
Abstract
The relevance of research on reconstructed organs is justified by the lack of organs available for transplant and the growing needs for the ageing population. The development of a reconstructed organ involves two parallel complementary steps: de-cellularization of the organ with the need to maintain the structural integrity of the extracellular matrix and vascular network and re-cellularization of the scaffold with stem cells or resident cells.
Whole organ engineering for liver, heart, lung or kidneys, is particularly difficult because of the structural complexity of organs and heterogeneity of cells. Rodent, porcine and rhesus monkey organs have been de-cellularized to obtain a scaffold with preserved extracellular matrix and vascular network. As concern the cells for re-cellularization, embryonic, foetal, adult, progenitor stem cells and also iPS have been proposed.
Heart construction could be an alternative option for the treatment of cardiac insufficiency. It is based on the use of an extra-cellular matrix coming from an animal’s heart and seeded with cells likely to reconstruct a normal cardiac function. Though de-cellularization techniques now seem controlled, the issues posed by the selection of cells capable of generating the various components of cardiac tissue are not settled yet. In addition, the recolonisation of the matrix does not only depend on the phenotype of cells that are used, but it is also impacted by the nature of biochemical signals emitted.
Recent researches have shown that it is possible to use decellularized whole liver treated by detergents as scaffold, which keeps the entire network of blood vessels and the integrated extracellular matrix (ECM). Beside of decellularized whole organ scaffold seeding cells selected to repopulate a decellularized liver scaffold are critical for the function of the bioengineered liver. At present, potential cell sources are hepatocyte, and mesenchymal stem cells.
Pulmonary regeneration using engineering approaches is complex. In fact, several types of local progenitor cells that contribute to cell repair have been described at different levels of the respiratory tract. Moving towards the alveoles, one finds bronchioalveolar stem cells as well as epithelial cells and pneumocytes. A promising option to increase the donor organ pool is to use allogeneic or xenogeneic decellularized lungs as a scaffold to engineer functional lung tissue ex vivo.
The kidney is certainly one of the most difficult organs to reconstruct due to its complex nature and the heterogeneous nature of the cells. There is relatively little research on auto-construction, and experiments have been performed on rats, pigs and monkeys.
Nevertheless, before these therapeutic approaches can be applied in clinical practice, many researches are necessary to understand and in particular the behaviour of cells on the decellularized organs as well as the mechanisms of their interaction with the microenvironment. Current knowledges allow optimism for the future but definitive answers can only be given after long term animal studies and controlled clinical studies.
Introduction
The relevance of research on reconstructed organs is justified by the lack of organs available for transplant and the growing needs for an ageing population [1]. On a technical level, the development of these reconstructed organs involves two parallel complementary stages: de-cellularization of the organ with a need to maintain the structural integrity of the extracellular matrix and re-cellularization of the matrix with stem cells or resident cells [2].
Whole organ engineering like liver heart, lung or kidneys, is particularly difficult because of the structural complexity and heterogeneity of organ cell types. But new ways of researches are currently focused on: the matrix to support re-cellularization and a promising approach is the direct use of extracellular matrix of the organ. Thus rodent, porcine and rhesus monkey organs have been de-cellularized to obtain a scaffold with preserved extracellular matrix and vascular bed. As concern the source of cells for re-cellularization embryonic, foetal, adult, progenitor stem cells and also iPS have been proposed.
Decellularization can be achieved through an intra-arterial infusion of a solution containing TritonX-100 and ammonium hydroxide. This method causes all the cellular elements to disappear, leaving elements of the extracellular matrix and the vascular system. Other methods of decellularization have also been used, employing other chemical, enzymes or physical agents (ultrasound) [3].
Several types of cell can be considered for re-cellularization. Stem cells probably represent the ideal source of material due to their ability to proliferate [4–6]. Their use appears limited, nevertheless, by their allogenic nature, which could possibly trigger an immune response and consequent rejection, in addition to the risk with embryonic stem cells of the formation of teratomes in vivo. These obstacles could be removed in future by using nuclear transfer techniques from the patient’s somatic cells (IPS) [7]. Finally, the stem or progenitor cells present in most organs are another source of cells that could be used for in vitro organogenesis. Considered as tools or repair material for their corresponding organs, they often remain difficult to define, isolate and to growth in culture. Furthermore, the type and number of cells to be used for re-cellularization vary depending on the organ to be reconstructed. Apparently, specific cells of the organ to be reconstructed are indispensable. Other types of cell, such as endothelial cells and fibroblasts are also needed, since they promote the functional cell phenotype and contribute to the structural organisation of tissue. The matrix of the vascular system of the organ to be reconstructed needs to be re-endothelialized so as to orientate the blood flow and prevent thrombosis.
Currently, growing organs in vitro and ex vivo can take several weeks until they have completely developed in the matrix. The seeding methods for re-cellularization are inspired by those used in cell therapy and the most practical solution seems to be intra-arterial infusion. The use of an extra-corporeal pulsating or continuous infusion system (bioreactor) is indispensable for providing the cells with an oxygen supply and keeping the infusate at a constant temperature. The infusion liquids are derived from the culture media used for the cells in question. They need to contain growth factors or other molecules that are more specific to each organ. Finally, there is another hypothetical possibility for re-cellularization, the transplanting of a de-cellularized organ into the recipient, in the hope that re-cellularization will occur directly from the recipient’s own cells.
Encouraging work has recently shown the feasibility of creating bio-organs for the reconstruction of the liver, heart, lungs and kidneys. However, clinical applications still remain a distant prospect.
1. Heart. Heart construction could be an alternative choice for the treatment of cardiac insufficiency. It is based on the use of an extra-cellular matrix coming from an animal’s heart and seeded with cells able to reconstruct a normal cardiac function. Though de-cellularization techniques now seem controlled, the issues posed by the selection of the cells capable of generating the various components of cardiac tissue are not settled yet. In addition, the recolonisation of the matrix does not only depend on the phenotype of cells that are used, but it is also impacted by the nature of biochemical signals emitted. The complexity of those problems results in the full replacement of the heart with a biomaterial substitutes to standard transplanting is one prospect. However, it is more realistic to hope, in the medium run, partial replacements of the heart with cellularized matrices reinforcing portions of the failing myocardium or with direct cellular therapy with stem cells [8].
The de-cellularization of animal hearts (rats and, more recently, big mammals) has been performed through the infusion of chemical detergents [9]. The results show that the integrity of the matrix (collagen, fibronectin, laminin, fibre orientation, etc.) can be maintained as well as permeability of the vascular tree and the competence of the heart valves [10,11]. Re-cellularization is more problematic due to the diversity of the cell populations that need to be reconstituted. These are the cardiomyocytes, myofibroblasts, endothelial cells and the smooth muscle [12]. Ways to achieve this could be considered. In summary, the complete replacement of a human heart by another heart build from a matrix of animal origin and seeded by cells capable to provide the organ with effective, mechanical activity remains a remote prospect and is unlikely to become a reality within the next 10 to 20 years.
Another way is the preparation of cardiac patches. The construction of the high biocompatible biomaterials pre-treated with stem cells will offer a promising strategy to improve the effects of stem cell therapy for MI (myocardial infarction) [13]. Thus the development of this cardiac stem cell patch has high therapeutic perspectives for the treatment of MI and prevention of the chronic heart failure. However the materials suitable for the treatment of MI need to have specific quality: biocompatibility, resistant to the mechanical force in situ, suitable for the cell amplification, with suitable size of pores for the cell communication which is necessary for the formation of the functional tissue. Under microscope, the pore size needs to be at least 50 μm which is necessary for the vascularization of the patch and assure the cell metabolism. The biological materials have more advantages than artificial materials because of the optimal cell integration for the construction of the cardiac stem cell patch. As the mesenchymal stem cells derived from the Wharton Jelly of umbilical cord are easy to be collected, the umbilical artery can be collected preferable at the same time. The natural matrix of the umbilical artery possesses the properties for the construction of a biocompatible cardiac patch.
2. Liver. Recent researches have shown that it is possible to use decellularized whole liver treated by detergents as scaffold, which keeps the entire network of blood vessels and the integrated extracellular matrix (ECM) [14]. Decellularized liver keeps exactly the texture of the original organ. This natural structure can provide a 3-dimensional matrix in favour of cultures cell proliferation, differentiation and function, which promotes the emergence of the idea to use decellularized organ in bioengineering organ (Fig. 1). The liver decellularization is carried out by perfusing detergents like TritonX-100 and sodium dodecyl sulphate (SDS), through liver portal vein. This method can destroy cell membrane and take off debris of cells, and at the same time keep the extracellular matrix complete with blood and biliary vessels. This matrix maintains the liver-specific proteins proportions for collagens I and IV, fibronectin and laminin. The intact vasculard system is useful in recellularization.
Beside of decellularized whole organ scaffold seeding cells selected to repopulate a decellularized liver scaffold are critical to the function of the bioengineered liver. At present, potential cell sources are hepatocyte, and mesenchymal stem cells [15,16] or even Induced pluripotent stem cell-derived hepatocytes [17].
Recent studies have shown that MSC originated from extre-hepatic tissues can differentiate into endoderm cell-lines as hepatocytes [18]. Several methods have successfully differentiated MSC into hepatocyte, such as stimulating MSC by cytokines and growth factors, direct and indirect co-culture MSC with hepatocytes, or promote MSC differentiation by 3-dimensional matrix [19]. In some cases, differentiation of MSC into hepatocytes can also be an alternative approach for whole organ transplantation in treatment of acute and chronic liver diseases [6].
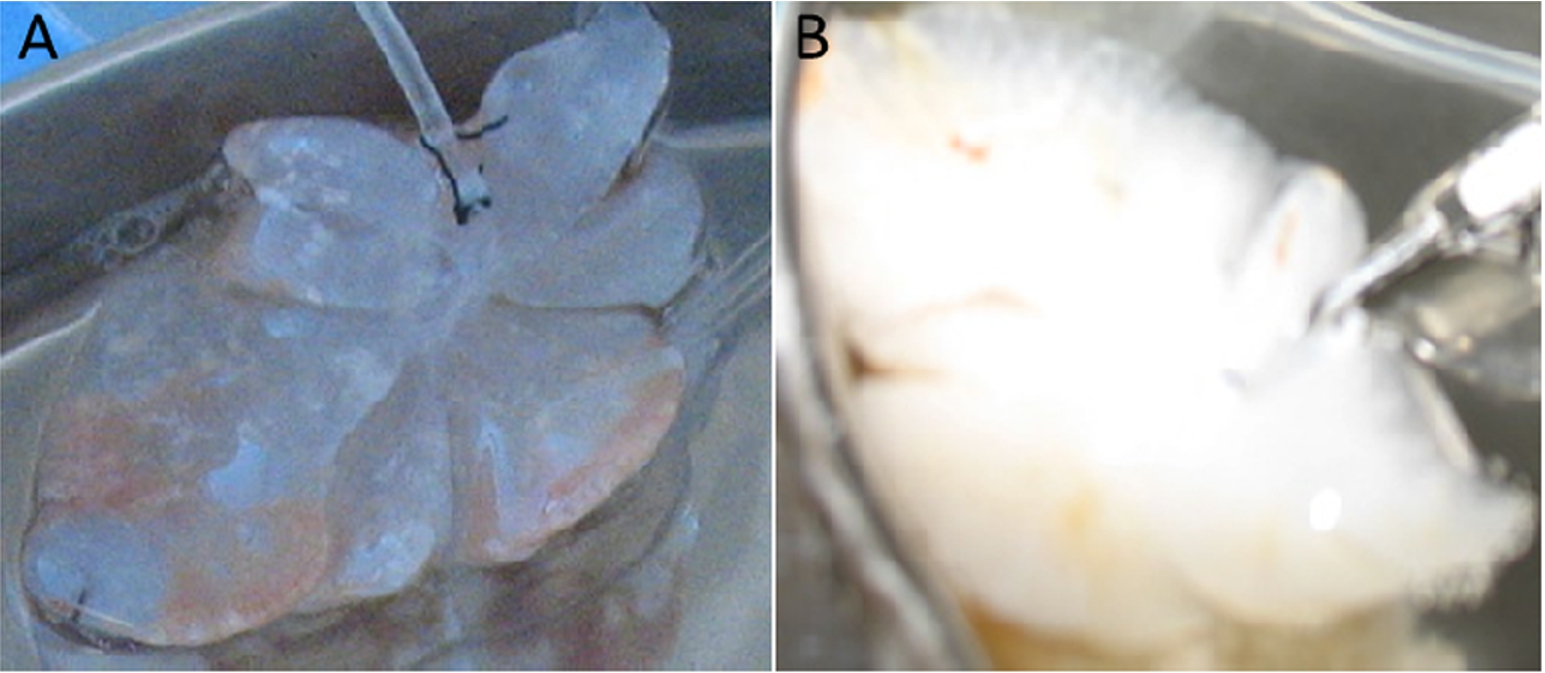
(A) Rat liver before decellularization; (B) after decellularization (from L. Zhang). [Work realized in the frame of the French–China CNRS-GDRI 0851.]
3. Lungs. About fifty million people throughout the world are living with chronic respiratory failure at a terminal stage. The only treatment for this condition which seriously reduces life expectancy is, in selected cases, lung transplants (first graft 1963) but the results remain poor [20,21].
A tracheobronchial graft remains a challenge [22]. Research has not yet found an ideal substitute for the airways. Failures have been observed with synthetic prostheses, bio-prostheses, tracheal allografts and autografts. In fact, not only epithelial tissue regeneration but also even cartilaginous regeneration has been observed. Research seems to indicate that this regeneration of tracheal tissue might be possible from an aortic matrix and stem cells taken from bone marrow [23]. Studies have been performed in humans in the context of extended cancer of the trachea and conservation surgery in cases of lung cancer. The research has also contributed prospects for understanding the tissue regeneration mechanisms.
Pulmonary regeneration using stem cells is complex [24]. In fact, several types of local progenitor cells that contribute to cell repair have been described at different levels of the respiratory tract. Moving towards the alveoles, one finds bronchioalveolar stem cells as well as epithelial cells and pneumocytes [25]. In the category of “local stem cells”, cells of the sub-population have been identified that are differentiation markers which in vitro mime stromal mesenchymal cells. The role of these cells in tissue repair has been demonstrated in animal models. Chistiakov et al. described resident, multipotent pulmonary stem cells that are capable of self-renewal as well as clonogenicity. The phenotype and functional characteristics of these new cells have been specified in vitro and in vivo. The lung also contains resident specific mesenchymal stem cells that have recently been described and characterised. These cells do not play a direct part in epithelial renewal but establish communication with the epithelium, thus ensuring their role as a local cytoprotector [26].
Finally, different studies performed on animals have shown the beneficial role played by exogenous, mesenchymal stem cells produced by bone marrow. The effects observed in lesional pulmonary œdema, sepsis, pulmonary hypertension and even idiopathic pulmonary fibrosis have resulted in clinical applications that are currently being assessed. The immuno-modulatory, anti-inflammatory, anti-apoptotic and angiogenic properties of MSC today place these cells at the heart of tissue repair. Contrary to past hypotheses, these cells do not seem to differentiate themselves into alveolar epithelial cells and their method of action would involve paracrine mechanisms not all of which have as yet been explained.
These initial researches open up a promising route for developing a functional bio-artificial lung, with the prospect of application to humans within 15 to 20 years [27]. However many questions remain to be answered: Is the use of a decellularized pulmonary matrix the only possible solution? Which cells should be chosen for recellularization? Mesenchymatous stem cells? Resident pulmonary cells? What is the optimal length of time for incubation in a bioreactor? Would the technique be applicable to the human lung with its very extensive alveolar surface?
4. Kidney. The kidney is certainly one of the most difficult organs to reconstruct due to its complex nature and the heterogeneous nature of the cells from which it is constituted [28]. There is relatively little research on kidney auto-construction though experiments that have been performed on rats, pigs and monkeys. The first demonstration of the feasibility of the approach was developed in the rat. A research team introduced extracellular matrices using embryonic stem cells injected into the renal artery or the ureter [29]. The cells introduced were differentiated into glomerular, tubular and vascular structures. They nevertheless lost their embryonic phenotype showed by the appearance of immuno-histochemical markers. Nakayama and his team decellularized sections of the kidneys taken from macaques at various growth stages, from foetus to adult, via intermediate ages, with the aim of optimising decellularization techniques and recellularization in vitro [30]. They compared different decellularization protocols and observed that sodium dodecyl sulfate at 4°C was the most effective in preserving the native architecture of the organ. Hematoxylin and eosin staining confirmed the removal of cellular material, and immunohistochemistry demonstrated preservation of native expression patterns of extracellular matrix proteins, including heparan sulfate proteoglycan, fibronectin, collagen types I and IV, and laminin. Moreover, biomechanical testing revealed a decrease in the compressive modulus of decellularized compared to fresh kidneys.
As with all organs, research into the construction of a kidney raises numerous questions about the preparation of a matrix and the sources of the cells destined for recellularization. Biological matrices have proved their superiority over the synthetic matrices sometimes used in tissue engineering. In the case of the kidney, the most frequently employed matrices are allogenic, even though xenogenic matrices could be considered, although they might be subject to specific immunological and regulatory issues [31].
A large number of problems remain to be resolved before a kidney can be prepared or constructed from an extra-cellular matrix. Furthermore, none of the ‘self-constructed’ organs in animals have proved capable of performing the vital function in the recipient for longer than a few hours. In the case of the kidney, no transplant has yet been reported even though it is the main challenge for research. The objective remains plausible, however, even if clinical applications appear to be very remote, certainly not before 15 to 20 years [32].
The development of reconstructed organs could open new perspectives in the clinics, mainly in pathologies where organ transplantation is needed. Among the two steps involved on organ reconstruction that are organ decellularization and organ recellularization, the first one is fairly advanced and different protocols are now available. Emphasis need to be placed on the way to better recellularize the organ and the cells that should be used.
Thus, before therapeutics can be applied in clinical practice, many researches are necessary to understand the behaviour of cells upon seeding into decellularized organs as well as the mechanisms of their interaction with the microenvironment. The mechanism of action of stem cell therapy is still being determined and the general today consensus suggests that the most probable mechanism may be through the release of cytokines and other growth-promoting molecules.
The regeneration of organs and the use of stem cells in clinical uses are and will remain a challenge for the development of cell therapy and xenografts. Adult stem cells and in particular mesenchymal stem cells provide exciting development of regenerative medicine. However, until now many problems remain to be solved:
Scientific knowledge and technical problems which can lead to the development of innovative strategies (quality of cells and their role in producing tissue repair, importance of mechanical signals, etc.).
Increase of the yield of preparation of the differentiated stem cells and study of the heterogeneous character of the preparations.
Possibility to have a standardized and reproducible product (preparation of controlled batches).
Grafting: can be introduced via direct or after implantation (cell therapy), or gene therapy.
Risk of teratogenic effect and of immune reaction (i.e., in the umbilical cord cells the immune risk being weaker).
Religious and legal issues with respect to the different country regulations.
Current knowledges allow optimism for the future but definitive answers can only be given after long term animal studies and controlled clinical studies.
Conflict of interest
The authors have no conflict of interest to report.