
Abstract
Orthodontic tunnel miniscrews with and without TiO2 nanotube arrays were fabricated to improve the induction of new bone formation and osseointegration. To inject the drug of recombinant human bone morphogenetic protein, tunnels in a conventional machined miniscrew were machined by a computer-numerical-control lathe. TiO2 nanotube arrays to load the drug were also formed on the surface of the tunnel miniscrew by anodic oxidation. To obtain clean TiO2 nanotube arrays, two-step anodic oxidation was conducted. The diameters of TiO2 nanotube window and TiO2 nanotube were ∼70 nm and ∼110 nm, respectively. Three groups, i.e., a conventional machined miniscrew, a tunnel miniscrew without TiO2 nanotube arrays, and a tunnel miniscrew with TiO2 nanotube arrays, were prepared and inserted in the legs of five New Zealand White rabbits. In a histomorphometric analysis, the bone implant contact ratios of the tunnel miniscrews with the TiO2 nanotube arrays and without the TiO2 nanotube arrays were 5.84% and 5.88%, respectively. These values were higher than the value of 4.30% for the conventional machined miniscrew. The bone surface ratios in the tunnel miniscrew with and without the TiO2 nanotube were also higher than those of the conventional machined miniscrew. The measured values of the tunnel miniscrew with and without the nanotube and the conventional miniscrew were 76.75%, 73.41%, and 44.82%, respectively, although the differences were statistically insignificant. New bone at three weeks and six weeks after the operations were found in the tunnel miniscrews in fluorescent images. Both the tunnel miniscrews with and without the TiO2 nanotube arrays demonstrated greater bone formation compared to the conventional miniscrews. However, TiO2 nanotube arrays was not likely to provide additional benefit to the tunnel miniscrew. An in vivo study suggested that the tunnel fabricated in the miniscrew can be efficient drug-delivery systems to improve osseointegration.
Introduction
The development of materials and technology has been one of the most important contributions to dentistry. Various dental materials and appliances have also been introduced to improve the efficiency, accuracy, and convenience of diagnoses and treatments in the field of orthodontics and dentofacial orthopedics. Orthodontic tooth movement basically follows Newton’s third law, stating that for every action there is an equal and opposite reaction. The reaction part, which must be able to resist the force of tooth movement, is known as an anchor unit. Loss of anchorage has been one of the most fundamental problems in conventional orthodontics. The introduction of skeletal anchorages such as miniscrews which are placed into the bone provide an absolute anchorage for orthodontic [1,2] and orthopedic treatments [3].
However, the most common problems when using orthodontic miniscrews involve the loosening and mobility of the miniscrews during the treatment period. In a systematic review of the survival and failure rates of orthodontic miniscrews, the failure rate was estimated to be 16.4% (95% CI 13.4%–20.1%) in a meta-analysis [4]. Unlike an endosseous dental implant that osseointegrates, orthodontic miniscrews achieve stability primarily through mechanical retention. Many previous studies have investigated the factors which affect the stability of orthodontic miniscrews; the diameters, lengths, shapes and designs of miniscrews, the insertion angles, the methods of operation, and the quality of the bone are known to be related to the stability of the miniscrews used [5–7]. Improvements in the designs of miniscrews contribute to their initial stability immediately after the insertion of the miniscrew. However, some miniscrews have shown a decrease in stability during an orthodontic treatment [8], despite the fact that the initial stability was good. In addition to the mechanical aspects, biological problems with regard to poor bone quality, such as thin cortical bone and low bone density in some patients, still remain to be overcome.
Bone morphogenetic proteins (BMPs), proteins within the transforming growth factor beta (TGF-β), play a role in the differentiation, proliferation, growth inhibition and arrest of maturation of a wide variety of cells [9]. Some studies have evaluated the effect of recombinant human BMP-2 (rhBMP-2) and reported that rhBMP-2-coated titanium implants induced new bone formation and osseointegration [10,11]. These studies showed the possibility of a prosthetic implant as a drug carrier. In this case, a porous surface of the implant, such as anodic TiO2 nanotubes, can be a good drug-delivery system [12]. Some researchers evaluated TiO2 nanotubes on dental implants for the purpose of serving as a BMP-2-carrier in vitro [13]. However, to the best of our knowledge, there have been few studies of the biological effects of TiO2 nanotubes as a drug carrier with regard to orthodontic miniscrews in vitro or in vivo. Recently, Karmarker et al. [14] reported the effect of anodized orthodontic miniscrews in an animal study, but their study focused only on the effect of anodization for early-phase mechanical retention capability.
To improve the induction of new bone formation and osseointegration, we newly designed a tunnel miniscrew for which the tunnel is used to inject drugs or bone cement. The tunnel miniscrew can also control the rhythm and dosage of the drug and deliver the drug repeatedly, as the tunnel is connected from the outside of the miniscrew to the bone. The tunnels, which are opened on the surfaces of the middle part of the miniscrew, may also provide space for the formation of new bone. The bone growth factor of rhBMP-2 was selected as a drug in this study. To load rhBMP-2 on the surface of the tunnel miniscrew, TiO2 nanotube arrays on the surface of the tunnel miniscrew were fabricated by anodic oxidation [15–20]. These components may serve as small reservoirs for the drug. The effects of the tunnel and the TiO2 nanotube arrays on new bone formation and osseointegration were characterized. The possibility of a drug-delivery system of tunnel miniscrews is demonstrated by an in vivo test.
Experimental details
Fabrication of tunnel and TiO2 nanotube arrays on orthodontic miniscrews
The samples were composed of one control group and two experimental groups. A conventional machined surface miniscrew (Dual-top JA, Jeil Medical, Korea), which is a screw-shaped titanium implant, was selected as the control group (CM group,
To fabricate the TM group with a tunnel on orthodontic miniscrews, the machined surface miniscrews of the control group were machined by a computer numerical control (CNC) lathe. Figure 1 shows the design of the machined tunnel miniscrew. The length of the tunnel miniscrews is 10 mm in Fig. 1(b). Figure 1(c) and (d) depict X–X’ and Y–Y’ cross-sectional views, respectively. The tunnel miniscrews have one vertical hole with a diameter of 0.5 mm at the center of the cylinder shape screw and two unilateral horizontal holes with a diameter of 0.5 mm perpendicular to the vertical hole through which the rhBMP-2 solution is injected.
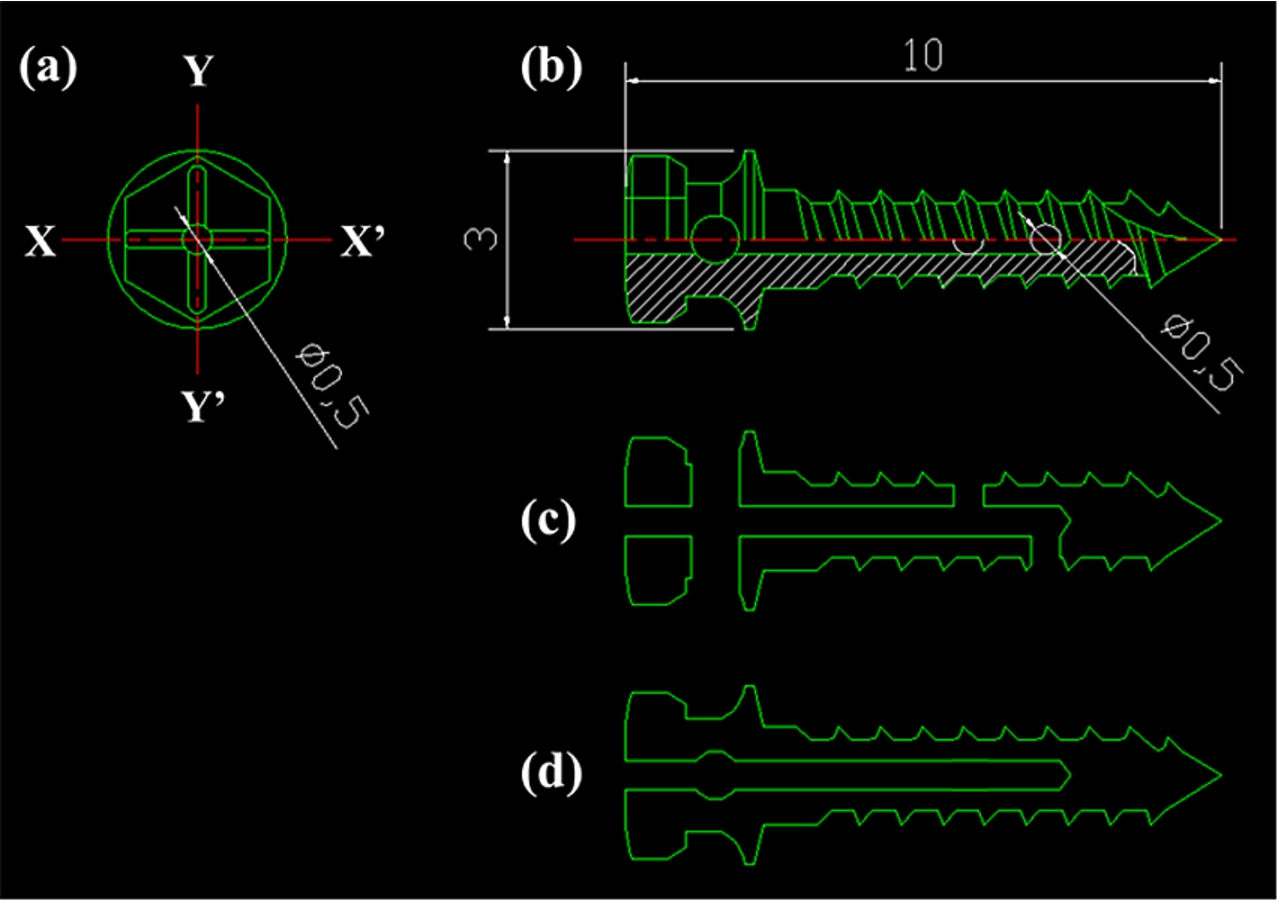
The design of the tunnel miniscrew for machining: (a) top view, (b) side view, (c) X–X’ cross-sectional view, and (d) Y–Y’ cross-sectional view.
To load the rhBMP-2 on the surface of the tunnel miniscrew, TiO2 nanotube arrays on the surfaces of the tunnel miniscrews were designed. The TM group was anodized to create the TiO2 nanotube arrays under various anodic oxidation voltages applied through a DC power supply in an electrolyte solution containing ethylene glycol with 0.5 wt% NH4F. Figure 2 shows a schematic diagram of the anodic oxidation. Two-step anodic oxidation was conducted to obtain a clean surface and open windows of the TiO2 nanotube arrays. The tunnel miniscrew was initially anodized at a voltage of 60 V and a time of 1 hr. The TiO2 nanotube arrays fabricated during the first anodic oxidation step were removed by ultrasonication. Then, the TiO2 nanotube arrays with the clean and open windows were formed by a second anodic oxidation step. The voltage and time of the second anodic oxidation step were 15 V and 15 min, respectively. The TNM group with the TiO2 nanotube arrays on the surface of the tunnel miniscrews was then fabricated. Before the TNMs were inserted into the bone, the rhBMP-2 (Cowellmedi Co., Busan, Korea) was loaded into the inner space of the TiO2 nanotube arrays on the surface of tunnel miniscrew by a dip coating process in a vacuum chamber. Each miniscrew was immersed three times in rhBMP-2 solution for 5 seconds and dried at a maximum of 20°C. The concentration of the rhBMP-2 solution was 1.5 mg/ml. The microstructure of the TNM group was observed by FESEM.
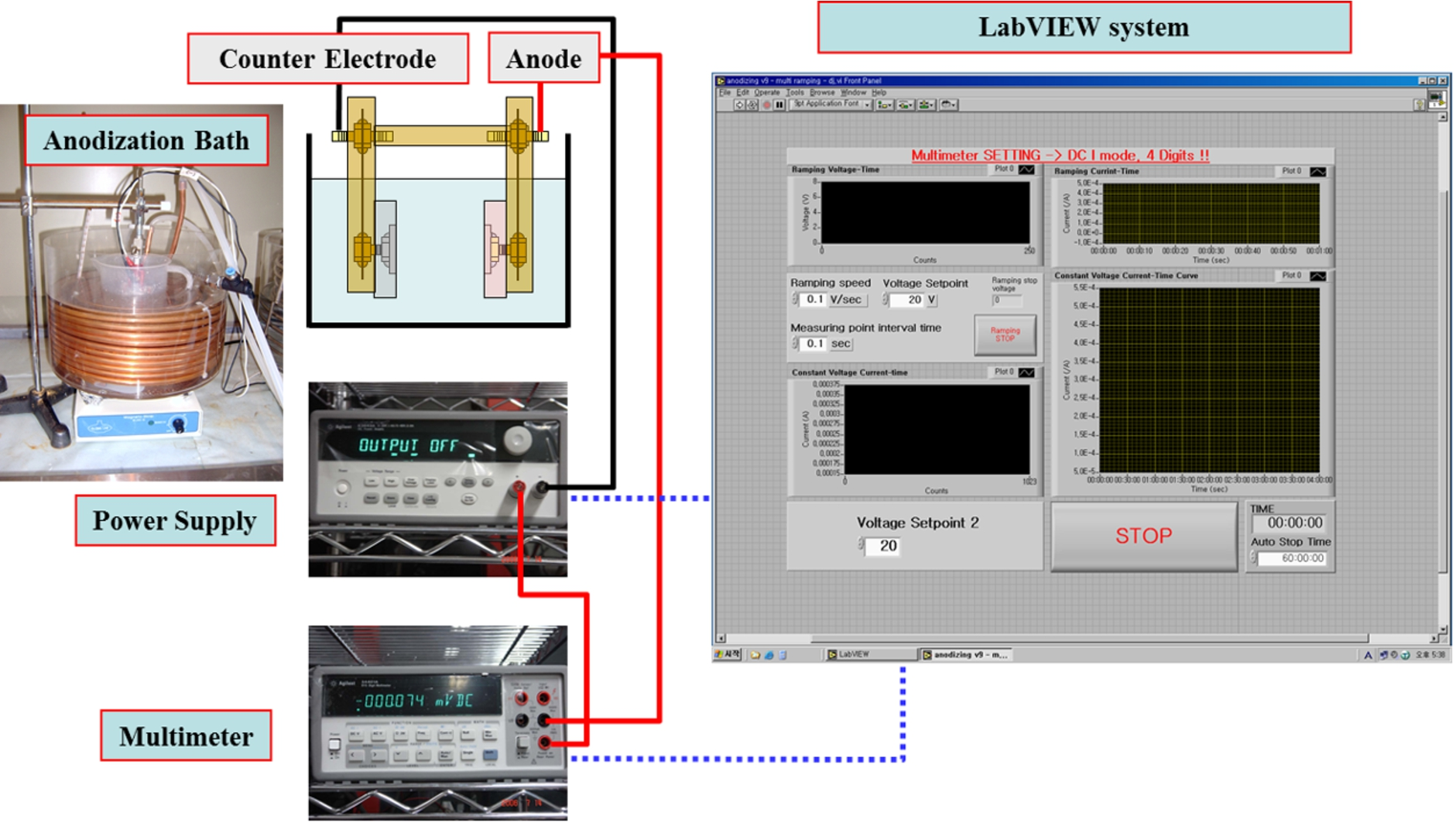
Schematic diagram of the anodic oxidation process.
The treatment of experimental animals for this study was approved by the Institutional Experimental Animal Committee of Gangneung-Wonju National University (GWNU-2013-3). Five New Zealand White rabbits (body weight,
All animals were sacrificed in a CO2 chamber at 8 weeks after the operation and 1 cm × 1 cm bone fragments with miniscrews were collected. The bone fragments were subsequently fixed with 10% formalin. The bone fragments were scanned at a 6 µm resolution using a micro-CT device (Skyscan 1173, Skyscan, Kontich, Belgium). In the 3D images, the bone volume ratio (%) and the bone surface ratio (%) were quantitatively calculated around three threads in the cancellous bone area. Then, after dehydration with an ethanol solution, embedding in methyl methacrylate resin, and polymerization, the miniscrews were cut and ground to approximately 30 µm in thickness (Kulzer EXAKT 400CS, Germany). All sections were examined by immunofluorescence microscopy (Leica Microsystems, Wetzlar, Germany) and the specimens were stained by Goldner’s trichrome and examined by optical microscopy (BX51, Olympus, Japan). The bone-to-implant contact ratio (BIC, %) and the new bone area ratio (NBA, %) values were also calculated in the section images using imaging analysis software (Media Cybernetics, Inc., USA). All examinations were performed by one investigator who did not know the aims of this study.
Statistical analysis
The data were analyzed using non-parametric method because of small sample size. A Kruskal–Wallis Test was used to verify the difference among the groups. Statistical significance was determined at the 5% level of confidence. All statistical analyses were performed with software (version 18.0; SPSS, Chicago, IL).
Results and discussion
Figure 3 shows FESEM images of the miniscrews of the CM and TM groups. The images of the miniscrew for the CM group showed the typical machined surface images of a titanium implant. To inject the rhBMP-2 solution, vertical and horizontal holes were fabricated by a CNC lathe. The horizontal hole is shown in Fig. 3(c). The diameter of the horizontal hole was 0.5 mm. The images of TM group miniscrews were also identical to those of the CM group with a conventional machined surface.

FESEM images of the miniscrews of CM group and TM groups: (a) low-magnification image (×35) of the CM group miniscrew, (b) high-magnification image (×2,500) of the CM group miniscrew, (c) low-magnification image (×30) of the TM group miniscrew, and (d) high-magnification image (×10,000) of the TM group miniscrew.

FESEM images of TiO2 nanotube arrays on the surface of a TNM group miniscrew: (a) low-magnification image (×20,000) of TiO2 nanotube arrays, (b) high-magnification image (×50,000) of TiO2 nanotube arrays, (c) low-magnification image (×10,000) of rhBMP-2-loaded TiO2 nanotube arrays, and (d) high-magnification image (×30,000) of rhBMP-2-loaded onto the TiO2 nanotube arrays.
Figure 4 shows FESEM images of the TiO2 nanotube arrays on the surface of a TNM group miniscrew. The TiO2 nanotube arrays were fabricated by means of two-step anodic oxidation. The traces of TiO2 nanotube arrays by the first anodic oxidation step are shown on the surfaces of the newly grown TiO2 nanotube arrays. The diameters of the TiO2 nanotube window and TiO2 nanotube were ∼70 nm and ∼110 nm, respectively. The length of the TiO2 nanotube arrays was ∼10 µm. The rhBMP-2 loaded into the TiO2 nanotube in the TNM group miniscrew is shown in Fig. 4(c) and (d). The window of the TiO2 nanotube, as shown in Fig. 4(d), was slightly clogged due to rhBMP-2 loading. The diameter of TiO2 nanotube window was decreased to ∼50 nm. This suggests that rhBMP-2 might be loaded into the TiO2 nanotube. Similar figures in dental implant were reported in our previous work [21]. The study has already shown the results of detecting rhBMP-2 by the interferometric biosensing methods [16,21]. In the previous study, the optical thickness was changed with elution of rhBMP-2 from TiO2 nanotube arrays in flow cell test kit. The optical thickness of rhBMP-2 loaded TiO2 nanotube arrays was ∼75 nm higher than that of unloaded TiO2 nanotube arrays and the value was sustained for 9 days. It meant that rhBMP-2 was successfully loaded and released from TiO2 nanotube arrays. In the present study, the rhBMP-2 was expected to be slowly released from the TiO2 nanotube of the miniscrew, because rhBMP-2 loaded TiO2 nanotube arrays in miniscrew was almost same as the previous our work [21]. However, both the result of the interferometric test and FESEM images are not sufficient to prove the amount of the rhBMP-2 in the TiO2 nanotube arrays. Therefore, a future study for quantitative evaluation on the amount of drugs which would be loaded in the TiO2 nanotube arrays is necessary.

Microscopic images of the miniscrews of the three groups inserted into the femurs of the rabbits: (a) CM group, (b) TM group, and (c) TNM group.

Micro-CT images of the miniscrews of the three groups inserted in the femurs of the rabbits: (a) CM group, (b) TM group, and (c) TNM group.
Figures 5 and 6 depict microscopic and micro-CT images of the miniscrews of the three groups which were inserted in the femurs of the rabbits. All miniscrews were successfully implanted into the bones. More trabecular patterns were observed in the TNM group than in the CM group and the TM group. Figures 7 and 8 show microscopic images of the miniscrews in the three groups which were inserted in the tibias of the rabbits. The tibia showed less of a trabecular pattern in cancellous bone than did the femur; however, the TNM group showed more trabecular bone around middle third of the screw than did CM and TM groups. In fact, the femur and tibia of the rabbit rarely have trabecular bone in the cancellous bone area, while there is dense and sufficient bone in the cortical bone area. Therefore, previous studies observed mechanical interlocking between the bone and the implant (or miniscrew) in the cortical bone area [11]. However, the area of interest in the present study was the cancellous bone area, as the aim of our study was to test the possibility of drug delivery through the tunnels which were opened in the middle third of the miniscrew. There would be different results in a histomorphometric analysis of the groups if rhBMP-2 was successfully injected through the tunnels of the miniscrews and osteoinduction subsequently occurred.

Microscopic images of the miniscrews of the three groups inserted in the tibias of the rabbits: (a) CM group, (b) TM group, and (c) TNM group.

Micro-CT images of the miniscrews of the three groups inserted in the tibias of the rabbits: (a) CM group, (b) TM group, and (c) TNM group.
Figure 9 and Table 1 show the results according to a histomorphometric analysis of the cancellous bone area. The TM group (5.88%) and the TNM group (5.84%) showed higher BIC levels than the CM group (4.30%). New bone area (NBA, %) around the middle third of the miniscrew was the highest in the TM group (9.41%), followed by the TNM group (4.60%), whereas new bone formation was not found in the CM group (0%). However, the differences among the groups were not statistically significant. Table 2 shows the results as evaluated by the 3D micro-CT images. The bone volume ratios measured in the middle third of the miniscrew were higher in the TM group (11.57%) and the TNM group (11.35%) than in the CM group (8.00%). The bone surface ratios were also higher in the TM group (73.41%) and the TNM group (76.75%) than in the CM group (44.82%). Overall, the amount of bone around the miniscrews was greater in the TM group and the TNM group than in the CM group. However the differences did not also show the statistical significance. An increase in the sample size may be necessary for statistically significant results.

Histomorphometric analysis in the middle third of the miniscrew in the cancellous bone area: (a) bone implant contact ratio, and (b) new bone area ratio.
Summarized data of histomorphometric analysis in the cancellous bone area
Kruskal–Wallis test. BIC, bone to implant contact ratio; NBA, new bone area ratio.
Micro-CT analysis in the cancellous bone area
Kruskal–Wallis test. TV, tissue volume; BV, bone volume; TS, tissue surface; BS, bone surface.
Figure 10 shows fluorescent images taken at the middle third of the miniscrews in the three groups. The bone images dyed in red and green represent new bone which formed at 3 weeks and 6 weeks after the insertion of the miniscrews, respectively. The arrows show the new bone. Distinct bone layers were observed through the surface of the miniscrews in TM and TNM groups, whereas no bone was found in the control group. As mentioned above, rabbits have little cancellous bone in both the femur and tibia. Therefore, the new bone in the TM and TNM group can be evidence of osteoinduction by rhBMP-2, meaning that the vertical and horizontal holes built into the miniscrews were efficient for delivering some of the drugs into the bone. It is interesting that the TM and TNM groups still had the osteoinduction effects of rhBMP-2 at 6 weeks after the operation.
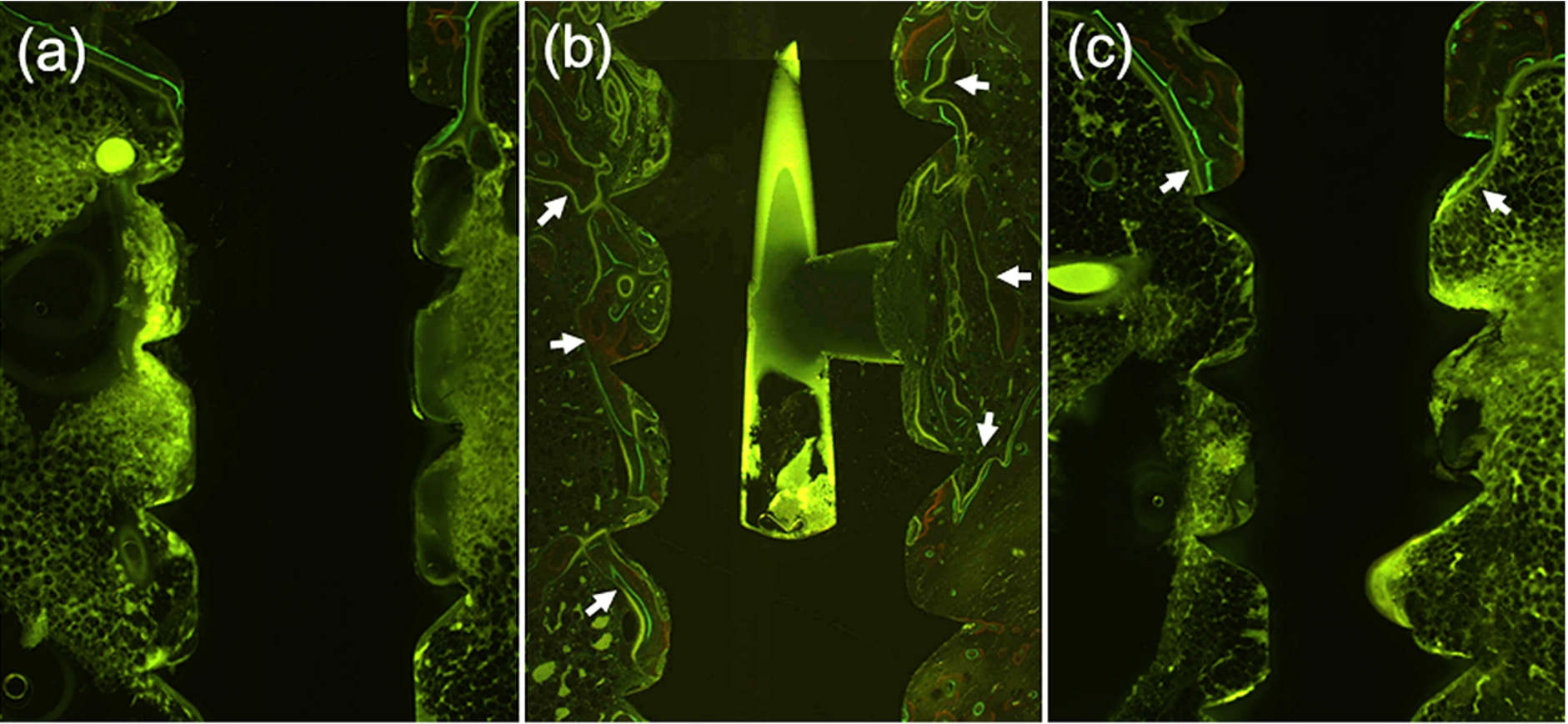
Fluorescent images observed at the middle third of the miniscrews of the three groups: (a) CM group, (b) TM group, (c) and TNM group.
There have been some reports of bone formation and cell adhesion effects of titanium anodization implants without drugs [19,22,23]. Von Wilmowsky et al. [19] investigated bone formation with various diameters of anodic TiO2 nanotubes ranging from 15 nm to 100 nm and reported that a significantly higher BIC could be found for groups with diameters of 50, 70, and 100 nm compared to controls, implying that the nanotube diameter can be designed to support the cellular functions of osteoblasts and osteoclasts. Karmarker et al. [14] also reported that anodized orthodontic miniscrews showed greater peak removal torque in rabbits, even when bio-chemical therapy was not applied. In the present study, it is unclear whether the greater BIC, NBA, BV/TV ratio, and BS/TS ratio in the TNM group resulted from the effect of rhBMP-2 or from anodization. However, it is certain that rhBMP-2 was successfully delivered onto the bone-to-miniscrew surface by an injection from the outside to the middle part of the miniscrew through the tunnels, as shown in Fig. 10(b), as TM group showed no effect of TiO2 anodization, which is known to enhance cell adhesion.
Caliskan et al. [22] tested the possibility of implant anodization as a drug reservoir and reported that the elution of bactericidal agents lasted up to 4 days. The diameter and length of the nanotube for some drugs should most likely vary, as the optimal dosages and releasing times are different depending on the drugs. Although an improvement in the microstructures of the nanotube as a drug carrier can increase and control the releasing time, tunnels may be a more direct approach to control the dosage. In addition, tunnel miniscrews with a TiO2 nanotube array can serve as a new drug-delivery system which supplies some drugs repeatedly from outside to an inner drug reservoir, like nanotubes. The microstructures of the nanotube should be sound during and after drilling to the bone. According to a study by Choi et al. [24], the middle thread edge of the anodic oxidized miniscrews was still rougher than the machined surface miniscrews, although the surface texture of the thread edge close to the tip of the miniscrew became smooth due to the self-drilling procedure.
This drug-delivery system including tunnels and TiO2 nanotube arrays may also be used for other drug purposes, such as for the delivery of antibiotics and anti-inflammatory drugs, which should be delivered to the local area within the bone for treatment of chronic osteomyelitis, osteitis, and bone cancers. However, there is little information on the optimal diameters and lengths of the nanotubes for the various drugs or the optimal amounts and dosages of rhBMP-2 for use with an orthodontic tunnel miniscrew. In the future, study of the optimal amount and rhythm of rhBMP-2 for maximum bone formation is necessary, and more convenient devices to deliver a drug through the tunnel of the miniscrew or an implant, especially without a loss of high-cost drugs, should be developed. Moreover, the viscosity of the drugs [25] and the possibility of the fracture of the tunnel miniscrew [26] should be considered.
Tunnel miniscrews have been newly designed and fabricated with and without TiO2 nanotube arrays. The tunnel and TiO2 nanotube arrays in the miniscrews developed here successfully delivered the rhBMP-2 bone growth factor. In an animal study, the bone surface ratios of the tunnel miniscrews with and without the TiO2 nanotube arrays were 76.75% and 73.41%, respectively. These values are higher than the value of 44.82% for a conventional miniscrew without tunnel or a TiO2 nanotube arrays, although the differences were statistically insignificant. The amounts of new bone around the tunnel miniscrews were also greater than that around a conventional miniscrew. Both tunnel miniscrews with and without TiO2 nanotube arrays improved the bone formation performance. However, TiO2 nanotube arrays was not likely to provide additional benefit to the tunnel miniscrew. An in vivo study suggested that the tunnel fabricated in the miniscrew can be efficient drug-delivery systems to improve osseointegration.
Footnotes
Acknowledgements
This research was financially supported by the Human Resource Training Program for Regional Innovation and Creativity, through the Ministry of Education and the National Research Foundation of Korea (Grant No. 2015H1C1A1035848).
Conflict of interest
The authors have no conflict of interest to report.