded. After that, the rabbits were sacrificed with an overdose of intravenous pentobarbital sodium (5 rabbits/time point). Each calvarium including two implanted sites was removed in 1 piece and it was fixed in 10% formalin. After 48 h, it was cut along the mid sagittal suture into 2 pieces using a cutting–gridding machine (Exakt, Germany). Micro-computed tomography (µ-CT) analysis was performed in all specimens before processing them for histomorphometric analysis (5 specimens/group/time point).

The two bi-cortical defects created at both sides of the calvarium and implanted with the scaffolds; on the right is the PCL-20%CS scaffold and the left one is the PCL-20%TCP scaffold. (Colors are visible in the online version of the article;
The specimens of each time point were scanned using a µ-CT machine (µCT 35, SCANCO Medical AG, Switzerland) in a direction parallel to the coronal aspect of the calvariums with a setting of 55 kVp, 72 µA and 4 W. New bone formation within each implanted site (Fig. 3(A)) was measured as the new bone volume fraction (VF) calculated by an analysis software (µCT 35, version 4.1, SCANCO Medical AG, Switzerland) using the following formula:
Histologic processing and histomorphometric analysis
The specimens were decalcified in formic acid and embedded in paraffin. For each specimen, serial 5-µm-thick sections were cut at the positions of 500 µm from the midline (Fig. 3(A)). The sections were stained with Haemotoxylin and Eosin (H&E), and Masson’s trichrome (MT) (2 sections/specimen/staining). The stained sections were observed under a light microscope (Nikon, Tokyo, Japan) and scanned using a slide-scanner (ScanScope, Aperio, USA) to be image files. The region of interest (ROI) was located between the rims of both sides of the defect including the newly formed bone, the remaining scaffold and its surrounding tissue. Microscopic features of the ROI were assessed descriptively. Area fractions (AF) of newly formed bone and remaining scaffold were calculated by the following formulas using analysis software (ImageScope, Aperio, USA) (Fig. 3(B)). Those parameters were measured as percentages to prevent error due to shrinkage of the specimens:
Statistical analysis
The data was analyzed using statistics analysis software (SPSS, version 14.0, USA). The microscopic features of the scaffolds and the surrounding tissue were assessed descriptively. One-way Analysis of Variance (ANOVA) followed by Tukey HSD was applied to compare the differences of the measured parameters among the healing intervals within each group. Dunnett’s T3 test was performed when equal variances was not assumed. The paired t-test was applied to compare the differences of those parameters between the two groups for each time point. The level of statistical significance was set at a
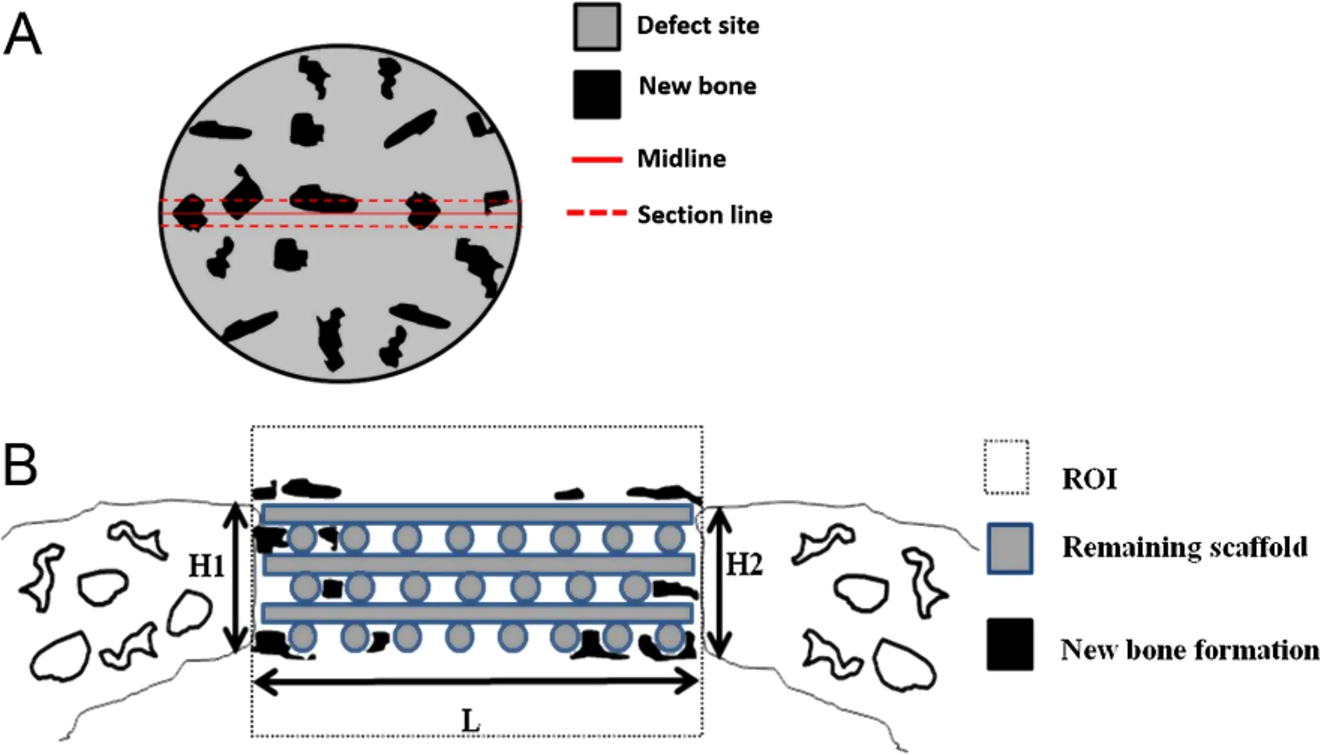
(A) schematic drawing for defining the defect site for the µ-CT analysis and the section lines for the histomorphometric analysis and (B) for defining the ROI for the histomorphometric analysis. (Colors are visible in the online version of the article;
All rabbits of both groups tolerated the operation well and they were healthy during the observation period. The surgical wounds healed without complication. The gross specimens of 8 weeks showed that the implanted sites could integrate to the surrounding host bone. The defects were covered with dense fibrous tissue without signs of foreign body reaction.
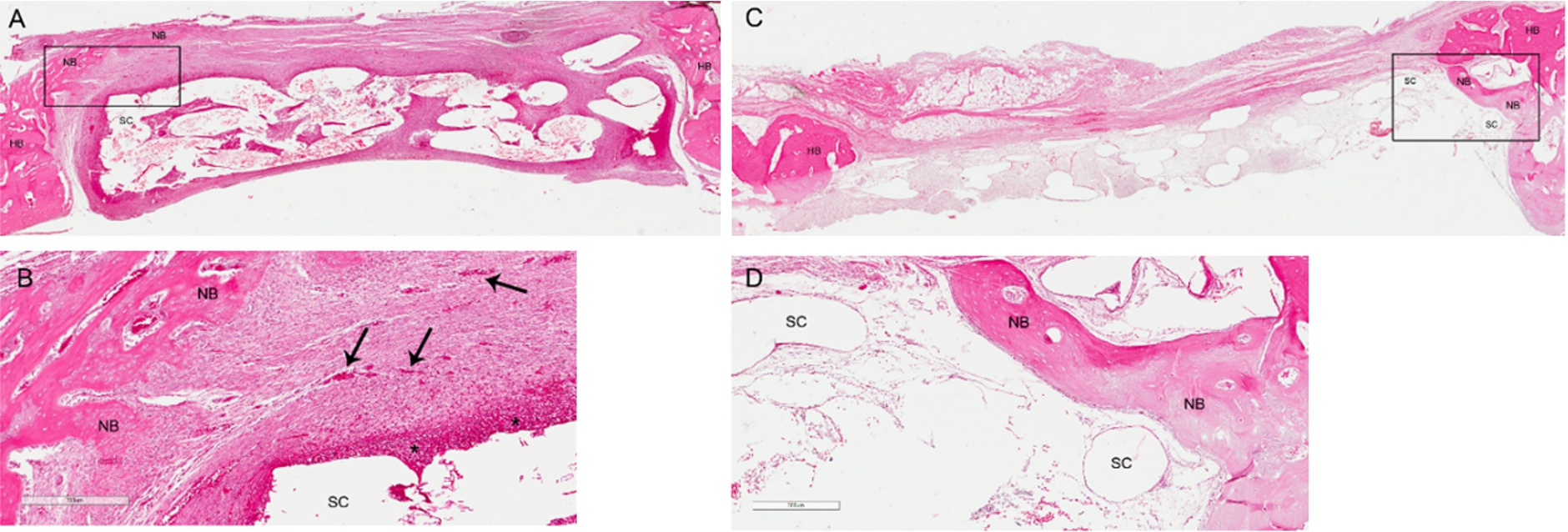
The H&E stained sections of the implanted sites after two weeks: ((A) and (B)) group A, ((C) and (D)) group B. (A) The section reveals newly formed bone regenerating from the periphery of the host bone (box). (B) The magnified image of the box reveals that the PCL-20%CS scaffold is surrounded by dense fibrovascular tissues (scale bar; 300 µm). Regeneration of several new vessels (arrows) and inflammatory cells accumulating along the surface of the scaffold (asterisks) are seen. (C) New bone tends to regenerate into the inner portion of the PCL-20%TCP scaffold (box). (D) The magnified image of the box in picture (C) (scale bar; 300 µm), the filaments of the scaffold are surrounded with loose connective tissue stromal without inflammatory response. Abbreviations: NB – newly formed bone, HB – host bone, SC – scaffold. (Colors are visible in the online version of the article;
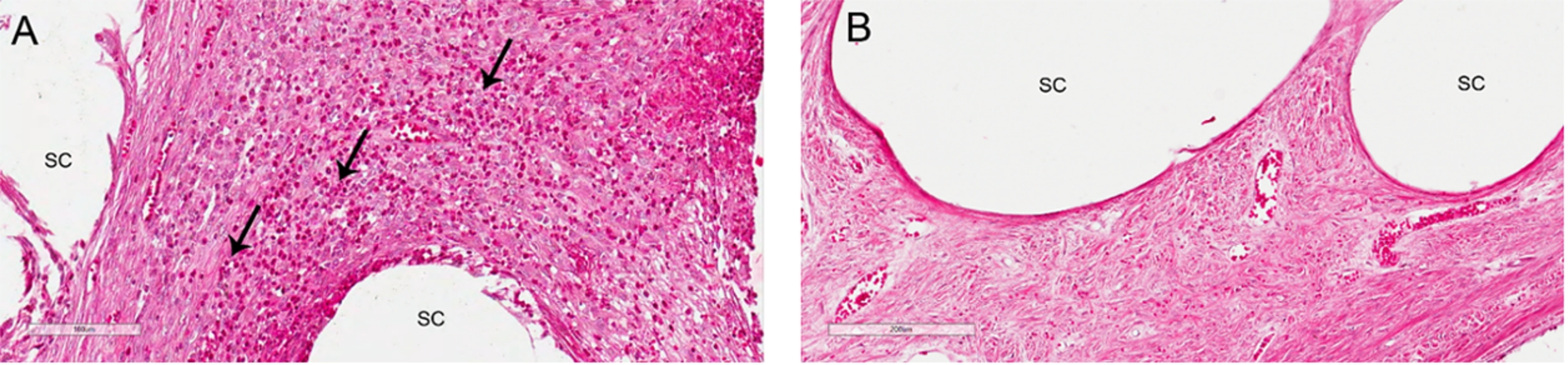
(A) Eosinophils are dominant and generally found along the surfaces of the PCL–CS scaffold (arrows) (scale bar; 100 µm). (B) Absence of those cells is detected along the surfaces of the PCL–TCP scaffold (scale bar; 200 µm). Abbreviations: SC – scaffold. (Colors are visible in the online version of the article;
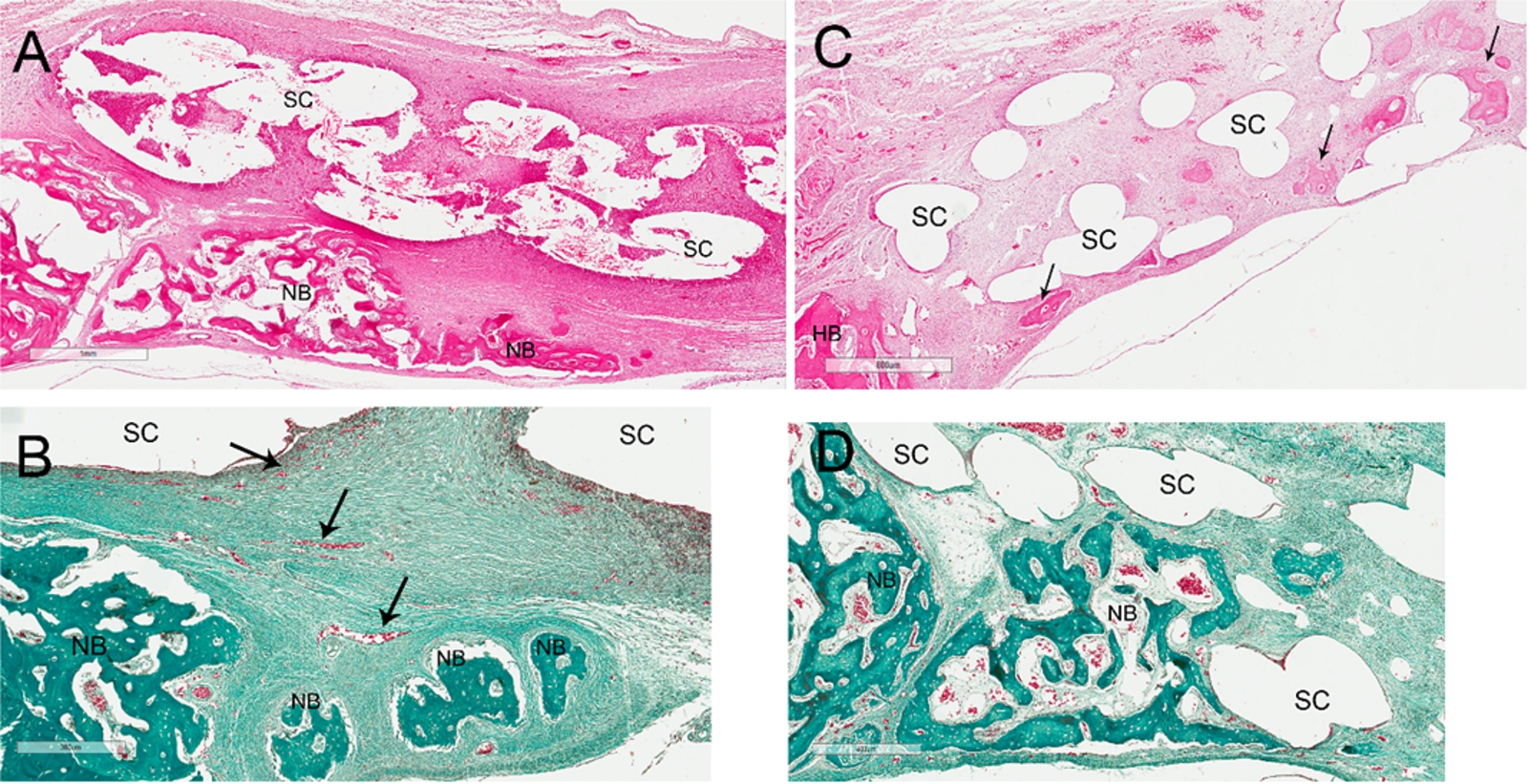
The stained sections of the implanted sites after four weeks: ((A) and (B)) group A, ((C) and (D)) group B. (A) The H&E stained section reveals increasing new woven bone along the floor of the defect beneath the PCL-20%CS scaffold (scale bar; 1000 µm). Vascularized stromal connective tissue is found within the medullary space of the newly formed bone. (B) The MT stained section demonstrates remarkable decrease of the inflammatory response along with an increase of dense collagen stromal and several newly formed small vessels (arrows). Newly formed woven bone is also indicated (scale bar; 300 µm). (C) The H&E stained section reveals some areas of new bone formation within the PCL-20%TCP scaffold (arrows) (scale bar; 800 µm). (D) The MT stained section reveals an increase of woven bone formation along the floor of the defect (scale bar; 400 µm). Abbreviations: NB – newly formed bone, HB – host bone, SC – scaffold. (Colors are visible in the online version of the article;
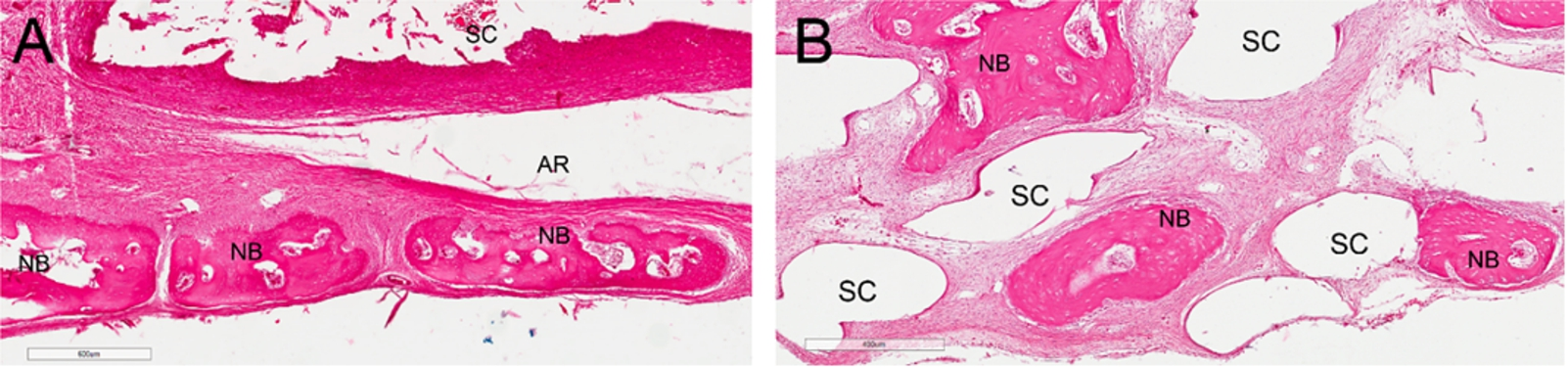
The H&E stained sections of the implanted sites after eight weeks: (A) group A and (B) group B. (A) Regular pattern of the bone foci beneath the PCL-20%CS scaffold indicates that the newly formed bone matures and remodels (scale bar; 600 µm). Smaller marrow spaces within the bone foci indicate the mature lamella bone. An artifact space from the histological sectioning is also seen. (B) The section shows areas of lamella bone formation along the pores of the PCL-20%TCP scaffold (scale bar; 400 µm). Abbreviations: AR – artifact space, NB – newly formed bone, SC – scaffold. (Colors are visible in the online version of the article;
Histological features of the implanted areas were demonstrated in Figs 4–7. During the histological preparation, the scaffolds of both groups totally dissolved, hence the scaffold areas in the histologic images were seen as empty spaces. At week 2 (Fig. 4), the scaffolds of both groups were surrounded by dense fibrous tissue and neo-vascularization was clearly found throughout the inner parts of them. Chronic inflammatory cells, which mainly included eosinophils and histeocytes, were generally found infiltrating along the surfaces of the PCL-20%CS scaffolds, but those cells were not detected in the PCL-20%TCP group (Fig. 5). New bone formation could be detected extending from the periphery of the defects. In week 4 (Fig. 6), an increase of neo-vascularization along with dense collagen connective tissue within the scaffolds was detected in both groups. A remarked decrease of the inflammatory response was observed in group A. The amount of new bone formation of both groups remarkably increased. It was found that the newly formed bone could regenerate into the deeper parts of the PCL-20%TCP scaffolds but this was not found in the PCL-20%CS scaffolds. In week 8 (Fig. 7), most of the newly formed bone within the defects of both groups matured and remodeled, hence it was difficult to distinguish between the newly formed bone and the host bone margins. No complete bony bridging of the defects and no bone-scaffold integration was found in either group. During the observation period, it was noted that the bone formation of the PCL-20%CS scaffolds was detected mostly along the peripheries of the scaffolds rather than within the scaffolds. In contrast, bone regeneration was detected both within the PCL-20%TCP scaffolds and along their periphery. The newly formed bone AF is demonstrated in Fig. 8. The data shows that the new bone formation of group A was less than that of group B at all time-points and that significant difference was found at week 8. The remaining scaffold AF is demonstrated in Fig. 9. It was found that the scaffold areas of the PCL-20%CS group were significantly greater than those of the PCL-20%TCP group at all-time points.
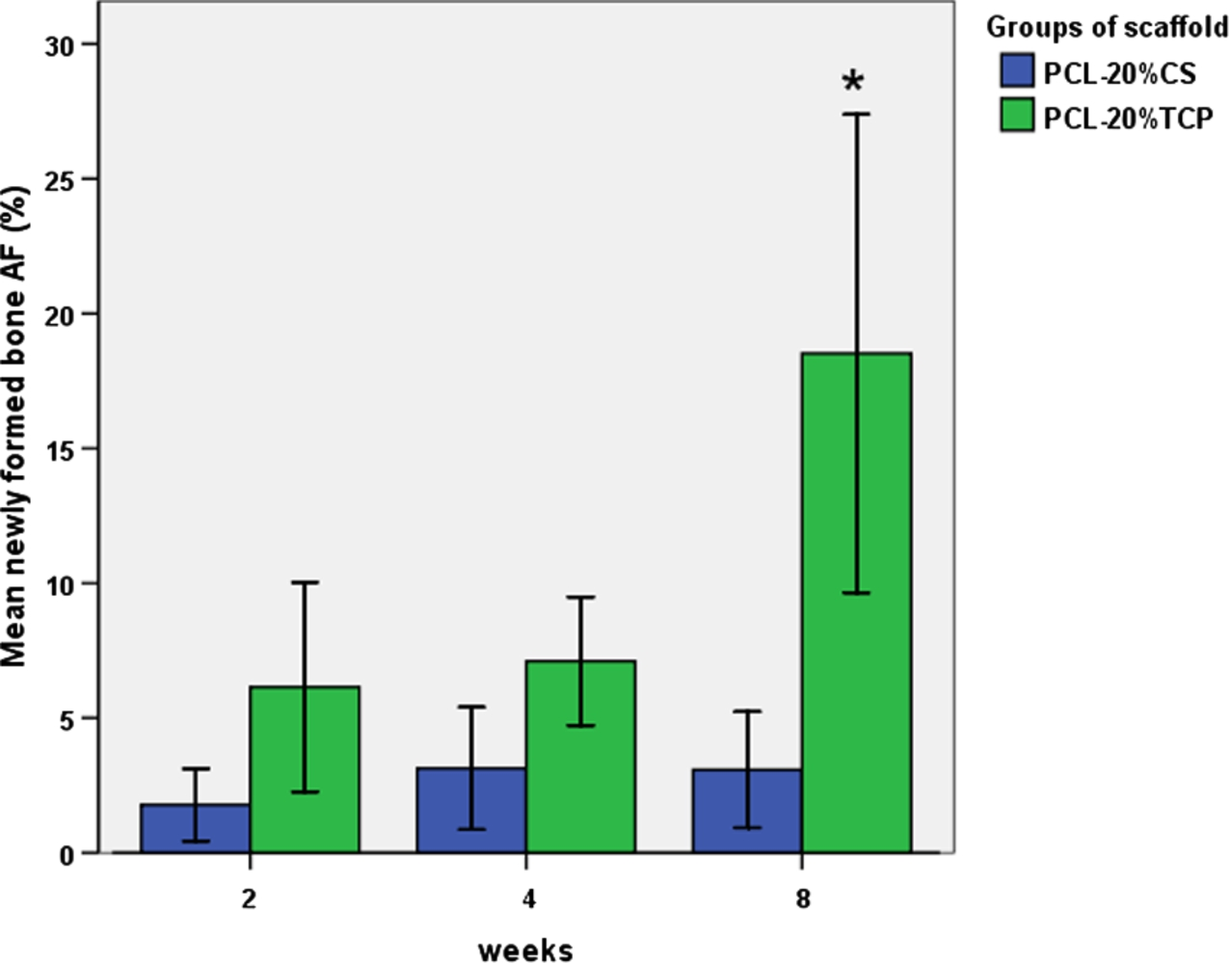
The graph of the newly formed bone AF, indicates that the new bone formation of the PCL-20%CS group was less than that of the PCL-20%TCP at all time points. At week 8, the bone formation of the PCL-20%TCP group increased significantly more than at other time points and than those of the PCL-20%CS group (ANOVA,
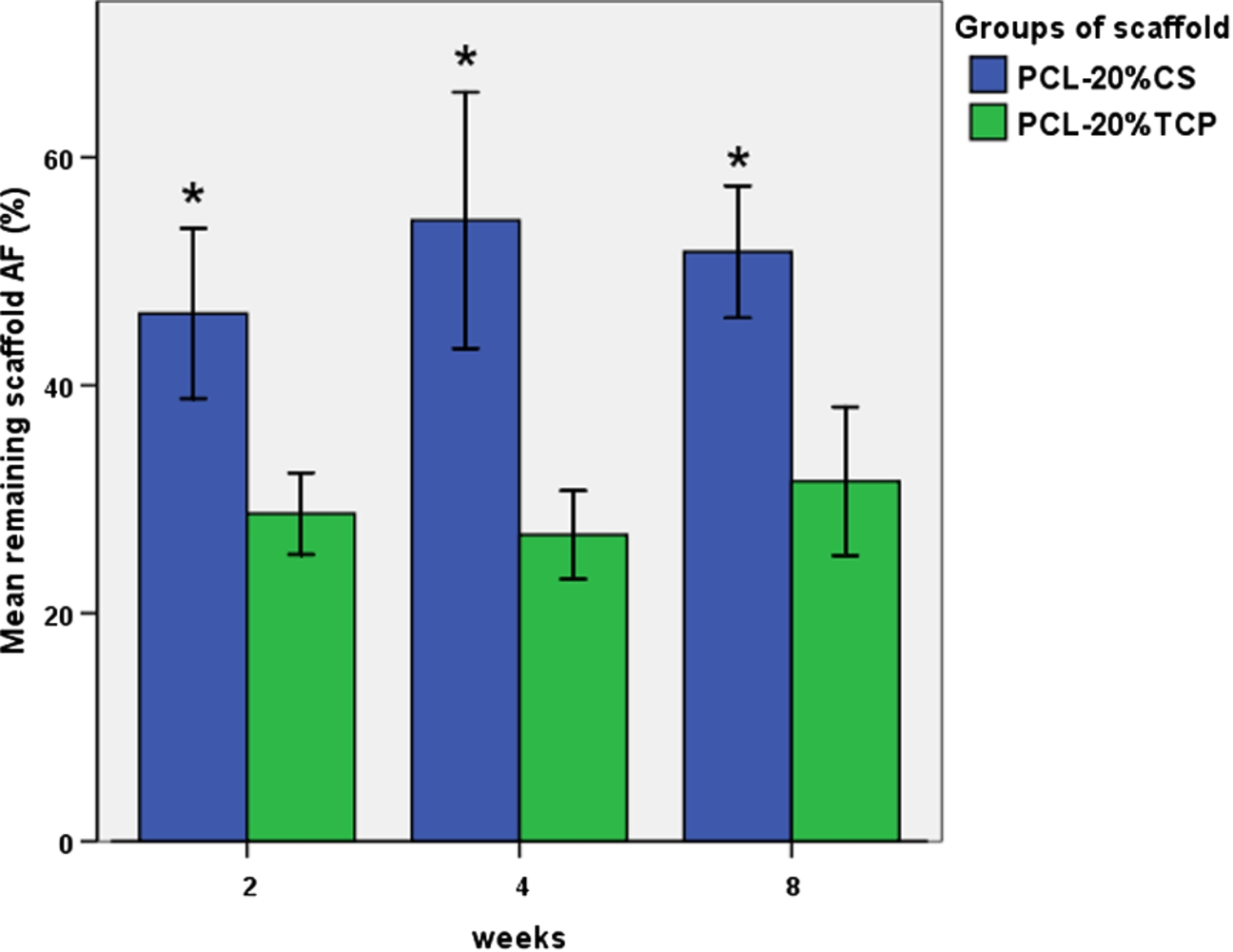
The graph of the remaining scaffold AF, shows that the scaffolds of group A significantly occupied larger areas in the defect spaces than those of group B at all time points. ∗
Morphologies of the implanted sites of both groups at over 8 weeks are demonstrated in Fig. 10. Newly formed bone initially regenerated from the defect borders and gradually increased its volume. Corresponding to the histological features, the PCL-20%TCP scaffolds could allow for more bone regeneration into their deeper parts than the PCL-20%CS scaffolds. The new bone volume fractions over 8 weeks are demonstrated in Fig. 11. It was found that the newly formed bone of the PCL-20%CS group gradually increased with time, whilst that of the PCL-20%TCP remarkably increased after week 4.
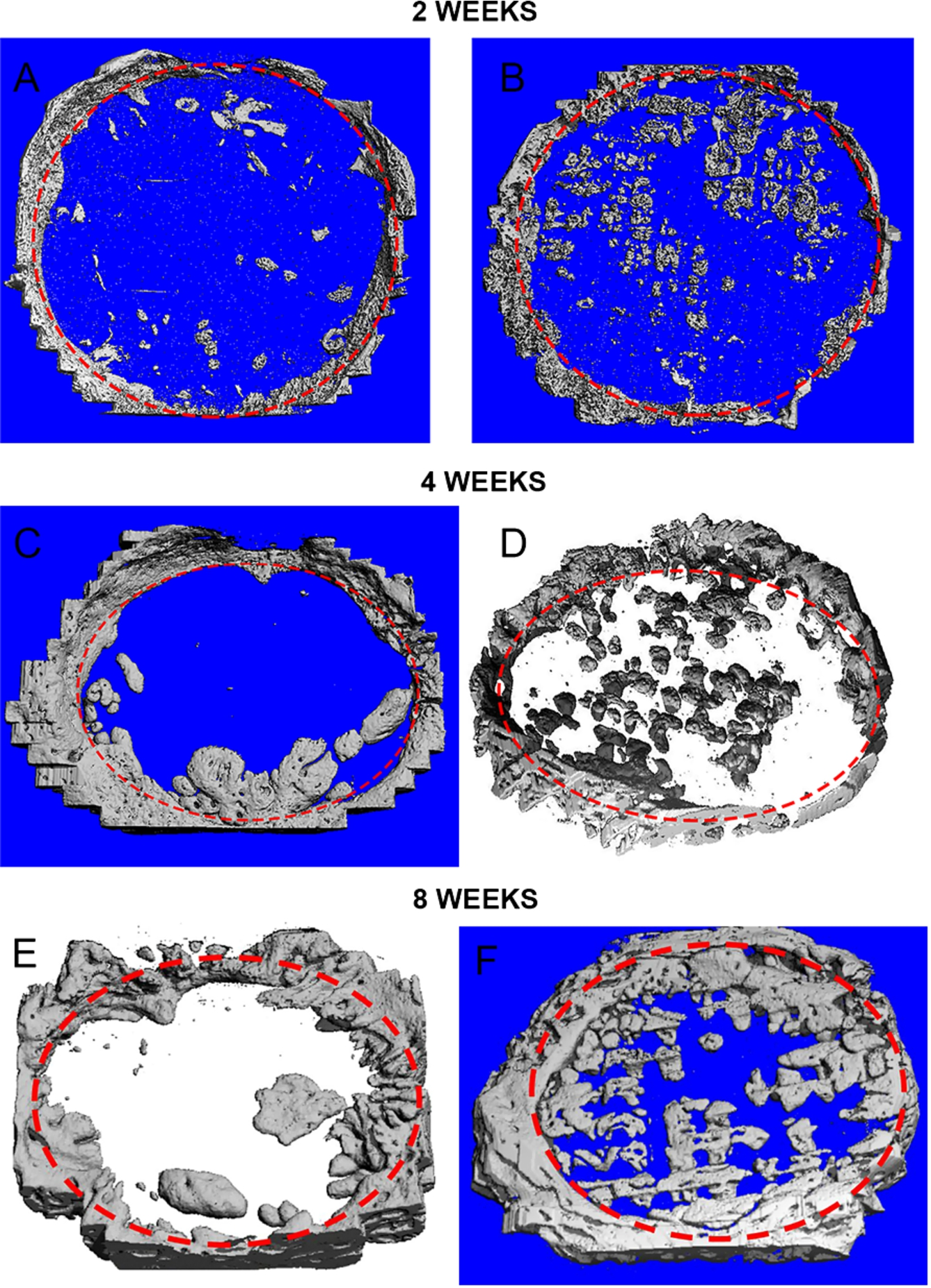
3D reconstructed pictures of the µ-CT images; pictures (A), (C) and (E) are group A and pictures (B), (D) and (F) are group B. The pictures of both groups show that new bone could regenerate into the defects and increase its volume over 8 weeks. In group A, new bone formation was detected mostly along the floors of the defects or beneath the scaffolds. In group B, new bone could regenerate into deeper parts and along the pores of the scaffolds. Dotted line – defect margin. (Colors are visible in the online version of the article;
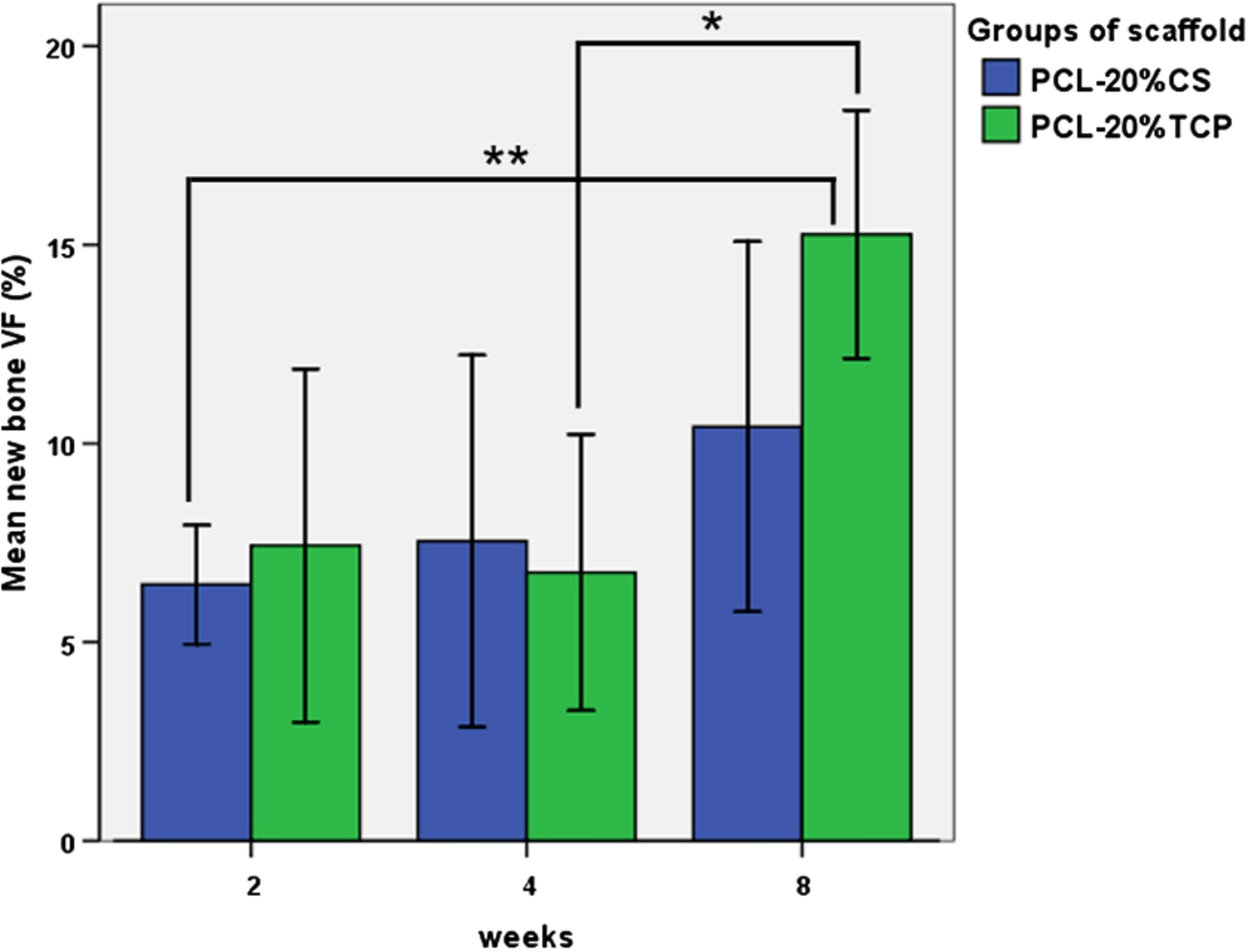
The bar graph demonstrates the new bone VF, over 8 weeks. The amount of new bone formation of both groups increased with time. At week 8, the new bone in group B significantly increased from week 4 and it was also significantly greater than that of group A at week 2 (Tukey HSD, ∗
The results of this study mainly revealed the osteoconductive and osteoinductive properties of the PCL–CS 20% MSMD scaffolds by focusing on their ability to enhance new bone regeneration in the in vivo bone defects. Those properties were compared with current commercial scaffolds to assess the possibilities for future experiments or clinical trials. However, some protocols of this experiment were different from those of the previous studies. Firstly, the 11-mm defect is smaller than the critical size defect of 15 mm in diameter by definition [27]. Several previous studies created their defect size in rabbit models within the range of 10–15 mm in diameter [28–32]. Recently, Sohn et al. [32] created 15-mm and 11-mm defects in rabbits and they found that spontaneous new bone formation of both groups in 8 weeks were not significantly different. In our rabbit models, two 15-mm defects could not be created in each cranium due to inadequate space, therefore, the two 11-mm defects were created instead in order to compare the efficacy of the two materials and reduce the errors between individuals. Secondly, our observation period was shorter than those of previous similar studies which ranged from 12 weeks to 9 months [20,21,23,33,34]. In our opinion, the duration of 8 weeks corresponds to the period of bone remodeling process in humans, and it was sufficient for estimating the efficacy for enhancing bone regeneration of tested scaffolds. Finally, we combined the micro CT and the histomorphometric analysis in the same specimen for a better assessment of bone regeneration. The VF measured by the CT is the most accurate value for implying the total new bone formation within the defects in 3D. Nevertheless, degradation or dimensional change of the scaffolds could not be comparatively assessed using the micro CT due to the very low density of the PCL–CS scaffolds. The AF measured by the histomorphometric analysis is less accurate for evaluating that bone formation and its volume is usually less than the VF. It is due to that bone can be seen only along the directions of the tissue sectioning that commonly done through the midline of a specimen. However, histomorphometric data is still the best method for demonstrating information regarding tissue responses to the scaffolds and maturity of the new bone. In addition, that data could reveal the areas of radiolucent PCL–CS scaffolds that could not be detected by the micro CT.
This study indicates that both types of scaffolds are biocompatible and can be implanted into in vivo bone defects without complications. The histological sections demonstrated that the interconnecting pore systems of both types of scaffolds could allow vessel regeneration throughout their inner portions, which can increase the tissue healing and survival of the grafted scaffolds. New bone formation could regenerate from the host bone margins and gradually increased with time to consecutively occupy the defects. In addition, remodeling of the new bone was detected after week 4. To measure the amount of new bone formation, correspondence between the AF and the VF was detected. The profiles of the VF demonstrated that the average new bone regeneration enhanced by the PCL-20%CS scaffolds was slightly less than that of the PCL-20%TCP scaffolds. Nevertheless, both of them could only gain a small amount of new bone into the defects. At week 8, the averages of new bone VF was only 10.42 ± 5.21% in the PCL-20%CS group and 15.26 ± 3.49% in the PCL-20%TCP group. This result is similar to those reported in some studies [20,21,33] which supported that the ability of the scaffolds alone seem to be insufficient for reconstructing large bone defects. Khojasteh et al. [35] implanted the PCL-20%TCP scaffolds into 20 × 10 × 10 mm-critical sized defects in dog’s mandibles and found that the amount of new bone formation was 17.27 ± 3.29% after 8 weeks. Rai et al. [33] extended the observation period to 9 months for implantation of the same scaffolds into the 18 × 10 × 7 mm-mandibular defects of mongrel dogs. They also found the minimum amount of new bone formation enhanced by the scaffold increasing from 5.07 ± 2.13% to 9.78 ± 1.11% from 6 to 9 months. Similarly, Sawyer et al. [20] found that PCL-20%TCP scaffolds alone could gain average new bone volume of less than 20% of the 5 mm-rat calvarial critical-sized defect by 15 weeks.
Although the PCL-20%CS scaffolds were proved to support growth and differentiation of the osteoblast cells in vitro excellently, this study demonstrated that they failed to enhance enough new bone regeneration for repairing bone defects in the animal models. The results also revealed two major problems of the MSMD scaffolds that require correction. Firstly, the scaffolds allowed less bone regeneration into the deep parts of their structures than the FDM scaffolds. The large AF of our scaffolds implied that they occupied excessive spaces in the defects that might be a barrier, especially to the regeneration of peripheral bone into their middle portions. Modifications to reduce the AF of the scaffolds will include decreasing the diameter of the scaffold’s filaments as well as increasing the space areas between the filaments. Secondly, regarding using the same matrix of PCL, the CS filler appeared to be inferior to the TCP filler in term of inducing more inflammatory responses in vivo. It corresponds with the reports of some studies which supporting the correlation between chitosan and induction of inflammatory cells [36–39]. Reese et al. [39] reported that chitin as well as chitosan could induce tissue accumulation of IL-4-expressing innate immune cells, including eosinophils and basophils when given to mice. Barbosa et al. [36] reported that the biological response to implanted chitosan scaffolds was influenced by the degree of acetylation (DA). They found that the DA 15% chitosan scaffolds induced a more intense inflammatory response when compared with the DA 4% scaffolds. The DA 15% chitosan attracted high numbers of leukocytes and induced a high infiltration of inflammatory cells within the scaffolds. The authors also suggested that acetyl and amine functional groups of chitosan played an important role in that phenomenon. VandeVord et al. [38] implanted porous chitosan scaffolds (DA 92%) in mice and found marked infiltration of neutrophil, which resolved with increasing implantation time. They suggested that this phenomena was due to the specific interactions of chitosan or its oligosaccharides with the neutrophil receptors. Chitosan has also a chemotactic effect on immune cells, but this effect does not lead to a human immune response. Therefore, the authors supported the biocompatibility of a 92% chitosan scaffold due to inducing minimal signs of inflammatory reaction in the implanted sites and no evidence of infection. That effect was similar to the result of our study, but the PCL-CS scaffolds seem to specifically induce eosinophils and histeocytes rather than neutrophils. Regarding those results, using CS (DA 75–85%) as the filler of the PCL-based scaffolds seems to be inappropriate for repairing bone defects. However, by using the concept of the MSMD technique, several filler materials which have stable properties within the range of 100–120°C [13] can be easily combined with the PCL. Among those materials, bioactive biphasic calcium phosphate (BCP) with various ratios of HA:TCP developed by our institute is currently being experimented [40], and we plan to use the BCP filler for the PCL-based MSMD scaffolds in the future.
Conclusion
In conclusion, efficacy of the PCL-20%CS MSMD scaffolds for repairing the calvarial defects was less than that of the PCL-20%TCP scaffolds over 8 weeks. Nevertheless, the ability of both types of scaffold can gain small amounts of new bone regeneration that is insufficient for reconstructing larger bone defects. Chitosan seems to be an inappropriate filler for the PCL-based scaffolds for repairing bone defects in terms of inducing some specific inflammatory cells. However, the concept of MSMD scaffolding is still valuable and available for further modifications.