
Abstract
The Lachman test is considered to be a reliable physical examination for anterior cruciate ligament (ACL) injury. Patients with a damaged ACL demonstrate a soft endpoint feeling. However, examiners judge the soft and hard endpoints subjectively. The purpose of our study was to confirm objective performance of the Lachman test using joint auscultation. Human and porcine knee joints were examined. Knee joint sound during the Lachman test (Lachman sound) was analyzed by fast Fourier transformation. As quantitative indices of Lachman sound, the peak sound as the maximum relative amplitude (acoustic pressure) and its frequency were used. The mean Lachman peak sound for healthy volunteer knees was 86.9 ± 12.9 Hz in frequency and −40 ± 2.5 dB in acoustic pressure. The mean Lachman peak sound for intact porcine knees was 84.1 ± 9.4 Hz and −40.5 ± 1.7 dB. Porcine knees with ACL deficiency had a soft endpoint feeling during the Lachman test. The Lachman peak sounds of porcine knees with ACL deficiency were dispersed into four distinct groups, with center frequencies of around 40, 160, 450, and 1600. The Lachman peak sound was capable of assessing soft and hard endpoints of the Lachman test objectively.
Introduction
The Lachman test is clinically considered to be a reliable physical examination for anterior cruciate ligament (ACL) injury [1–5]. To perform the test, the patient lies on an examination table and the examiner holds the patient’s knee between 20 and 30 degrees of flexion. The patient’s femur is stabilized with one of the examiner’s hands, while the proximal aspect of the tibia is moved forward with the other hand. Not only the degree of tibial anterior translation but also the endpoint feeling of movement offer important information about the ACL condition [5]. Patients with a damaged ACL may demonstrate more anterior translation and a soft endpoint feeling during the Lachman test. However, the Lachman test is often difficult within the acute phase of ACL injury, because swelling and pain cause guarding by the patient. Instrumented arthromeres can be a helpful in the diagnosis of an acute ACL injury; a maximum manual side to side differences of 3 mm or more is diagnosis of an ACL tear [6]. These devices can assess the degree of tibial anterior translation.
Now, we have investigated a new testing device of ACL injury from a different standpoint to assess an endpoint feeling during the Lachman test objectively. Therefore, we utilized a knee auscultation to assess the Lachman test and analyze knee joint sound using fast Fourier transformation [7]. In this feasibility study, we examined whether our system can accurately evaluate knee joint sound during the Lachman test. The goal of our study was to confirm objective performance of the Lachman test using joint auscultation, which would allow another approach of arthrometric diagnosis of all patients with ACL injury.
Methods
Knee joint auscultation system
An outline of the knee joint auscultation system is given in Fig. 1. A contact microphone (FL-330; Sun-mechatronics, Tokyo, Japan) was placed on the medial suprapatella area, which was coated with an ultrasound transmission gel (Sono Jelly; Toshiba Medical Supply Co. Ltd., Tokyo, Japan). The gel was used to effectively eliminate skin friction noises caused by slight movement of the microphone during tibial translation in the Lachman test. The contact microphone was fixed with Velcro tape. The contact microphone was connected to an IC recorder (R-05; Roland, Hamamatsu, Japan) through an equipped small amplifier. The knee joint sound (hereinafter described as Lachman sound) was recorded during 10 tibial translations of the Lachman test. The Lachman sound was recorded in the WAV file format at 16 bits/44.1 kHz (bit rate/sampling rate). The Lachman sound data were converted into a spectrogram by fast Fourier transformation. Figure 2 shows typical digitized audio data of the Lachman sound (upper) and the resulting spectrogram (lower). The Lachman sound spectrogram comprises a two-dimensional map with the x-axis and y-axis representing the time and frequency, respectively, and the relative amplitude (acoustic pressure) is indicated by the color grade. As quantitative indices of Lachman sound, we measured the peak sound of the fifth tibial translation as the maximum relative amplitude and its frequency. Five measurements of the Lachman peak sound were evaluated for each knee.
Configuration of the knee joint auscultation system.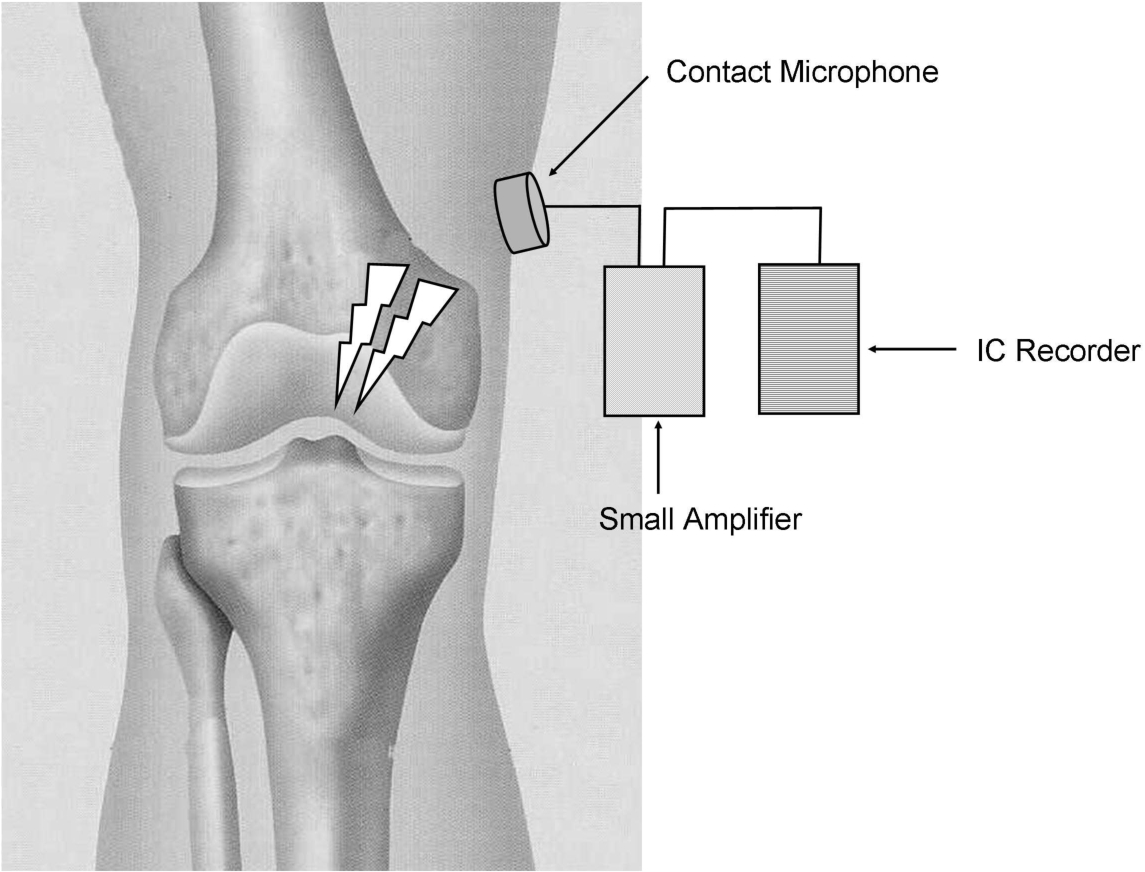
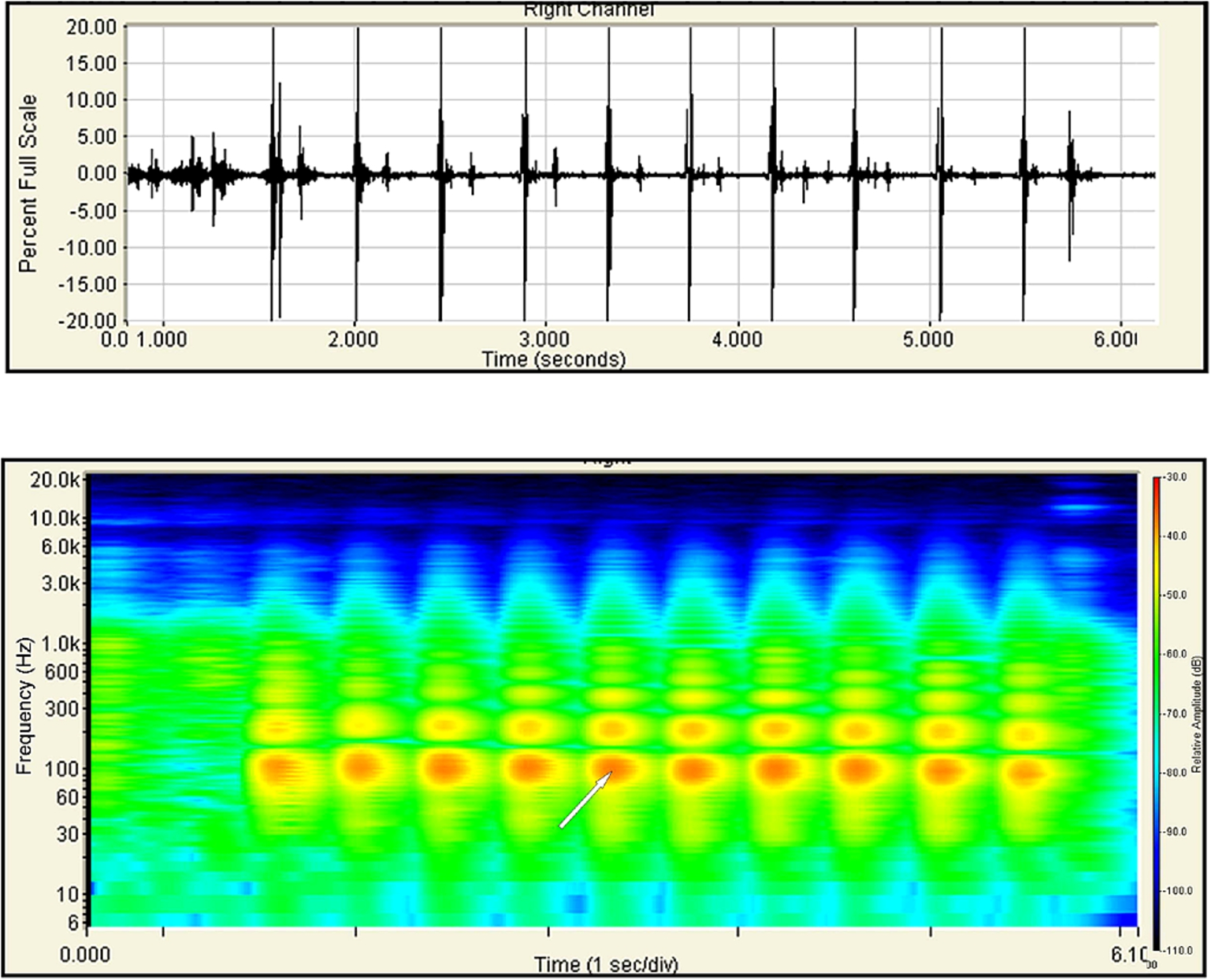
Typical human knee joint sound (Lachman sound) with a hard endpoint of the Lachman test. Digitized audio data (upper) were converted into a spectrogram (lower) by fast Fourier transformation. The spectrogram comprises a two-dimensional map with the x-axis and y-axis representing the time and frequency, respectively, and the relative amplitude (acoustic pressure) is indicated by the color grade. As quantitative indices of Lachman sound, the peak sound of the fifth tibial translation as the maximum relative amplitude and its frequency are selected (white arrow).
Twenty-three healthy male volunteers (average age, 40.9 years; age range, 25–57 years) underwent Lachman sound analysis during the Lachman test. The Lachman sound of the right knee was recorded and analyzed by the above-described methods. All volunteers provided informed consent and the study was approved by the Konan Women’s University Ethics Committee.
Porcine right legs were also prepared for this study. Ten porcine legs with preserved soft tissues (muscle, ligament, and capsule) around the knee joint were delivered within 10 h of slaughter, and stored at below −30°C until use. During preparation, the lower legs were first defrosted at 20°C. The Lachman sound of the porcine knee joints was recorded and analyzed by the above-described methods. Subsequently, a small incision was made on the patella ligament of the lower leg using a scalpel and surgical scissors were inserted into the cruciate ligaments. The ACL and posterior cruciate ligament (PCL) were cut off blindly. The Lachman sound of the porcine knees with ACL and PCL deficiency was then recorded and analyzed by the above-described methods. The Lachman tests of the volunteer and porcine knee joints were performed by a specialist in orthopedic surgery approved by the Japanese Orthopaedic Association (KH).
Results
The Lachman peak sounds of the healthy male knees are shown in Fig. 3. All male knees had a hard endpoint feeling during the Lachman test. The mean frequency of the Lachman peak sound of the knees was 86.9 ± 12.9 Hz, and the mean acoustic pressure of the Lachman peak sound was −40 ± 2.5 dB. The Lachman peak sounds of the healthy male knees were centered around 90 Hz.
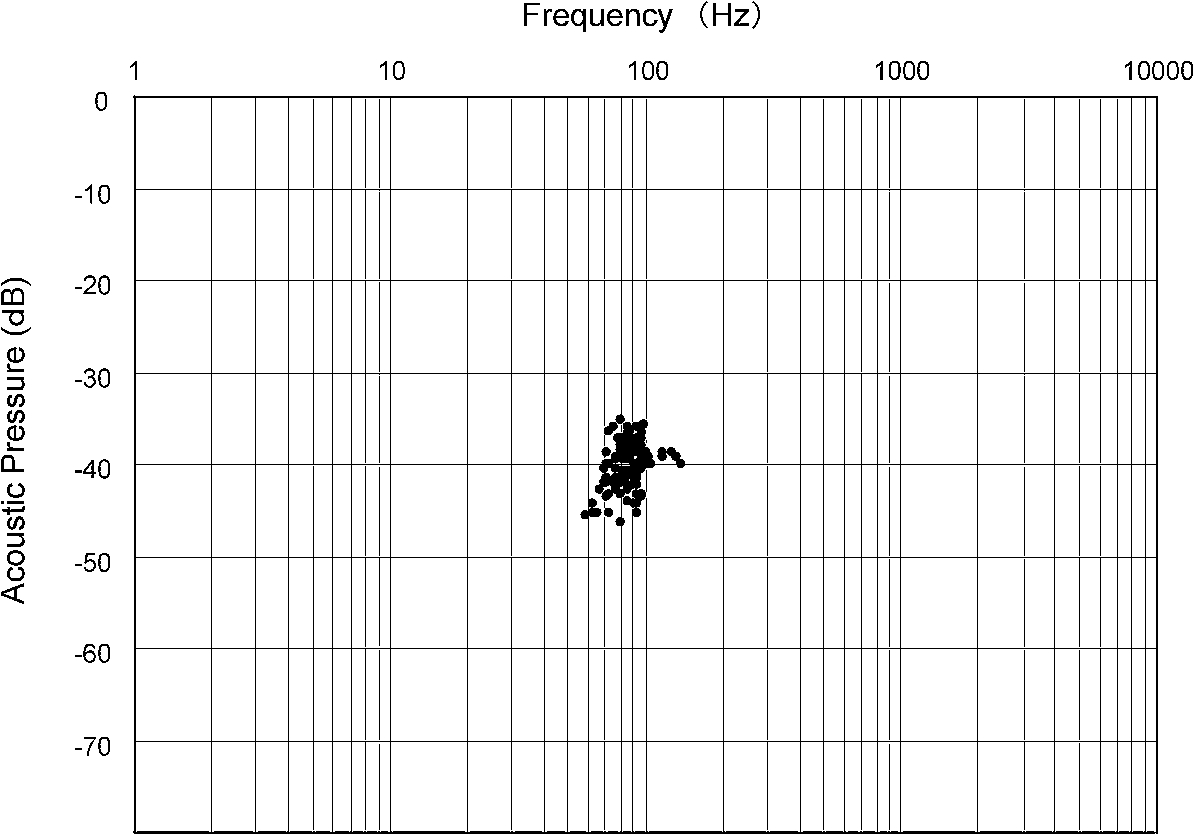
Acoustic distribution charts of the Lachman peak sound obtained from healthy male volunteer knees (total of 115 points in 23 male knees) presenting the hard endpoint of the Lachman test.
The Lachman peak sounds of the porcine knees are shown in Fig. 4. All intact porcine knees had a hard endpoint feeling during the Lachman test. All porcine knees with ACL and PCL deficiency had a soft endpoint feeling during the Lachman test. In the intact porcine knees, the mean frequency was 84.1 ± 9.4 Hz and the mean acoustic pressure was −40.5 ± 1.7 dB. The results for the porcine knees were similar to those for the healthy male knees. The Lachman peak sounds of the porcine knees with ACL and PCL deficiency were dispersed into four distinct groups, with center frequencies of around 40, 160, 450, and 1600. Significant differences in the Lachman peak sounds were found between the intact knees and each group of knees with ACL and PCL deficiency (
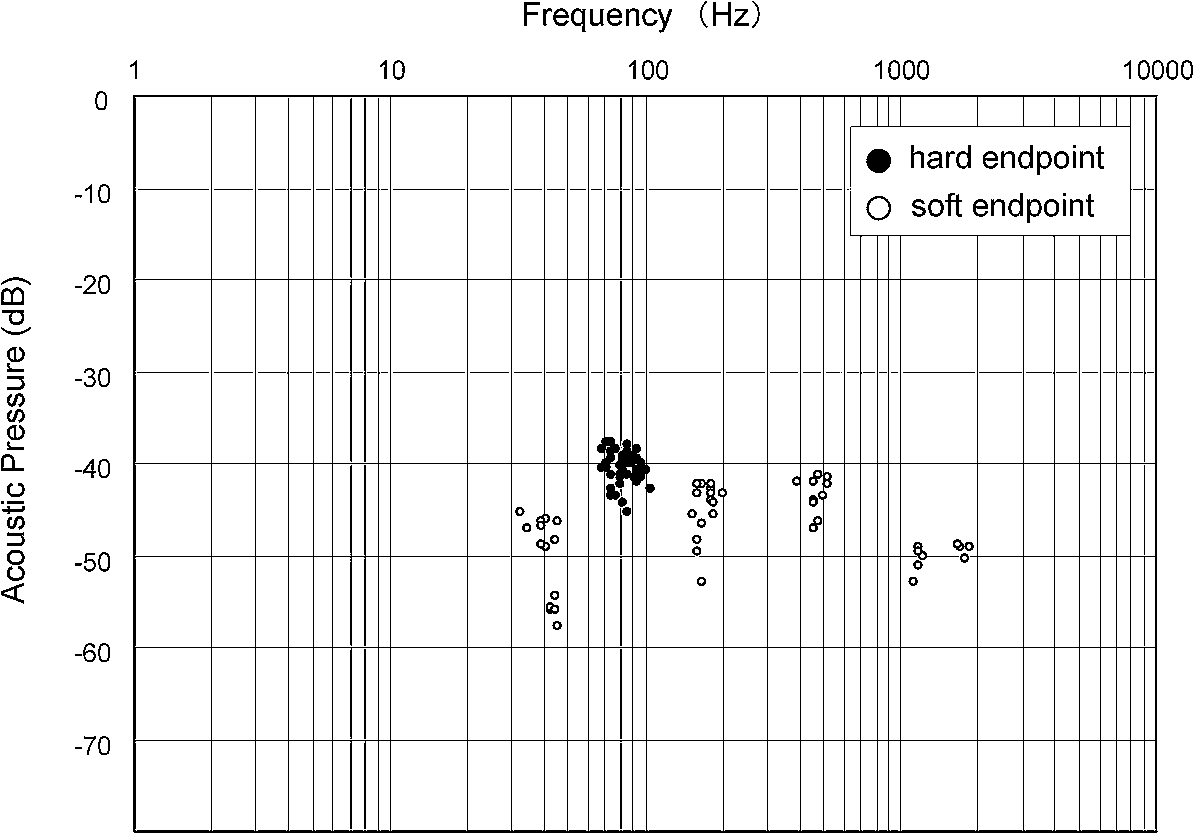
Acoustic distribution charts of the Lachman peak sound obtained from porcine knees with hard (filled circles) and soft (open circles) endpoints of the Lachman test.
The present study investigated knee joint sound during the Lachman test as Lachman sound. Using a contact microphone, ultrasound transmission gel, and Velcro tape, we were able to record and analyze the Lachman sound in a numerical manner. The main finding of the study was that the Lachman peak sound was capable of assessing soft and hard endpoints of the Lachman test objectively. In particular, the frequency of the Lachman peak sound was able to assess rupture of the ACL. Therefore, the joint auscultation system is promising as an endpoint judgment device to be used as supporting method of the Lachman test under any situation.
The Lachman test was first described by Torg et al. [5], who trained under Lachman at Temple University. Since then, the sensitivity and specificity of the Lachman test have been examined by many researchers. Originally, Torg et al. reported that the Lachman test was positive in 88 of 93 patients with ACL and medial meniscus injury [5]. The false-negative cases were attributed to bucket-handle meniscus tears that blocked forward translation of the tibia. Donaldson et al. described a sensitivity of >99% for this test and found it to be relatively unaffected by associated ligamentous or meniscal injuries [1]. The sensitivity of the Lachman test has been reported to range from 80–99% with a specificity of 95% [1–5,8]. Therefore, the Lachman test has been considered to be the most sensitive and specific test for diagnosis of ACL injury. The joint auscultation system should contribute to support the judgment of the Lachman test under any situation.
Several studies have assessed the endpoint quality of the Lachman test. Murase et al. reported that an accelerometer could evaluate the soft and hard endpoints in patients with ACL injury and healthy volunteers [9]. To judge the endpoint quality, they used the waveform pattern of the accelerometer during the Lachman test (i.e. spike waveform as a hard endpoint and sinusoidal waveform as a soft endpoint). However, the sensitivity and specificity were 81.0% and 98%, respectively. Therefore, it may be difficult to assess the endpoints of the Lachman test quantitatively using only waveform analysis. Kawaguchi et al. developed a fingertip pressure sensor and measured the pressure of the examiner’s fingertip during the Lachman test [10]. They revealed differences in the finger tip pressure between the soft and hard endpoints. However, the wide variety of examiners’ grip configurations and test styles could cause differences in the fingertip pressure. As a result, comparisons among examiners might be difficult using measurements of finger tip pressure. Our method using the joint auscultation system is hardly influenced by examiners’ grip configurations and test styles. Although the study was not sufficiently ongoing, it produced reproducible results. Further studies are needed to evaluate the intraexaminer and interexaminer reliability of Lachman sound analysis.
Auscultation is one of the most ancient methods for diagnosis. According to the paper by Steindler [11], the first application of auscultation for knee joint disease was reported by Hueter in 1885. He used auscultation to localize loose bodies in knee joints. Erb introduced modern instruments for auscultation of joint disease, in that he listened to minimized extraneous sounds using a contact microphone [12]. Steindler studied 397 knee joint sounds using a cardiophone, an oscilloscope, and a recorder [11]. He identified articular cartilage degeneration throughout a range of motion in the knee joint, but noted difficulty in distinguishing articular sounds from extrinsic sounds such as snapping tendons and noise from hand tremors while holding the cardiophone. Chu et al. analyzed the frequency spectrum of knee joint sounds and revealed different spectral patterns among normal, osteoarthritic, and rheumatoid arthritic knees [13]. They used a surgical lubricant on the skin surface to effectively eliminate skin friction noises caused by microphone motions on the knee during active motion. However, to the best of our knowledge, there have been no reports of applying knee joint auscultation for diagnosis of ACL injury. We utilized knee joint auscultation for assessment of the Lachman test and elucidated differences between the soft and hard endpoints of the Lachman test as differences in the frequency of the Lachman peak sound. Further clinical research on assessment of the ACL using knee joint auscultation is now required.
Based on the findings for the porcine knee joint auscultation, the Lachman peak sound for the hard endpoint was around 90 Hz, while those for the soft endpoint were around 40, 160, 480, and 1200 Hz. Therefore, Lachman peak sound of 90 Hz represented the hard endpoint feeling during the Lachman test. Indeed, the data for healthy human volunteer knees were similar to those for intact porcine knees. However, it is not known why Lachman peak sounds with different frequencies existed during the Lachman test with the soft endpoint. Biomechanically, Butler et al. revealed primary and secondary restraints to anterior tibial translation [14]. They determined that the ACL provides 86% of the total resisting force and that other ligaments, cartilage, and capsular structures provide the remaining secondary restraint. Therefore, differences in the main secondary restraint may cause the variety of Lachman peak sounds with different frequencies.
Two limitations of our study should be considered. First, this study was performed on healthy male volunteer and porcine knees, and the Lachman peak sound will therefore differ somewhat from the Lachman peak sound of patients with ACL injury. We are currently evaluating the Lachman sound of patients with ACL injury. In a preliminary study, we evaluated the Lachman sound of male patients with ACL deficiency (Fig. 5). The frequency of the Lachman peak sound was 323–378 Hz in knees with ACL deficiency compared with 79–86 Hz in the opposite healthy knees. Second, the frequency of the Lachman peak sound could detect differences in the soft and hard endpoints of the Lachman test, but Lachman sound may have more information about the ACL condition. According to Mersenne’s laws, the frequency of stretched strings is defined by the length, the force and the density. Therefore, the frequency of Lachman sound may be involved in an information of biomechanical property of ACL and further studies are required to determine whether knee joint auscultation will prove beneficial for ACL injury and reconstruction.
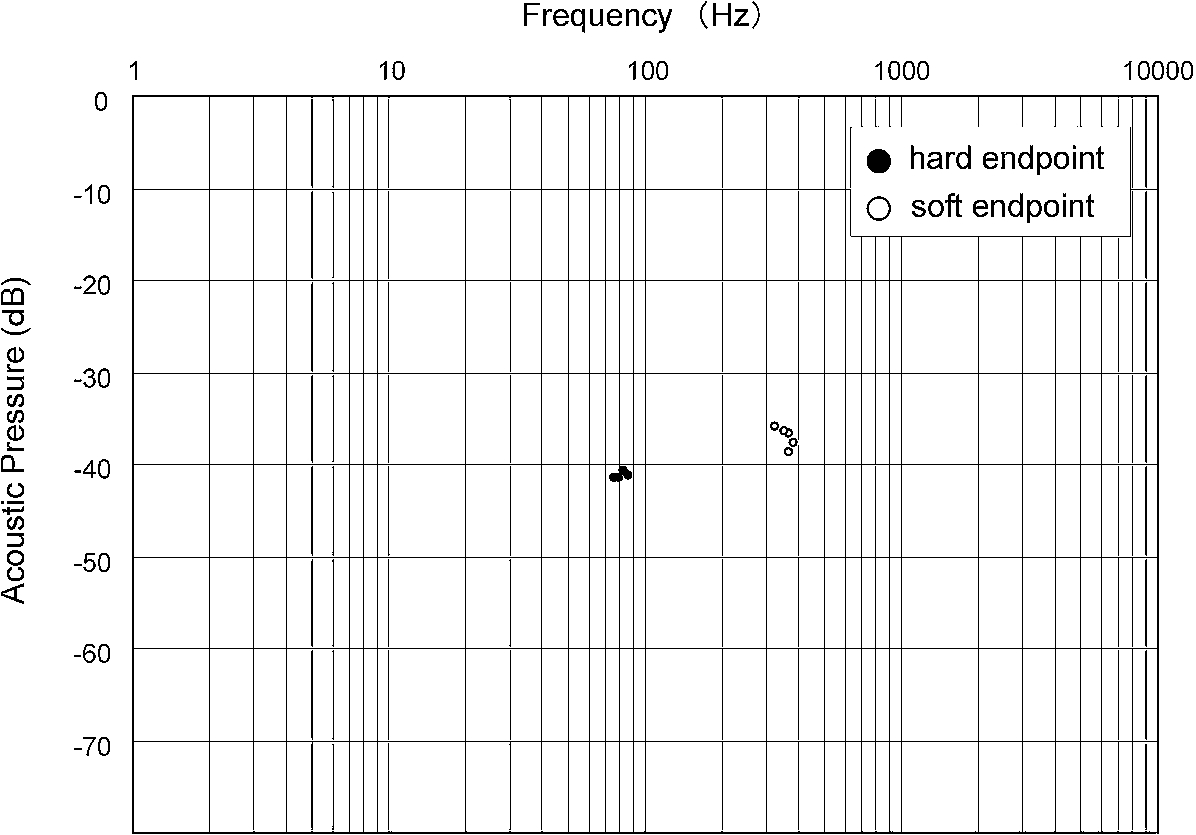
Case of a 35-year-old male. He sprained his left knee playing football 2 years previously, and presented to our hospital. MRI and arthroscopy demonstrated a partial tear of the medial meniscus and complete rupture of the ACL. A partial medical meniscectomy was performed under arthroscopy. However, ACL reconstruction was not performed and a conservative therapy was selected. Currently, he presents a soft endpoint for the left knee during the Lachman test. The acoustic distribution charts show differences in the Lachman peak sound for the hard endpoint (filled circles) of the healthy right knee and the soft endpoint (open circles) of the left knee with ACL deficiency.
In conclusion, knee joint sound can assess soft and hard endpoints of the Lachman test. The knee joint auscultation system can be used as a supporting method of the Lachman test. Combined with arthrometer, examiner can evaluate the degree of tibial anterior translation and the endpoint feeling of movement quantitatively. The knee joint auscultation system may contribute to progress in ACL treatment and Lachman sound can be expected to become one of supporting methods for the judgement of the Lachman test.
Conflict of interest
No potential conflicts of interest are declared.