
Abstract
Hydroxyapatite (HA) is a representative bone repairing biomaterial for its similar composition to human bones and teeth. However, pure HA is limited in application for some unwanted characteristic, such as it is brickle and weakness in degradation. In this study, we modified HA by doping magnesium (Mg) to the material and studied its property in vitro. Besides, we also evaluated the calvarial defect repair effect using MgHA combined with rhBMP-2 in goat model. According to our outcomes, HA composited Mg made the scaffold smooth and the pore regular. In vitro study, Mg could increase the Ca releasing, which may reflect a faster degradation property modified by Mg. And then, MgHA improved the cell viability and proliferation. Furthermore, MgHA could increase the expression of ALP, Collagen I and VEGF protein compared with pure HA (
Introduction
Bone defect usually occurs after severe fracture, sequestrum resection, bone neoplasm operation, et al. and remains a troublesome problem in orthopedic surgery [1,2]. Therefore, a large number of researchers have put great efforts to study the proper materials to repair the defect and tremendous work has been done in this field. However, the completely satisfied substitutes for bone transplantations are still in controversy and none of them could be comparable to autogenous bone yet [3,4].
Hydroxyapatite (HA) is a representative bone repairing biomaterial for its similar composition to human bones and teeth [5–7]. It has been reported to have outstanding biocompatibility and was not only widely used in bone tissue engineering, but also introduced to clinic [8–11]. However, the pure HA material still has limitations in application for some unwanted characteristic, such as it is brickle and weakness in degradation [12,13]. Consequently, it is necessary to modified the bioceramics materials and improve its biological properties.
Biotic bone is not only composed of HA and collagen, but also containing trace amount other elements such as Mg, Sr, Si, copper, zinc, and Ag, which also play important role in its biological characteristic. Therefore, adding metal ion to the material to modify its properties is becoming popular [14–17]. Magnesium is a vital and widely used component for the bone substitutes [18]. It has been proved to have unique biocompatibility, nontoxicity and bone formation effects [19–21]. Moreover, Mg may also have effect on angiogenesis according to the literature [22,23]. However, Mg alloys was reported to have high corrosion rate and early inflammatory reaction around implants in vivo, which have limited the clinical application [24,25]. Consequently, choosing a proper way to use the Mg in bone tissue engineering is significant.
In this study, we doped proper content of Mg to HA, which was not only improved the scaffold’s bioactivity and avoided the weakness of the Mg alloys, but also could make the scaffold obtain osteogenesis and angiogenesis effects theoretically. Furthermore, to increase the bone formation ability, we combined our scaffold with recombinant human bone morphogenetic protein-2 (BMP-2), which is a growth factor and has been proved to have high activity of osteogenic induction [3,26]. This research was conducted to study the property of MgHA in vitro, and analyze its osteogenesis and angiogenesis effects. After that, we evaluated the bone defect repair effect using MgHA combined with rhBMP-2 in goat model.
Materials and methods
Scaffold fabrication
MgHA powders were obtained using chemical precipitation. Porous MgHA scaffolds containing different concentrations of Mg and pure HA scaffolds were prepared as follows: Ca(NO3)2 ∙ 4H2O and NH4H2PO4 were dissolved in distilled water and then stirred ten minutes until the substance was dissolved completely. After that, the pH of NH4H2PO4 solution was buffered close to 10 using NH3 ∙ H2O, and then poured the adjusted NH4H2PO4 solution into Ca(NO3)2 ∙ 4H2O solution slowly, stirring and adding Mg(NO3)2 solid with molar ratio of Mg2+/Ca2+ = 1:99, 3:97, 5:95 and 10:90, which formed MgHA containing 1%, 3%, 5% and 10% concentration of Mg. The last, mixtures were stirred for 1 h at 60°C and precipitation was completed. The precipitates were washed with distilled water until the pH of filtrate was about 7. MgHA precursors were achieved via filtering and drying (at 80°C) the washed precipitates, and then the precursors were ground and screened to produce powders. The powders with a size of 50–75
The scaffolds were tested by X-ray diffractometer (XRD, 3KWX, Philips, The Netherlands). And then, the morphology of obtained scaffolds was observed by scanning electron microscopy (SEM, Japan Electronics Co., Ltd.).
In vitro study
Evaluation of the degradation of MgHA in cell culture
Human osteoblasts cells (MG63) with a density of
The effect of MgHA scaffolds’s cytotoxicity and proliferation of osteoblast
To explore the cytotoxicity, study the effect of MgHA scaffolds on proliferation of MG63 and determine the most optimal concentration Mg briefly, MTT assay was operated to evaluate them. Briefly, sterilized MgHA and HA scaffolds were immersed in culture mediums for 24 h at 37°C and then the viable cells were cultured on each sample for 3, 7, 10 and 14 days. At the specified time, 20 μl/well of MTT solution (5 mg/ml in phosphate buffered saline) was added and then the plate was incubated at 37°C to form formazan crystals. After 4 h, the MTT solution was removed and 200
MG63 were seeded onto scaffolds respectively at a density of
Preparation of the composite materials
1 milligram of rhBMP-2 (Yantai Zhenhai BioTech Co., Ltd.) were dissolved in 100 mL of deionized H2O. The prepared 5%MgHA scaffold was soaked in the protein solution, placed in a freeze dryer (Shanghai Bilon Instrument, Co., Ltd., Shanghai, China) for 24 h, and frozen at −55°C for 48 h. The scaffolds were sterilized by γ-rays (60 Co) at a dose of 25 kGy. The morphology of obtained scaffolds was observed by scanning electron microscopy (SEM, Japan Electronics Co., Ltd.).
Western blot analysis for ALP, Collagen I
ALP and Collagen I were analyzed using Western blot. Briefly, after these scaffold samples were co-cultured with HUVECs and MG63 (1:2) for 14 days, cells were lysed and freeze-thawed in RIPA buffer (150 mM NaCl, 50 mM Tris–HCl, pH 7.5, 1% deoxycholate, 0.1% SDS, 1% Triton X-100), which containing protease inhibitors. And then, reduced proteins were resolved by 10% Tris–HCl polyacrylamide gel electrophoresis (Bio-Rad Gels) and transferred onto a nitrocellulose membrane (Amersham, New York, American). The membranes were blocked overnight in Tris–buffered saline containing 5% skim milk and 0.05% Tween-20 (TBST). After that, ALP and Collagen I were detected with a rabbit anti human polyclonal antibody (1:1000), Blots were again washed three times with TBST metioned above, and immunoreactive bands were visualized using the ECL plus Western blotting detection reagents (Sigma). The antibody-bound protein intensities were analyzed using a hemi-imager-5500 V 2.03 electrophoresis gel image system.
VEGF measured by double ligand enzyme-linked immunosorbent assay (ELISA)
The protein secretion of VEGF was evaluated by double ligand enzyme-linked immunosorbent assay (ELISA). After these scaffold samples were co-cultured with HUVECs and MG63 (1:2) for 14 days, the supernatant liquid for the ELISA assay was collected through centrifugation at 14 000 rpm for 5 minutes. According to the instructions (R&D Corp.) on the kit, the concentrations of these proteins were accurately determined and their values were expressed as pg/ml.
Evaluation of the bone defect repair effect of the scaffold in goat model
Preparation of animals
Eighteen healthy adult goats (animal experimental center of west China hospital, Sichuan University, Chengdu, China) weighing 20–25 kg, male and female unlimited comprised the animal experimental model used. The goats were randomly divided into two groups: group I (
Surgical procedures
The animals were anesthetized with 0.1 ml/kg of sumianxin II via intramuscular administration. During operation, intravenous injection of 10% of the chloral hydrate was performed to maintain the deep anesthesia. With the prone position, the areas of the top of the cranium were shaved before surgery, and the surgical field was prepared with an iodine solution. We made a 30 mm longitudinal incision at bilateral parietal, and dissected through the skin, subcutaneous tissue, fascia, and then exposed parietal bone. A symmetrical round 15 mm diameter bony defect was then formed at the bilateral parietal using 15 mm diameter trephine.
After the bone defect was constructed, the right sides of the defects of the goat in group I were filled with magnesium-doped porous HA scaffold combined rhBMP-2 (Group A). The left sides were only filled with magnesium-doped porous HA scaffold (Group B). For the comparison, the two sides of the calvarial defects in group II were both filled with pure porous HA (Group C).
To prevent wound infection, all goats were intramuscularly injected with penicillin (800,000 U/d), one preoperative dose and three postoperative doses.
Radiologic analysis
The goat calvarial computed tomography (CT) examination were obtained post operation at week 4, 8, 12 after operation to evaluate the absorption, degradation of implanted materials at the defect regions. BI-2000 medical image analysis system was used to analyze the CT film, which measured the mean gray value of all levels of the defect regions. A higher value suggests a better defect healing.
Histological and histometric analysis
Histological observations were performed at week 4, 8, 12 after operation respectively. The implants were cut and fixed in the 10% formaldehyde for a week. The implants were then decalcified in 20% EDTA solution for about six months and then dehydrated through a gradient ethanol series, cleared in xylene, and embedded in paraffin. Sections with 4 μm thick were made and stored in thermostat of 37°C. Specimen sections were stained with haematoxylin and eosin (HE), Masson’s trichrome and toluidine blue (TB). At last, each piece of the sections was observed by light microscope (BX41, Olympus, Japan).
In addition, HE dyeing histological section was used to calculate the percentage of the new bone in the defect regions with the method of histomorphometry and the data was analyzed by BI-2000 medical image analysis system. New bone formation area (%) = new bone formation area/Bone defect area ×100%.
Real-time PCR
The specimens obtained at 12 weeks postoperatively were snap frozen in liquid nitrogen and completely grounded into powder and homogenized. To evaluate the expression of Collagen I and VEGF, real-time PCR was performed. Briefly, Total RNA was extracted with TRIzol solution (Invitrogen, Carlsbad, CA, USA) and reverse transcribed to complementary DNA using the QuantiTect Reverse Transcription Kit (Thermo Fisher Scientific Inc., Fremont, CA, USA). The specific transcripts were quantified by quantitative real-time polymerase chain reaction (PCR) with QuantiTect SYBR Green PCR Kit (Takara Bio Inc., Tokyo, Japan) and analyzed using ABI 7500 real-time PCR system (Applied Biosystems, Foster City, CA, USA). And then, we obtained the sequences of gene-specific primers of Collagen I and VEGF. Products of Collagen I and VEGF were 325 bp and 303 bp oligonucleotides. PCR was performed in 40 cycles at 94°C for 15 s, 55°C for 30 s and 72°C for 30 s. The relative mRNA expression was calculated with comparative CT method.
Statistical analysis
The SPSS19.0 software (SPSS Inc., Chicago, IL, USA) was used for the statistical analysis. The results were analyzed with one-way variance analysis, the each two groups were compared with SNK-q test and LSD test, with
Results
Characterization of the MgHA scaffold
According to the Fig. 1, The incorporation of low-dose Mg into HA did not change the crystal structure of HA, but the HA diffraction peaks were accompanied with diffraction peaks of β-tricalcium phosphate, which indicated that incorporation of Mg leads a amount of HA decomposed into β-TCP.

XRD data of MgHA.
We obtained the HA scaffolds with 70% porosity and the micropores were uniform distributed on the scaffolds (Fig. 2(a)). At high magnification, we can see the morphological regular of granular structure and irregular pores (Fig. 2(b)). After the Mg was doped into the HA, the granular structure became variable in size but the surface of the scaffolds were more smooth and the micropores more regular (Fig. 2(c)).
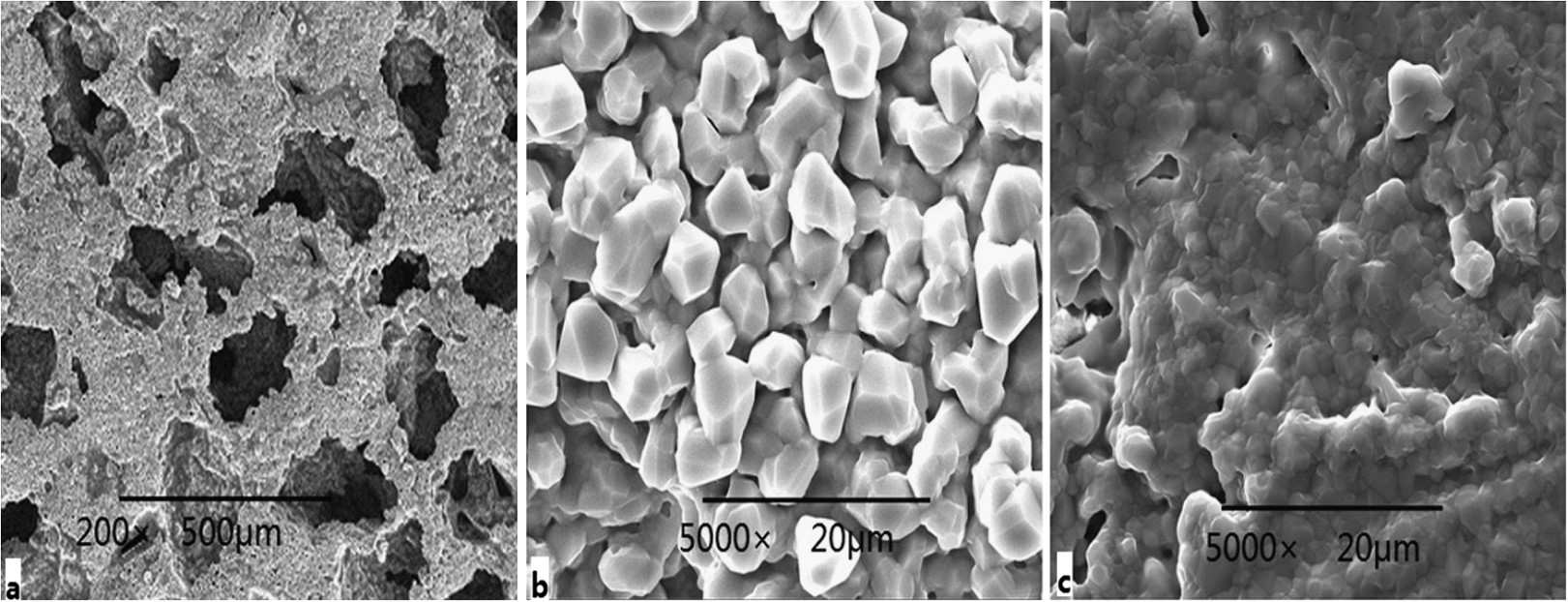
SEM images showing the micropore and surface morphology of the scaffolds. (a) HA scaffold at low magnification (200×); (b) HA scaffold at high magnification (5000×); (c) MgHA scaffold at high magnification (5000×).
Figure 3(a) shows the cumulative Mg release of MgHA scaffolds immersed in cell culture. With the increasing of the Mg content, its release curve is steeper. Figure 3(b) shows the lost mount of the Ca, at any time, it demonstrated that the Ca release of MgHA had a higher level than HA, which indicated the Mg doped into the HA can contribute to degradation of the scaffolds. However, both the release of Mg and Ca didn’t reach the accelerating phase.

The curve of cumulative magnesium release (a) and cumulative calcium release (b) of MgHA and HA (
To find out the most proper content of Mg, MTT assay was an effective method to assess the cytotoxicity and proliferation. As the Fig. 4 showed, at the first seven days, the cell proliferation was without significance among the groups (
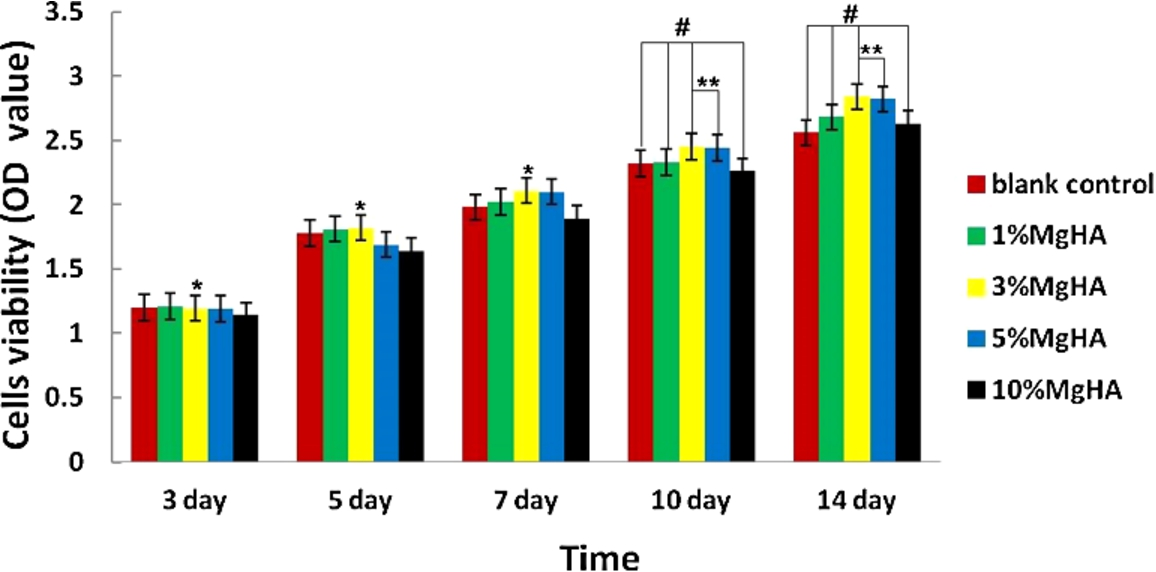
OD values of osteoblasts cultured with 1% MgHA, 3% MgHA, 5%MgHA, 10MgHA and blank control group.

Fluorescence staining photos on the scaffolds in blank control group (a), 1%MgHA group (b), 3%MgHA group (c), 5%MgHA group (d) and 10%MgHA group (e).
According to the Fig. 6, we can see some floccules on the surface of the scaffolds and in the micropore, which suggests that the rhBMP-2 has been located on the material. ALP and Collagen I are two potent factors to prove the osteogenesis, while VEGF is an angiogenic growth factor with the ability to stimulate endothelial cell proliferation and migration. In our experiment, western blot was used to quantificationally analyze the ALP and Col I and ELISA was used in our study the levels of VEGF. As presented in Fig. 7 and Fig. 8, the 5%MgHA/rhBMP-2 group, the amount of ALP, Collagen I were much better than the other two groups at day 3, day 7 and day 14. The VEGF expression in 5%MgHA/rhBMP-2 group was not significant difference compared with other three groups at day 3, but at day 7 and day 14, they are much better. At the same time, the 5%MgHA group at the day 3 and day 7 were not superior to the HA and blank control group on protein secretion, but at day 14, the outcome was higher than that in the other two groups.

SEM images showing the surface morphology of the MgHA scaffold when composited with rhBMP-2.

The western blot of cellular ALP and Col I expression.

The effect of various scaffolds on cellular VEGF secretion.
General condition of the animals
All the animals accomplished the experiment, as the Fig. 9 shows, the defect models were well structured and the scaffolds were properly implanted. After the operation, all goats’ activities and diet were normal. In addition, serious complications, such as infection, fracture, pneumonia, etc did not occur.

Photographs of in vivo goat modeling. Defects on cranial bone (a) and (b) materials implanted.
According to the examination of the CT films, Fig. 10 shows the three-dimensional reconstruction of the defect at the twelfth week, it revealed that the scaffold in group A had been degraded to some extent and lost its shape, for comparison, group B’ scaffolds had degradation at the edges of materials and its shape remained clear. However, we didn’t see the scaffolds in group C had obvious degradation and its shape almost kept unchanged. Figure 11 shows the coronal plane of the defect and Fig. 12 was the sagittal plane of the defects. At the fourth week (Fig. 11(a), (d) and Fig. 12(a), (b), (c)), all groups had formed some bone callus, but the group C was relative rare. At the eighth week (Fig. 11(b), (e) and Fig. 12(d), (e), (f)), group A showed the continuity of callus and new bone formation in the defect, while the group B and group C presented obvious large area of the defects remain. At the twelfth week (Fig. 11(c), (f) and Fig. 12 (g), (h), (i)), the defects in group A almost filled with new bone and callus, group B had formed continuous callus, while group C had not seen obvious improvement of the defect healing compared with the previous observation.

Three-dimensional computed tomography examination (3D CT) of the goat skull 12 weeks after surgery. White arrow indicates the 5%MgHA/rhBMP-2 group and grey arrow indicates the MgHA group (a); yellow arrows indicate the pure HA group.

Photographs of CT coronal plane. White arrow indicates the 5%MgHA/rhBMP-2 group and grey arrow indicates the MgHA group; yellow arrows indicate the pure HA group. (a) and (d) shows the photographs at 4 week after operation; (b) and (e) shows the photographs at 8 week after operation; (c) and (f) shows the photographs at 12 week after operation.
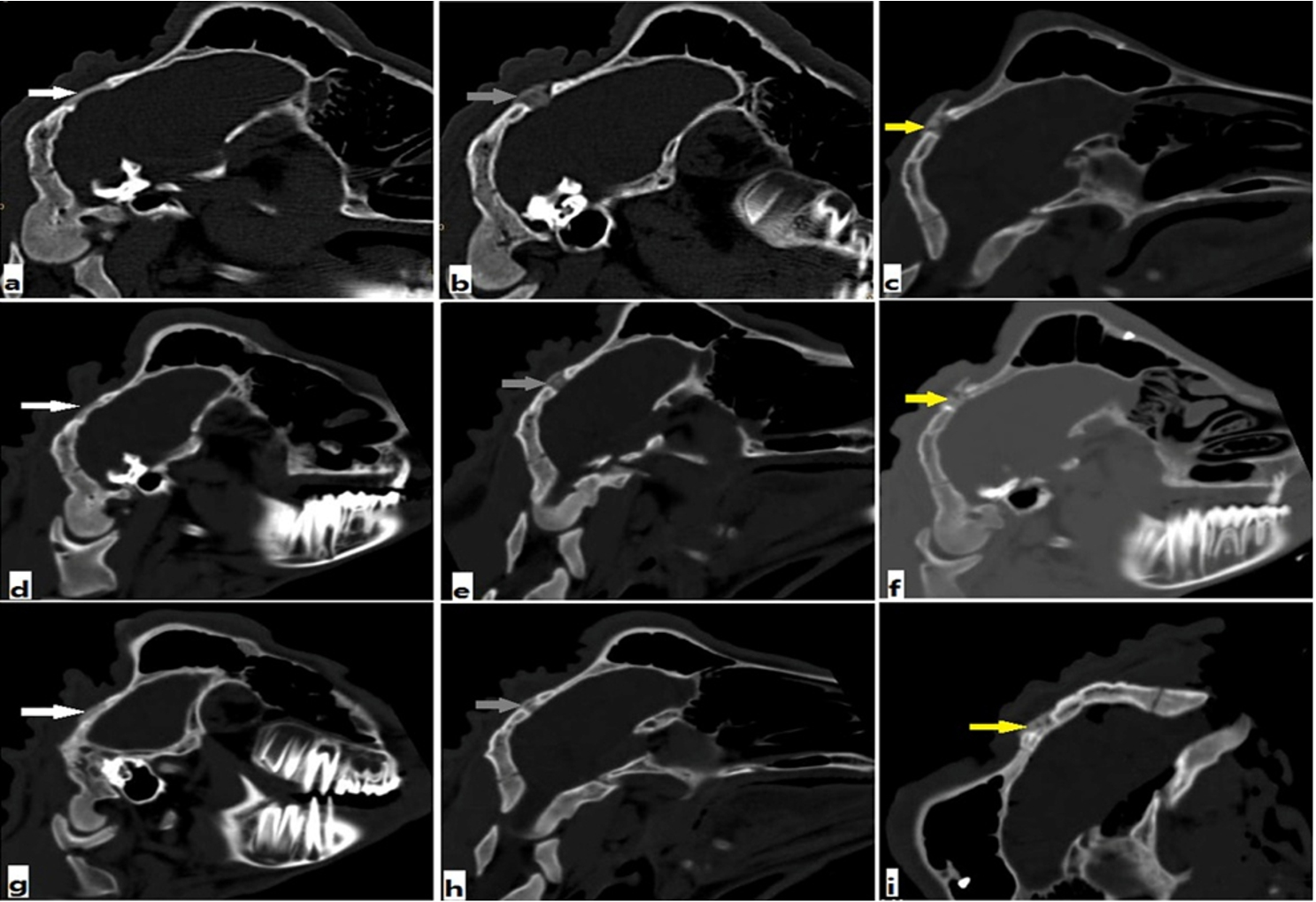
Photographs of CT vertical plane. White arrow indicates the 5%MgHA/rhBMP-2 group ((a), (d), (g)) and grey arrow indicates the MgHA group ((b), (e), (h)); yellow arrows indicate the pure HA group ((c), (f), (i)). (a), (b), (c) shows the photographs at 4 week after operation; (d), (e), (f) shows the photographs at 8 week after operation; (g), (h), (i) and (f) shows the photographs at 12 week after operation.
When conducted image analysis of the CT films (Fig. 13), the average gray values of the defect regions at all levels in each groups increased over time, and the differences were significant (

Mean gray values in the four groups at 4 weeks, 8 weeks and 12 weeks respectively (
According to the HE and Masson dyeing (Fig. 14 and Fig. 15(a)–(f)), the implanted materials had small amount of degradation in groups A, B at the fourth week, but we can see the formation of new bone, fibrous tissue. In group C, the defect regions were almost blank and only a little new bone was formed. At the eighth week, the implanted materials were degraded more in the defects and the newly formed had evenly increased in group A and B, while in the defects of group C, still see the host bone and rare of now bone appeared. When it came to the 12th week, large number of the new bone grew into the defects in groups A and B. However, in group C, the new bone remained a small area. Figure 15(g), (h), (i) shows the TB staining of the sections, which help to observe the formation of the cartilage, the group A and group B were also significant better than the group C too.

HE staining of histological sections in group A at 4 weeks (a), at 8 weeks (b) and at 12 weeks (c) after surgery (×200).
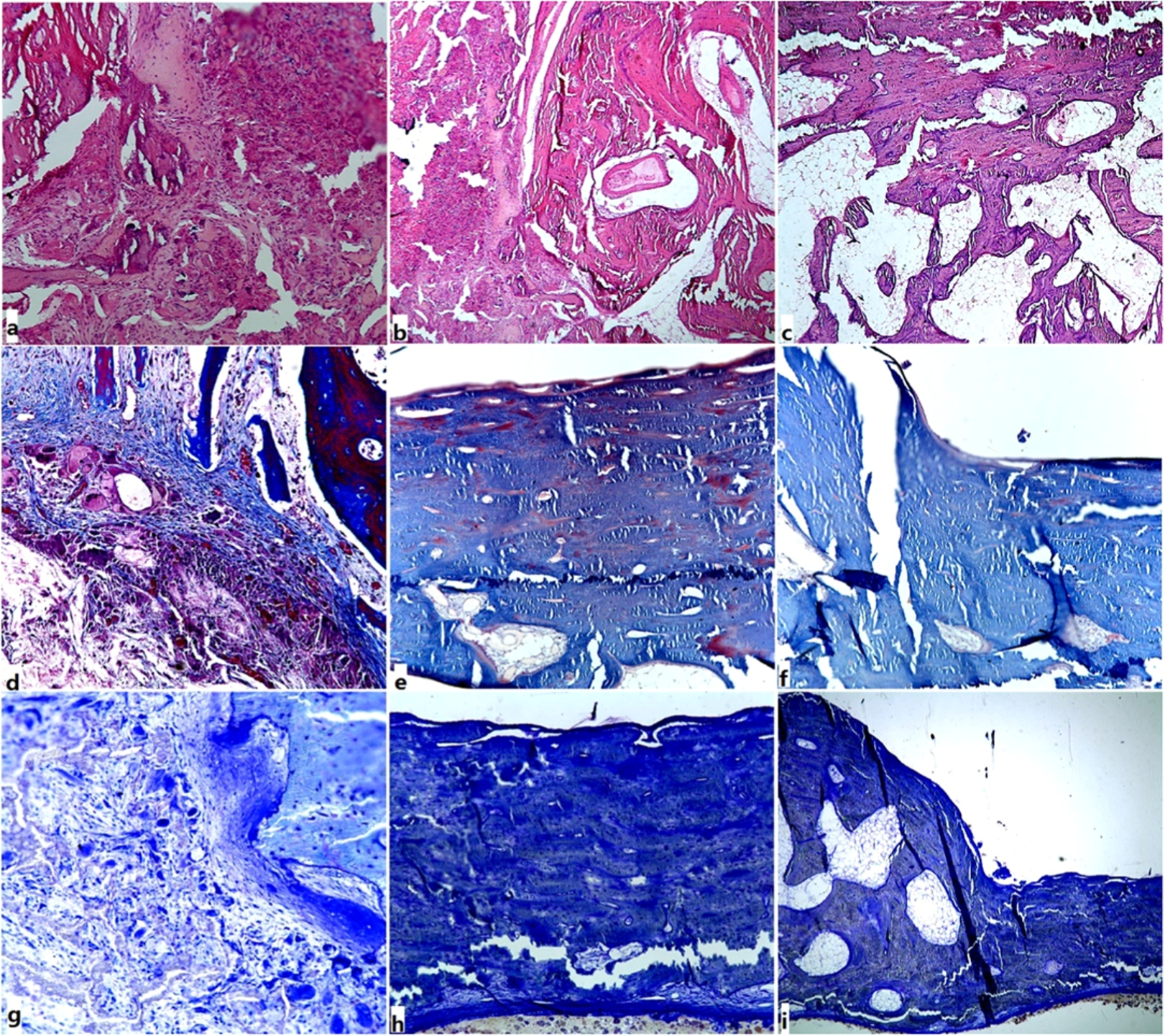
HE staining of histological sections of the three groups at week 12, (a) (HE X100, group A); (b) (HE X100, group B); (c) (HE X100, group C). Masson staining of histological sections at 12 weeks in group A (d) (X100), group B (e) (X100) and group C (f) (X100). TB staining of histological sections at 12 weeks in group A (g) (X100), group B (h) (X100) and group C (i) (X100).
BI-2000 medical image analysis system was used to quantitatively determine the area of new osteogenesis. According to the Fig. 16, the mean osteogenic area in group A was larger than those in group B and group C at all observation time (

The percentage of the mean osteogenic area in the defect regions of the three groups at 4 weeks, 8 weeks and 12 weeks, respectively (
PCR was used to evaluate the osteogenesis and vascularization. We found that the expression of Collagen I mRNA and VEGF in groups A and B were significant higher compared with those in groups C (

Results of real-time PCR of Collagen I and VEGF mRNA at 12 weeks after implantation.
According to this research, HA composited with Mg makes the scaffold more smooth and the porosity more regular. In vitro study, firstly, Mg could increase the Ca releasing from the scaffold, which may reflect a faster degradation property modified by Mg. And then, proper content of Mg in HA improved the cell viability and proliferation. Finally, MgHA could increase the expression of ALP, Collagen I and VEGF protein compared with pure HA. In the vivo study, MgHA shows a better defect healing effect in radiologic evaluation compared with HA, but it inferior to the MgHA scaffold when combined with rhBMP-2. Besides, in the histological analysis, MgHA/rhBMP-2 also shows the most effective bone formation outcome, and the MgHA group is significant better than the pure HA group on osteogenesis. Furthermore, Collagen I and VEGF mRNA expression at 12 week in MgHA/rhBMP-2 group were also significat higher than other two groups.
The surface of the MgHA scaffold become more smooth and the micropores is more regular than the HA scaffold, which may be caused by adding Mg to the HA could lead to β-TCP and subsequently decrease the composite material’s melting point and the irregular space of the particles were filled by the molten mineral material. After soaked in culture medium, MgHA not only improved the dissolution of Ca2+ and Mg2+, as well as the degradation ability of the composited scaffold, but the release rate of Mg2+ was not related to the increasing content of Mg in HA, which may be caused by the different phase composition of various MgHA after the setting process as well as the inhibition of adsorbed protein from culture medium on the material surface [27]. Our results were conformed to Zhang’s work [28], in their study, they doped Mg in calcium phosphate cement and the cement degradation was also significant improved.
As believed, an increase cell adhesion or osteogenic differentiation of the material could lead to the improvement of transplantation efficiency [29]. Based on the data obtained from the in vitro cell culture, it revealed that MgHA with smooth surface were potent inducer of the cell adhesion and 3%, 5%MgHA were most effective on cell viability and proliferation. Also, it could be observed from the immuno-fluoroscope photos that on 3%MgHA and 5%MgHA surfaces, the cell densities were increased. But the 5%MgHA was with more efficiency on degradation, so we choose the 5%MgHA as the proper scaffold for the following experiment.
The MgHA enhanced the ALP, Col I and VEGF expression of the co-cultured cells on the surface at the 14th cultured day, which indicated that the Mg released slowly from the scaffold but it obviously improved the scaffold’s biological activities. As the previous study reported, Mg plays a vital role as a cofactor in numerous enzymatic reactions and it could stabilizes structure of proteins, nucleic acids, modulates signal transduction, and cell proliferation [20,30,31], consequently, a proper content of Mg has an effect on bone mineral metabolism and promote bone formation [32–34]. Furthermore, Mg could also stimulate endothelial proliferation and migration [35,36], so in our study in vitro, the VEGF expression improved. A material with angiogenesis effect is very promising for repairing of bone defect is not only the process of the regeneration of new bone, but also greatly depends on the new formed vessels to supply nutrients and excrete metabolites [4,37,38].
The osteoregeneration results evaluated by CT and histological studies, the Collagen I and VEGF expression confirmed that the MgHA stimulated defect healing and new bone formation more effectively than pure HA, which was consistent with previous studies [19,33,34]. Specifically, MgHA/rhBMP-2 group showed the fastest bone regeneration, suggesting that the magnesium-induced positive effect on cell adhesion and osteogenic differentiation remained valid in vivo, but in can also improved and modified by combining with growth factors. According to Cui et al.’s study [39], adding rhBMP-2 to their composited scaffold Si-HA has promoted the defect recovery, and in our previous research [3], we combined antigen-free bovine cancellous bone with rhBMP-2 for the repair of tibial bone defects in goat model and our outcome showed the experiment groups significant improved bone defect healing effect. Thus, our material with mechanical support and growth factor, and has been studied in vitro and in vivo to prove its bone formation effectiveness, is very encouraging.
Our research provided a promising composited scaffold for bone defect repair. However, our present works also had some limitations. First, we didn’t evaluate the angiogenesis effectively in vivo. Second, to make clear of the mechanism, our detection indexes of this study were limited and more meaningful tests, such as PCR, immunohistochemical staining, et al., need to be accomplished. Third, the sample is relative small. Fourth, we used the cell culture experiments to test the cell activity and cytotoxicity of the scaffold. Fifth, doping Mg into HA could lead HA decompose to β-TCP and our study didn’t explore how much of β-TCP in HA could exert the best physical and chemical properties. We just studied optimal concentration briefly in this method. Therefore, more studies with more sufficient evidence are needed to put into research in the future.
Conclusions
Magnesium has significant effects on bone formation and angiogenesis, and MgHA and MgHA/rhBMP-2 have capacity to promote the repair of bone defects. It is worthy of being recommended to further studies.
Footnotes
Acknowledgement
This study was supported by the National Natural Science Fund of China (81271976/H0605 and 81672165).
Conflict of interest
The authors have no conflict of interest to report.