
Abstract
Objective:
Understanding the biomechanical properties of hernia meshes is essential in facilitating their selection. The aim of this study was to evaluate the mechanical compatibility of hernia meshes and human abdominal fascia and assess their applicability in hernia repair.
Methods:
Uniaxial tensile tests were performed. A total of eight hernia meshes were tested – three standard meshes (Surgimesh®, Surgipro™, TecnoMesh®) and five light-weight meshes (Optilene®, TiO2Mesh™, Parietex™, Vypro™ II, Ultrapro™).
Results:
The secant modulus at 5% strain and the level of orthotropy (the ratio between tensile stress in the longitudinal and the transversal direction) at 5% strain were calculated from the stress–stretch ratio curves. The impact of pore size and thickness on the elastic properties of these meshes was determined. The relationships between density and elasticity as well as between elasticity and the strain developed at 16 N/cm load were presented. The resulting mechanical properties of meshes were compared to the elasticity, orthotropy and deformability of human abdominal fascia.
Conclusions:
Vypro™ II and Parietex™ brands display properties similar to those of fascia in both directions. The TiO2Mesh™ and Ultrapro™ display deformability close to the deformability at 16 N/cm of the fascia transversalis. Only the Vypro™ II brand’s orthotropy is similar to that of fascia.
Introduction
The use of mesh grafts is a standard method in abdominal wall hernia repairs. Numerous hernia meshes are currently used in the surgical practice to augment the abdominal wall. It is extremely difficult for surgeons to select the appropriate mesh because of the large number of meshes available in the clinical practice. There are synthetic, organic, nonabsorbable, partially absorbable, absorbable and coated meshes manufactured by various methods, using polymers of various pores, density and thickness. In the work of Coda et al. 166 hernia meshes were considered for classification depending on their biomaterial properties, while Klinge et al. reported for more than 300 brands of hernia meshes. Some 50 new mesh designs are launched in the market each year [1,2].
The number of publications on the structure and biomechanical properties of hernia meshes has increased. Various studies have presented their properties or evaluated their mechanical compatibility with soft tissues. In all of these studies hernia meshes are investigated using mechanical tests. Loads at failure, suture retension, tear resistance, ball burst strength and compression are determined [3–6]. It is commonly accepted that the biomechanical properties of meshes are important factors to be considered in a hernia surgery. The impact of meshes’ textile characteristics on the outcome of hernia repair has been widely investigated [7]. Hollinski [5,6] presented data on the thickness, weight, pore size, ultimate tensile strength, modulus of elasticity and flexture of 12 meshes. Deeken [3,4] described the same information about nine investigated meshes and calculated the pressure in the abdominal cavity of normal and obese patients. Miao [8] published a comprehensive analysis of the physical characteristics of nine selected brands. Pott [9] evaluated the mechanical characteristics of six meshes and suggested data regarding the directionality of the mechanical properties of meshes to be provided by the manufacturers. Sabersky [10] reported results about the ratio of anisotropy for six meshes. All published studies on the physicochemical properties of hernia meshes will help optimize the outcomes of the operations and assess the benefits and risks of mesh implants.
The main task of any hernia repair is to restore the physiological properties of the abdominal wall. It requires knowledge of both the material properties of hernia meshes and the properties of the abdominal layers. After meshes are implanted the surrounding tissue grows so that, mesh and tissue become an inseparable complex. Hence the emphasis on tensile strength and elasticity of the abdominal wall and its structures focuses attention. The assessment of the mean distention of the abdominal wall and its restriction after the implantation of hernia meshes leads to an investigation of the mechanical compatibility between native tissues and meshes.
Using theoretical tensile stresses generated inside the human abdomen Junge and colleagues calculated that the strain developed in the human anterior wall at load 16 N/cm is between 10%–30% [11]. According to Deeken et al. materials that demonstrate less than 10–30% elongation at 16 N/cm will stretch less than the native human abdominal wall and will result in greater foreign body sensation or discomfort [3]. Meshes that stretch more than 30% in length could result in bulging or hernia recurrence.
On the basis of spherical and cylindrical pressure models Klinge et al. and Deeken et al. evaluated the impact of abdominal size and intra abdominal pressure (IAP) on the stress generated inside the human abdomen [2,3]. It was predicted that theoretical tensile stress would be between 10.5 N/cm in a normal weight female patient with an IAP of 20 kPa and up to 47.8 N/cm for obese male patients with an IAP of 30 kPa.
A different approach for evaluating the mechanical compatibility and load bearing capacity of hernia meshes is to compare the deformability of mesh samples at the maximum stress developed in fascia samples, e.g. – 0.4 MPa, 1 MPa and 2 MPa [12]. The mechanical behaviors of three heavyweight meshes were determined. When a stress level of 0.4 MPa (which corresponds to 5% strain applied to fascia samples) was applied, the deformability of hernia meshes in both orthogonal directions was close to the deformability of fascia samples (3–7%). When a stress of 1 MPa (which corresponds to 10% strain applied to fascia samples) was applied a huge mismatch in the deformation of mesh samples was observed. It increased between 12.84%–22.47% in longitudinal and 4.8%–12.5% in transversal direction. This could cause an increase of tensions in the tissues surrounding the hernia meshes. The deformability of hernia meshes at a tensile stress of 2 MPa (mean stress for fascia transversalis in longitudinal direction at 15% strain) was in the 8.5%–45.92% range [12]. The results indicate that in case of deformations which are above the physiological load the mismatch between the mechanical properties of fascia layers and those of hernia meshes increases enormously.
The first generation of meshes, i.e. heavyweight meshes are still used, but to improve the quality of life of patients manufactures have reduced the volume of the material increasing the pores of meshes. Implantations of lightweight meshes with large pores cause less scarring tissue while stiffness of the abdominal wall and chronic pain decrease [13]. However the use of lightweight meshes in hernia repair remains controversial, because of their long-term effects: their use is associated with a higher recurrence rate as compared to heavyweight meshes implantation [6,14]. According to Weyhe material reduction and coatings are not the only way to improve the biocompatibility of meshes. Mesh construction is actually characterized by pore size, filament structure, thickness and porosity. These characteristics are more important determinants of foreign body reaction and outcomes after implantation [14]. Practical recommendations about the process of implantation are included in the articles of Klinge, Deeken and Holinski [2–6].
The need to know more about the mechanical compatibility between hernia meshes and the tissues they substitute have stirred our interest in the matter.
The aim of this study is to evaluate the mechanical compatibility of hernia meshes and human abdominal fascia and thus to assess their applicability in hernia repair.
A list of tested meshes and their characteristics
A list of tested meshes and their characteristics
Nine knitted meshes that typically represented standard (Surgimesh® (SM), Surgipro™ (SP), TecnoMesh® (TM)) and lightweight meshes (Optilene® (OL), TiO2Mesh™ (TO), Parietex™ (PT), Vypro™ II (VP), Ultrapro™ (UP)) were selected. Information about the tested meshes is presented in Table 1. We used Coda’s classification [1]. Five lightweight meshes with density 35–70 g/m2 and three standard meshes with density 71–140 g/m2 were investigated. Light microscopy was used to perform a morphometric analysis to measure both the pore size and the filament diameter. A sample of each mesh material was photographed using a digital camera of light microscope (Fig. 1). The thickness of each mesh was determined using a digital micrometer.
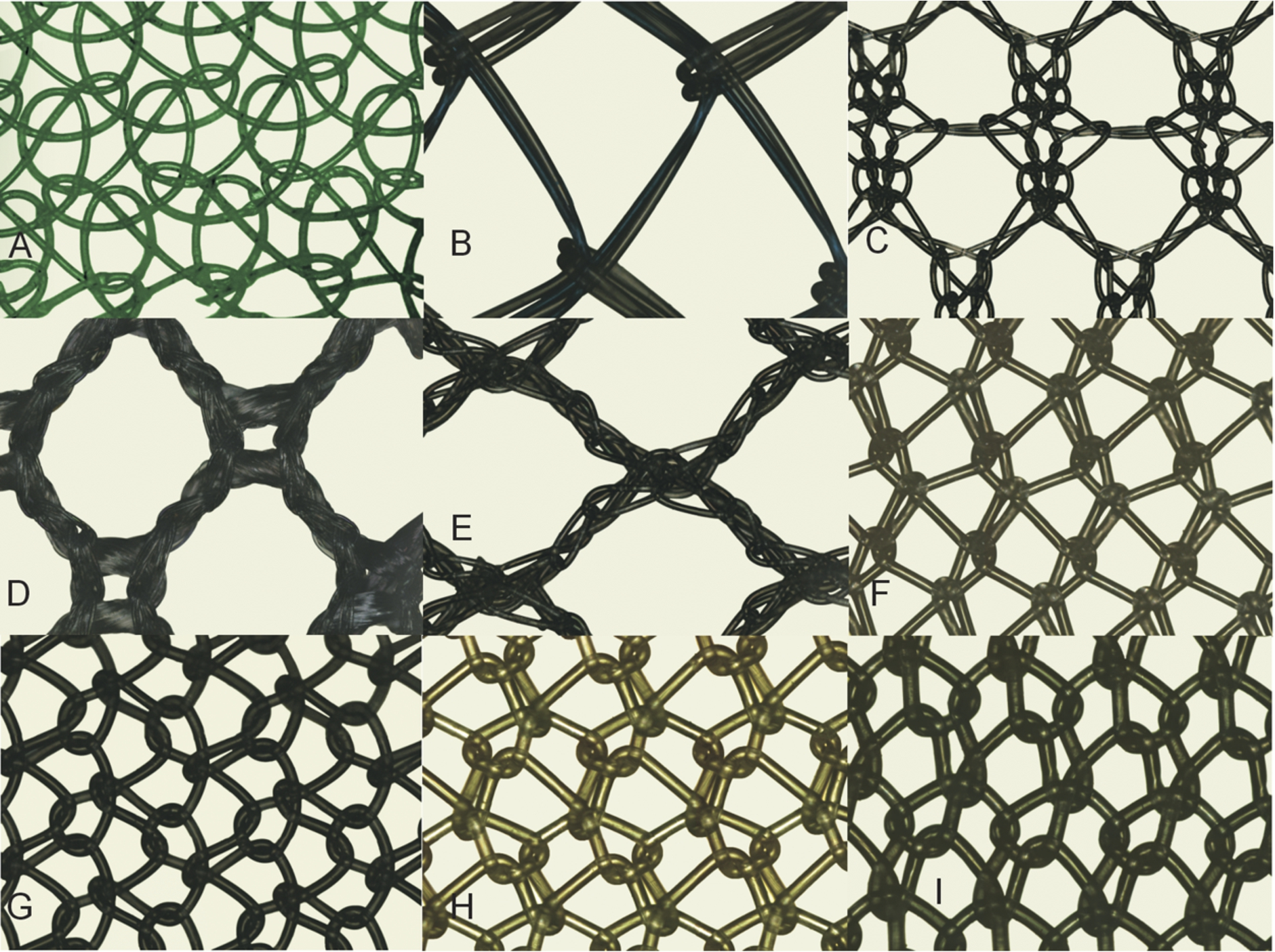
Augmentation picture of each investigated mesh in this study: (A) Optilene®, (B) TiO2Mesh™, (C) Parietex™, (D) Vypro™ II, (E) Ultrapro™, (F) Surgimesh®14, (G) Surgipro™, (H) TecnoMesh®, (I) Surgimesh®20.
The main material of meshes is polypropylene (PP), only Parietex™ is from polyester. We used four polypropylene meshes (Optilene®, Surgimesh®, Surgipro™ and TecnoMesh®), one polypropylene mesh with titanium coatings (TiO2Mesh™) and two meshes which are partially absorbable (Vypro™ II and Ultrapro™). Two of the standard meshes SM14 and SM20 come from one brand (Surgimesh®) but differ in filament diameter and porosity. SM14 denotes Surgimesh® with filament diameter 0.14 mm, while SM20 denotes Surgimesh® with filament diameter 0.2 mm.
The weight was measured using a highly accurate electronic balance (AJ 150, Mettler Instrument Corporation, Switzerland). The area weight was registered in g/m2.
To verify the biomechanical properties of each mesh before implantation, we used a universal testing machine (FU 1000E, Germany) equipped with a 500 N load cell with minimal value of the load of 0.2 N and minimal value of the displacement of 0.1 mm. The strain rate was 0.13 mm/s. Uniaxial tensile tests were performed on five samples along each orthogonal direction (parallel to column of loops (L direction) and perpendicular to it (T direction)). A rectangular specimen size
Statistical analysis was performed using STATISTICA version 13 software. The results were presented as
We measured the main structural characteristics of the investigated hernia meshes – filament diameter, thickness, pore size and density (Table 2). Eight out of nine meshes are manufactured from monofilament fibers. Only Vypro™ II has a multifilament structure. The filament diameter is between 0.04–0.20 mm. The filament diameter of lightweight meshes is in the range 0.04–0.15 mm and 0.14–0.20 mm for standard meshes. Vypro™ II displayed the smallest value of filament diameter – 0.04 mm, while TecnoMesh® and Surgimesh®20 exhibited the largest value of filament diameter – 0.20 mm, which is 5 times larger than the thinnest diameter.
Main structural characteristics of hernia meshes
Main structural characteristics of hernia meshes
The thickness is in the range 0.25–0.6 mm, pore size is between 0.3–3.0 mm and density ranges from 36 g/m2to 130 g/m2. To characterize pore size we used the classification system proposed by Earle & Mark [18]. Thus TiO2Mesh™, Vypro™ II and Ultrapro™ have very large pores (>2 mm), Parietex™ has large pores (1–2 mm), medium pores has Optilene® (pores in the range 0.6–1.0 mm), while Surgimesh®14, Surgipro™, TecnoMesh® and Surgimesh®20 have pores that are between small and medium in size (small pores have dimensions 0.1–0.6 mm).
The heaviest mesh is Surgimesh®20 (130 g/m2) and the lightest mesh is Optilene® (36 g/m2). The mean density of lightweight meshes is
The results from statistical analysis showed that the ultimate Lagrangian tensile strength was not significantly lower in the lightweight mesh group as compared to the standard mesh group for L direction (7.11 MPa vs. 9.12 MPa,
Mechanical characteristics of hernia meshes
∗
The modulus of elasticity, strain at physiologically relevant loads at 16 N/cm and orthotropy of the meshes are presented in Table 3. The parameters are presented as
The mean value of elastic modulus at 5% deformation for lightweight meshes is
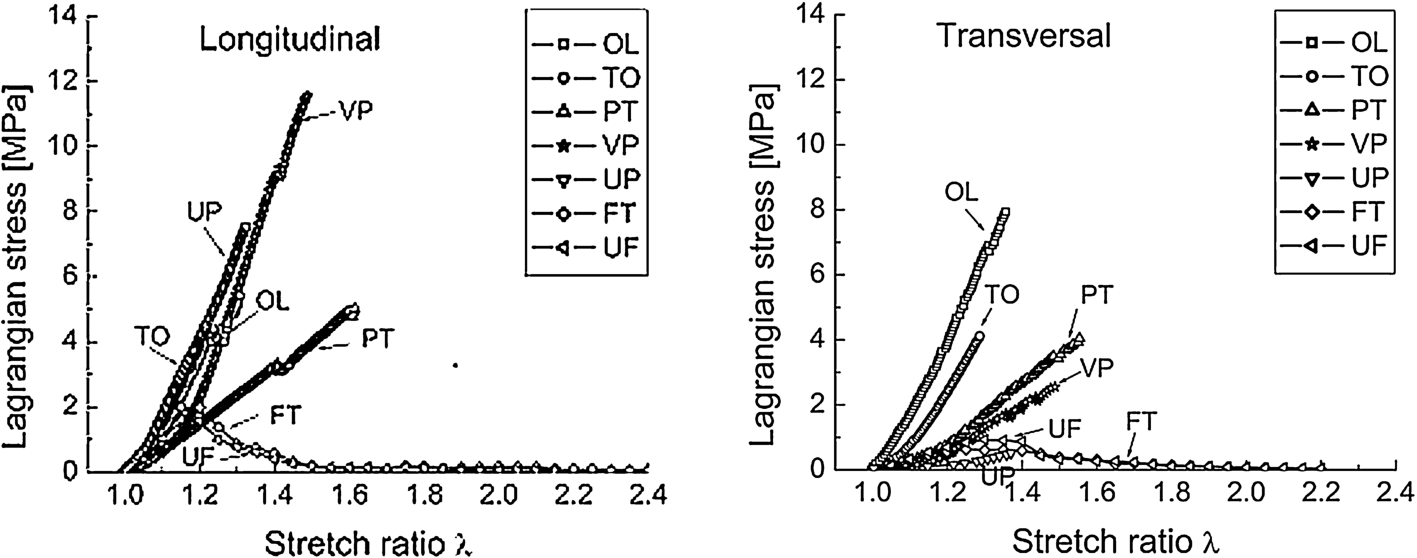
The elastic properties of the umbilical fascia (UF), fascia transversalis (FT) and lightweight meshes Optilene® (OL), TiO2Mesh™ (TO), Parietex™ (PT), Vypro™ II (VP), Ultrapro™ (UP) in the longitudinal (left) and transversal direction (right).
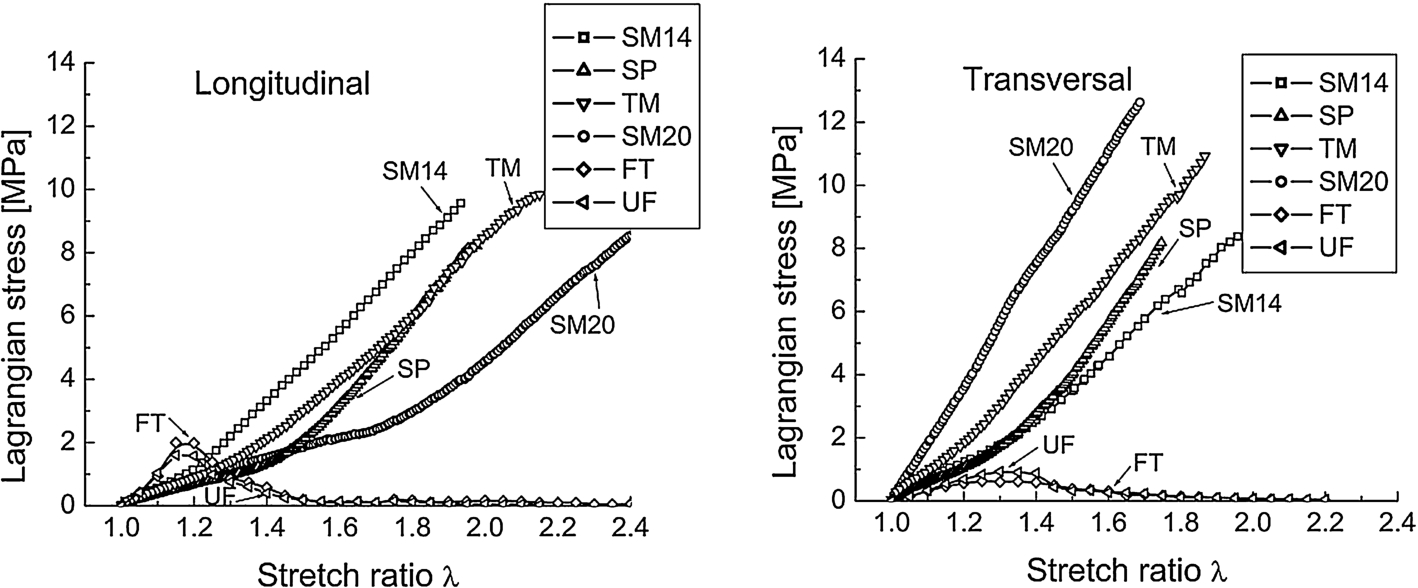
The elastic properties of the umbilical fascia (UF), fascia transversalis (FT) and standard meshes Surgimesh® (SM) (SM14 denoted Surgimesh® with filament diameter 0.14 mm, while SM20 denoted Surgimesh® with filament diameter 0.2 mm), Surgipro™ (SP), TecnoMesh®™ in the longitudinal (left) and transversal direction (right).
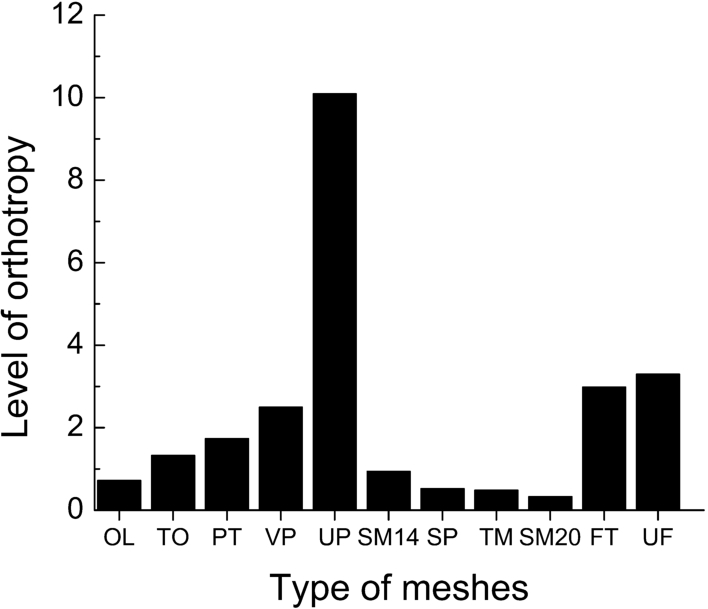
The level of orthotropy of hernia meshes, ordered according to increasing density: Optilene® (OL), TiO2Mesh™ (TO), Parietex™ (PT), Vypro™ II (VP), Ultrapro™ (UP), Surgimesh® (SM14), Surgipro™ (SP), TecnoMesh® (TM), Surgimesh® (SM20), fascia transverrsalis (FT) and fascia umbilicalis (UF).
The level of orthotropy for the investigated meshes is compared (Fig. 4). The level of orthotropy of standard meshes is between 0.48–0.95, while for lightweight meshes it is 0.72–10.09. Four of the meshes (Parietex™, TiO2Mesh™, Ultrapro™ and Vypro™ II) have a level of orthotropy higher than 1 (
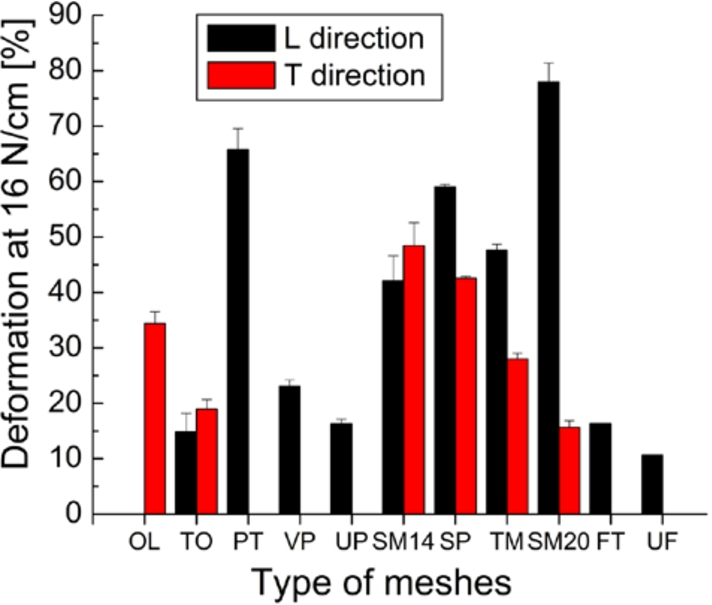
A deformation at 16 N/cm of the human fascia and all meshes ordered according to increasing density Optilene® (OL), TiO2Mesh™ (TO), Parietex™ (PT), Vypro™ II (VP), Ultrapro™ (UP), Surgimesh® (SM14), Surgipro™ (SP), TecnoMesh® (TM), Surgimesh® (SM20).
The levels of deformability at 16 N/cm are presented in Fig. 5. For Optilene®, Vypro™ II, Ultrapro™ and fascia in one direction the maximum load was less than 16 N/cm. The meshes exhibited various degrees of deformability from 15.66% to 78% and the difference between deformability in both directions was in the range 6–63%. TecnoMesh® and Surgimesh®20 being the most anisotropic meshes demonstrated a mismatch in direction deformability of 19.6% and 63%, respectively. Deformation at 16 N/cm of the fascia transversalis was 16.33% and only the TiO2Mesh™ and Ultrapro™ meshes displayed similar properties (Fig. 5).
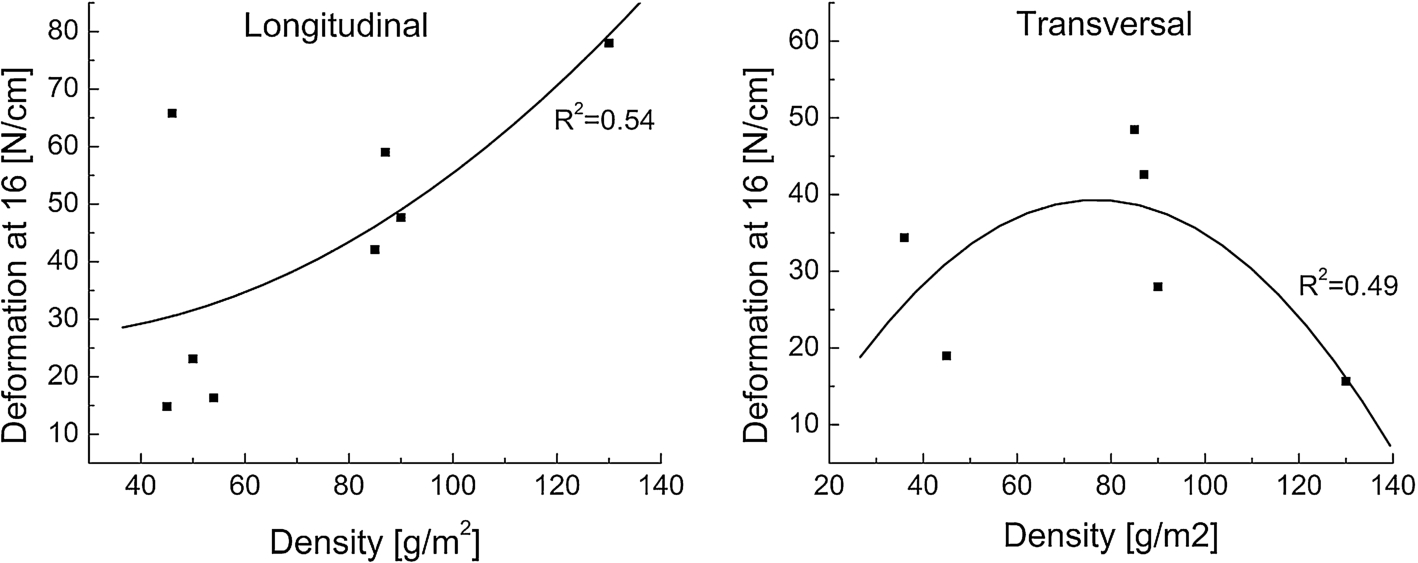
Correlation between mesh weight and deformation at load 16 N/cm in the longitudinal (left) and transversal direction (right).
The relationships between density and deformation at 16 N/cm in both directions are shown in Fig. 6. In the L direction deformation increased with density increase (Fig. 6(left)), while in the T direction the opposite trend was observed (Fig. 6(right)). Data was approximated with the polynomial and the regression coefficient R2 was 0.54 and 0.49, respectively.
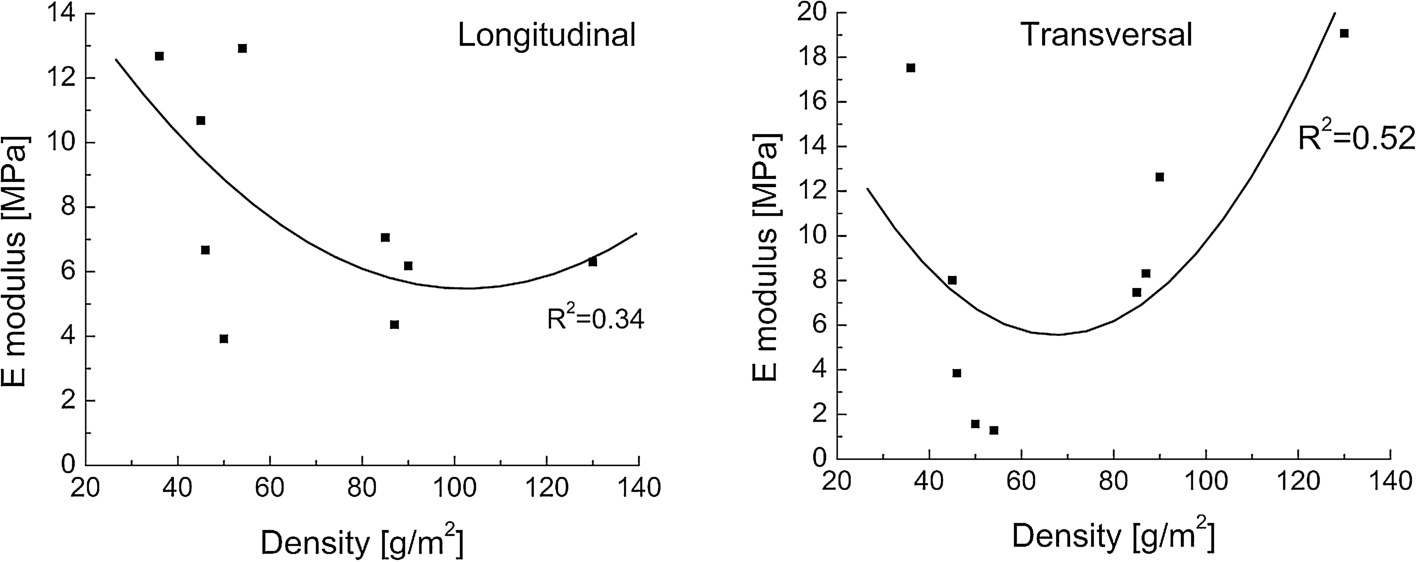
The relationships between modulus of elasticity and density of the meshes in the longitudinal (left) and transversal direction (right).
The relationships between the modulus of elasticity and density of the meshes were evaluated (Fig. 7). The elastic modulus for lightweight meshes in the L direction was in a broad interval 4–13 MPa, while the modulus for standard meshes was in the range 4–7 MPa (Fig. 7(left)). In the transversal direction the elastic modulus for both types of meshes was broader – in the interval 3.8–19.07 MPa (Fig. 7(right)). In the longitudinal direction the prediction of the model was low
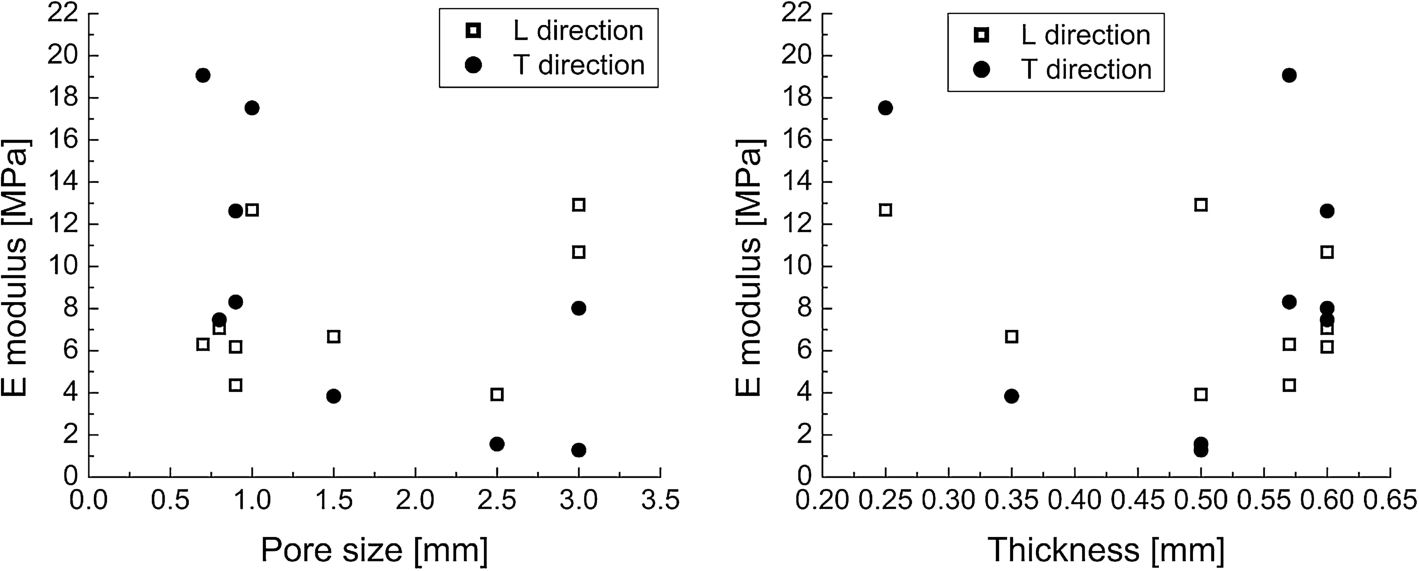
Correlation between pore size of meshes and elastic modulus (left). Correlation between mesh thickness and elastic modulus (right).
The results about the relationships between pore size and elastic modulus revealed that most of the meshes had a medium or large pore size and only three light meshes had a very large pore size (Fig. 8). In the longitudinal direction both types of the meshes had elastic modulus in the range 4–13 MPa while in the transversal direction the elastic modules of standard meshes were between 3 MPa–19 MPa, while lightweight meshes with very large pores were in the narrower range 1–8 MPa.
The meshes exhibited varying thickness, but seven of them were between 0.5–0.6 mm thick. Reducing mesh thickness leads to a fast decrease in elastic modulus.
A biomechanical testing of synthetic graft materials was performed to assess the impact of mesh structure on mechanical compatibility between lightweight, standard hernia meshes and abdominal tissues. Nine meshes were evaluated and compared on the basis of their filament diameter, pore size, density, elastic properties and thickness.
Twenty years ago when Chu et al characterized the mechanical properties of three of the most implantable heavyweight hernia meshes determined that they had one common characteristic – greater strength in the wale direction and greater extensibility in the course direction [19]. Later on it was commonly accepted that conventional standard polypropylene prosthesis such as Surgipro®, should have small pores while light-weight meshes like Vypro II® have to be produced with big pores [13]. Today no clear line exists between mesh properties as demonstrated for the above results. The meshes exhibited varying thickness, pore size and porosity although the study of Coda et al. [1] shows that 72% of the presented standard meshes and 50% of the lightweight meshes have thickness in the range 0.5–0.6 mm.
We demonstrated that the majority of meshes exhibited a marked degree of anisotropy. Only Surgimesh®14 revealed isotropic properties. The differences between mechanical behaviors in perpendicular directions were demonstrated by LO in the range 0.4–2.5 yet for Ultrapro™ the level of orthotropy ratio was 3 times higher than the LO of fascia – 10.09. Of all the tested meshes only Vypro™ II displayed orthotropy similar to that of abdominal fascia – 2.49 versus 2.9 and 3.3.
The actual load on the abdominal wall is an important factor in the selection of hernia mesh. Recent investigations in the abdominal wall strength have revealed that the recommended tensile strength for abdominal wall is 22 N/cm in the cranial/caudal direction and 32 N/cm in the lateral direction [20]. From a strength standpoint only Surgipro™ and TecnoMesh® can be implanted in the abdominal wall as they do meet the physiological requirements of mesh materials according to Zhu et al. [20]. It is likely that these theoretical values rarely arise in vivo but they should be considered by surgeons.
Mesh orientation, stretch at 16 N/cm and 20–40% elongation were also considered as critical in groin hernia surgery [11,13,20]. According to Deeken [3] materials with strain values less than 10–30% at 16 N/cm will stretch less than the native human abdominal wall, while meshes that stretch more than 30% could result in hernia recurrence. It can be supposed that Optilene®, Vypro™ II, Ultrapro™ and Parietex™ will not be suitable for repair of inguinal hernia because at 16 N/cm - they will stretch less than the native human abdominal wall and will result in a more pronounced foreign body sensation or discomfort. Surgimesh®14, Surgipro™, TecnoMesh® however could result in bulging or hernia recurrence. Deformability of the fascia and meshes were compared at both directions. Only TiO2Mesh™ and Ultrapro™ demonstrated deformability close to the mechanical properties of fascia in the longitudinal direction.
The obtained results on ultimate tensile strength showed that Optilene®, TiO2Mesh™, Ultrapro™ and Parietex™ should not be used in case tensile strength above 47 N/cm is required, i.e. – when obese patients are operated.
It was observed that deformability and elasticity of meshes are direction dependent. Their deformation at 16 N/cm load increased with mesh density in the longitudinal direction. Comparisons of the pore size and thickness of light-weight and standard meshes established no clear difference between them. According to Zhu et al. [20] good postoperative results with PP meshes are achieved when a pore size greater than 1 mm is used. The mechanical properties of the fascia and the investigated hernia meshes in the longitudinal and transversal direction were compared to evaluate their mechanical compatibility. There are two lightweight mashes – Vypro™ II and Parietex™ with properties that correspond to those of fascia in both directions. The conclusion is not valid for standard meshes.
The comparison between the elastic properties of the tested standard meshes and human fascia revealed that in the longitudinal direction Surgimesh®14 resembled the elastic properties of the fascia transversalis and umbilical fascia in the same direction, while the elastic properties of the umbilical fascia in the transversal direction were close to the elastic modulus of Surgipro™ and Surgimesh®14 (Fig. 3). It was observed that only two light-weight meshes – TiO2Mesh™ and Ultrapro™ demonstrated deformability similar to deformability at 16 N/cm of the fascia transversalis (Fig. 5).
The investigation has some limitations. We tested light and standard meshes only. A recent survey among surgeons from leading clinics in Bulgaria confirmed that our choice of meshes was relevant to clinical practice in the country. The most preferred meshes were polypropylene ones (51.8% of the surgeons implanted polypropylene meshes only, 25% worked with polypropylene and polyester meshes, and 11% implanted partially absorbable or polypropylene meshes. About 50.5% of the surgeons used standard meshes (70–140 g/m2) and 27% used light and standard ones [21].
Conclusion
This study is our contribution to the efforts of many colleagues in describing the main mechanical properties of hernia meshes.The results demonstrated that the properties of the meshes largely vary because of the impact of the mechanical structure on the mechanical behavior of meshes. The range of ultimate stress was large with the strongest mesh having maximum stress about 4 times than the weakest mesh in the longitudinal direction and 10 times in the transversal direction. The meshes are highly anisotropic except for Surgimesh®14 which is the only isotropic mesh. According to reference values for maximum forces arising in the abdominal wall Optilene®, TiO2Mesh™, Ultrapro™ and Parietex™ meshes are unsuitable for hernia repair for obese patients.
Meshes should be implanted taking into consideration their elasticity and deformability. This is why their structural and mechanical parameters should be mentioned in details by the manufacturing companies on the package or in the user manual.
Footnotes
Acknowledgements
This work is supported by the grant D-82/2017, financed by the Council of Medical Science at the Medical University-Sofia. The authors thank the Institute of Optical Materials and Technologies for their support in the use of equipment of the project BG16 1P0003-1.2.04-0034-C0001 under Operational Program “Development of the competitiveness of the Bulgarian Economy”.
Conflict of interest
The authors have no conflict of interest to report.