
Abstract
INTRODUCTION:
Exogenous Nel-like molecule type 1 (NELL1) represents a potentially attractive clinical treatment option in the orthodontic and other settings because of its osteoinductive and vasculogenic properties.
AIMS:
To explore effects of NELL1on corticotomy-assisted tooth movement and osteogenesis in a rat model.
METHODS:
Thirty Sprague-Dawley rats were divided into 6 groups: Control, Sham, Tooth movement only, Vehicle, NELL1-LD (low-dose NELL), NELL1-HD (high-dose NELL). Human recombinant NELL1 protein was applied locally (Groups NELL1-LD and NELL1-HD) into buccal mucosa region of left first upper molar. Then the distance and velocity of tooth movement was measured, animals at 6 weeks after surgery were sacrificed, and was followed by computed tomography and histochemical staining.
RESULTS:
Both NELL1 groups had higher bone mineral density, greater tooth movement distance and velocity in comparison to the Vehicle group. Proximally and distally, periodontal ligament width was significantly increased in the NELL1-LD and NELL1-HD groups. Decortication enhances remodeling, however, rapid bone formation by high-dose NELL1 may affect bone absorption.
CONCLUSION:
Appropriate dose of NELL1 can be administrated to reduce the total time for tooth movement, and may shorten the treatment time in select populations.
Introduction
Tooth movement induced by orthodontic force application is characterized by remodeling changes in the compression and tension regions, in which osteoblasts and osteoclasts are key cellular effectors [1,2]. There are extensive macroscopic and microscopic changes in bone and adjacent periodontal tissues following exposure to mechanical loading [2,3]. The result is a biochemical adaptive response that includes reorganization of the intracellular and the extracellular matrix, and change in the periodontal tissue vascularity and blood flow in parallel with the synthesis of growth factors, metabolites, cytokines and various enzymes [4,5].
Intervention with alveolar corticotomy has demonstrated accelerated orthodontic tooth movement by promoting remodeling concomitant with an increase in Receptor activator of nuclear factor kappa-b ligand (RANKL) levels [1]. RANK and its ligand, RANKL, regulate osteoclast formation and activation, and these mechanisms underlie the osteoresorptive effect of some hormones and cytokines [6]. Conversely, bone morphogenetic protein (BMP)-2 is an osteoinductive factor widely used in human surgery. In the dental setting, BMP-2 has been successfully used in alveolar defects in animal models and in clinical orthodontic tooth movement [7,8]. However, emerging safety concerns including the risk of uncontrolled bone formation, bone resorption, immunogenicity, and malignancies have yet to be fully characterized [9].
Exogenous Nel-like molecule type 1 (NELL1) represents a potentially attractive clinical treatment option in the orthodontic and other settings because of its osteoinductive and vasculogenic properties demonstrated in bench studies and animal models [10–12]. Unlike the BMPs, NELL1 is highly specific to the osteochondral lineage and avoids undesirable pleiotropic effects.
The goals of this study are to explore whether applying NELL1-containing collagen membranes facilitates tooth movement and osteogenesis, and to investigate the effects of NELL1 on bone formation and bone resorption in a rat model of augmented corticotomy-assisted orthodontics.
Methods and materials
This study was carried out in strict accordance with the recommendations in the guidelines of the Department of Experimental Animals, China Medical University, Liaoning, China. The protocol was approved by the Committee on the Ethics of Animal Experiments of Sheng Jing Hospital, affiliated to China Medical University.
Experimental animals
Thirty 6-week-old Sprague-Dawley rats (males weighing 180–200 g) were divided into 6 groups for the 6-week experiment (Table 1). Several animals died during the study, resulting in n = 5 for Control, Group S, Group TM only groups, and n = 4 for Group V, NELL1-LD, NELL1-HD groups. The animals were acclimatized for at least 1 week before the start of the experiment and housed under normal laboratory conditions, with access to powdered laboratory chow and water ad libitum. All animal procedures were performed under general anesthesia and with the permission of the Institutional Animal Care and Use Committee (IACUC) of Jiao Tong University School of Medicine, Shanghai, China.
Total experimental sample and group distribution
Total experimental sample and group distribution
∗ N = 5 for 6 groups for total 30 animals. Several animals died during experiment, resulting in n = 5 for Control, Group S, Group TM only groups; n = 4 for Group V, NELL1-LD, NELL1-HD groups. 1Animals in the sham surgery group underwent anesthesia up to the creation of flaps. No corticotomy was performed and the flaps were closed without any filling materials. 2Animals in the vehicle group received lank collagen membrane soaked in saline.
A full-thickness triangular mucoperiosteal flap was raised in select groups (Group S, sham surgery; Group V, corticotomy plus vehicle; Group NELL1-LD, corticotomy plus low-dose NELL1; Group NELL1-HD, corticotomy plus high-dose NELL1) by making an incision from the gingival sulcus on the mesial surface of the left maxillary first molar and extending it 5 mm to the soft tissue space inferior to the gap between molars. Alveolar decortication (Group V; Group NELL1-LD, and Group NELL1-HD) was performed according to the method reported by Baik et al. [13]. The surgical design consisted of performing apical-occlusal cuts (0.3 mm deep) to the buccal cortical bone around the left first molar under water irrigation. A low-speed hand drill with fine fissure bur was used. Hemostasis was achieved with manual compression and placement and compression of collagen membranes. The collagen membranes were fixed to the buccal surface and the lifted mucoperiosteal flap was sutured.
Tooth movement appliance and measurement
Experimental tooth movement was performed using a method previously describe [14,15]. In brief, experimental force was applied in select groups (Group TM, Group V; Group NELL1-LD, and Group NELL1-HD) by means of a preformed 25-g force nickel-titanium closed-coil springs (Rocky Mountain Orthodontics. Denver, CO) placed between the upper left first molar and upper central incisor under general anesthesia. A band with cleat was placed around the first molar with ligature wire attached to the cleat. Self-cure resin was used to bond the spring to the mesial aspect of the left first molar cleat ligated with a 0.008-inch twisted stainless steel ligature wire. The other side of the spring was ligated through grooves in the maxillary incisors drilled laterally immediately above the gingival papilla with a round bur. A steady medially directed force was applied to the upper first molar. An illustration of the surgical procedure and placement of the device is shown in Fig. 1.
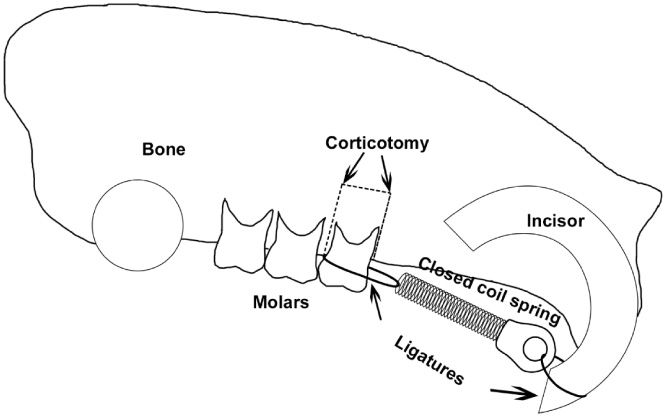
Illustration of the surgical procedure and placement of the device.
Human recombinant NELL1 protein (Cat. no. H00004745-P01, Abnova, Taipei, Taiwan) was applied locally (Group NELL1-LD and Group NELL1-HD) into the buccal mucosa region of the left first upper molar using absorbable collagen sponge (ACS) and collagen membrane. NELL1 was reconstituted with concentrations adjusted to 100 ng/μl (Group NELL1-LD) and 300 ng/μl (Group NELL1-HD) by adding phosphate buffered saline (PBS). Commercially available ACS was cut into 3-mm pieces with a biopsy punch and irradiated with UV light for 2 hours after which NELL1 was loaded onto the sponges by soaking in reconstituted NELL1 solution (∼15 μl). Similarly prepared Geistlich Bio-Gide collagen membrane was impregnated with 15 μl NELL1 solution to carry 1.5 μg (Group NELL1-LD) and 4.5 μg (Group NELL1-HD) of the recombinant human NELL1 protein. (Note: to avoid variation due to brand, size, humidity, etc., the maximum allowable NELL1 absorbed by a collagen membrane sample was ≤5 μg as measured under the operating condition of the laboratory).
Experimental design
Overall the experimental order was as follows: (1) measure distance and velocity of tooth movement on animals; (2) sacrifice of animals at 6 weeks after surgery, followed by CT imaging; and (3) subsequent Hematoxylin and Eosin (H&E) staining.
Tooth movement
Tooth movement was measured weekly from 1 to 6 weeks post-surgery by computing the distance between the most distal contact point of the maxillary left first molar and the most mesial contact point of the second molar. The distance was directly measured on animals with velocity defined as distance/time. Tooth movement distance was measured during 4 periods: Day 0–3, Day 3–7, Day 7–14, and Day 14–28. Tooth movement distance (and velocity) was measured as 0 in both Control and Group S. Comparisons were made among Group TM, Group V, and Groups NELL1-LD and NELL1-HD groups.
Micro-computed tomography (CT) imaging
Rats were sacrificed 6 weeks after surgery. The maxilla was harvested and fixed with 10% neutral buffered formalin for 48 hours after which micro-CT images were recorded. CT imaging was conducted only one time, at 6 weeks after surgery. Through the CT images, the following measurements were collected: (1) thickness of the periodontal ligament (PDL); and (2) bone analysis for each volume of interest (VOI). All measurements were repeated three times and the average value calculated. The sagittal plane of the entire maxilla was imaged to clearly exhibit changes in tissues.
The thickness of the PDL at the mesial and distal sides of the mesial root of the first molar was measured. In addition, analysis for each VOI of 500 μm3 of alveolar bone on the mesial and distal sides were analyzed. Bone analysis included bone volume (BV); bone volume fraction (BV/TV), defined as the ratio of BV to total volume (TV; 500 μm3); bone marrow density (BMD); and bone marrow content (BMC).
Histology and immunofluorescence
After CT imaging and the relevant measurements, the maxilla samples were subject to Hematoxylin and Eosin (H&E) staining. Five untreated rats were sacrificed to provide baseline controls for histological analysis. Maxillae were resected around the maxillary left first molar from the mesial contact point of the second molar to two-times the distance of tooth movement on the mesial side of the first molar to create an asymmetric sample. The tissue sample was immediately immersed in fixative solution overnight at 4 °C. Tissue blocks were subsequently decalcified using 10% ethlylene diamine tetraacetic acid (EDTA) in phosphate buffered saline (0.01 mol/L, pH 7.4) at 4 °C for 4–6 weeks.
After decalcification, the samples were processed and embedded in paraffin. Serial 5.0-μm thick sections were prepared perpendicular to the long axis of the distal root of the maxillary first molar, and sectioned from the side of the roots. A total of 12 slices in the middle region of the roots were prepared to have three replicates for each staining. H&E staining followed standard protocol.
Statistical analysis
Micro-CT measurements, teeth movement (including distance and velocity), periodontal ligament width, and alveolar bone crest (ABC) to cementoenamel junction (CEJ) distance analysis for Control, Group S, Group TM, Group V, and Groups NELL1-LD (NELL1 1.5 μg) and NELL1-HD (NELL1 4.5 μg) were represented as mean ± standard deviation (SD) for each group for Control, Group S and Group TM (each n = 5) as well as Group V and Groups NELL1-LD and NELL1-HD (each n = 4). Differences among groups were compared using one-way ANOVA test with a Bonferroni test for post-hoc pair-wise comparisons. Additionally, one-sample t-test was performed for distance of teeth movement for Group TM, Group V, Group NELL1-LD and GroupNELL1-HD as compared with either Control or Group S (mean value of 0). All statistical assessments were two-tailed and considered significantly different as p < 0.05. All statistical analyses were carried out with IBM SPSS statistical software version 22 for Windows (IBM Corp).
Results
Micro-CT measurements
As shown in Fig. 2, Group TM and Group V had significantly lower BMD than Control (p < 0.01 versus Group TM; p < 0.001 versus Group V) and Group S (p < 0.001 versus Group TM; p < 0.001 versus Group). Group NELL1-LD and Group NELL1-HD had higher BMD than Group V (all p < 0.001) (Fig. 2A). Results were similar for bone volume fraction, with Group TM and Group V having significantly lower BV/TV ratio than Control (p < 0.001 versus Group TM; p < 0.001 versus Group V) and Group V lower than Group S (p < 0.001 versus Group V). In addition, Group NELL1-LD and Group NELL1-HD had higher BV/TV ratio than Group V (all p < 0.001) (Fig. 2B).
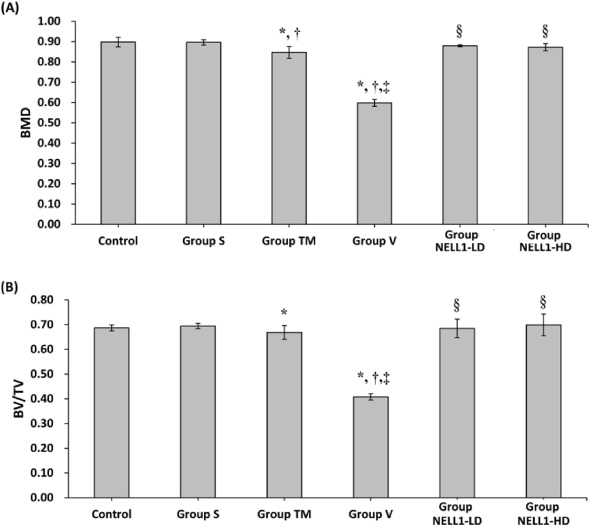
(A) bone mineral density, and (B) bone volume fraction (BV/TV) results. Data presented as mean ± SD for each group (n = 5 for Control, Group S and Group TM; n = 4 for Group V and Groups NELL1-LD and NELL1-HD). ∗†‡§ P <0.05, significantly different compared to ∗Control, †Group S, ‡Group TM, and §Group V.
Tooth movement distance was significantly greater in Group V, Group NELL1-LD and Group NELL1-HD than Group TM in the tooth movement group during the Day 0–3 and Day 3–7 (all p < 0.001) (Fig. 3A). During the period Day 7–14, the high-dose NELL1 group had significantly less movement distance than Group TM, Group V, and the low-dose NELL1 group (all p < 0.001); during period Day 14–28, the NELL1 high-dose group had less teeth movement distance than Group V and NELL 1 low-dose group (all p < 0.001).
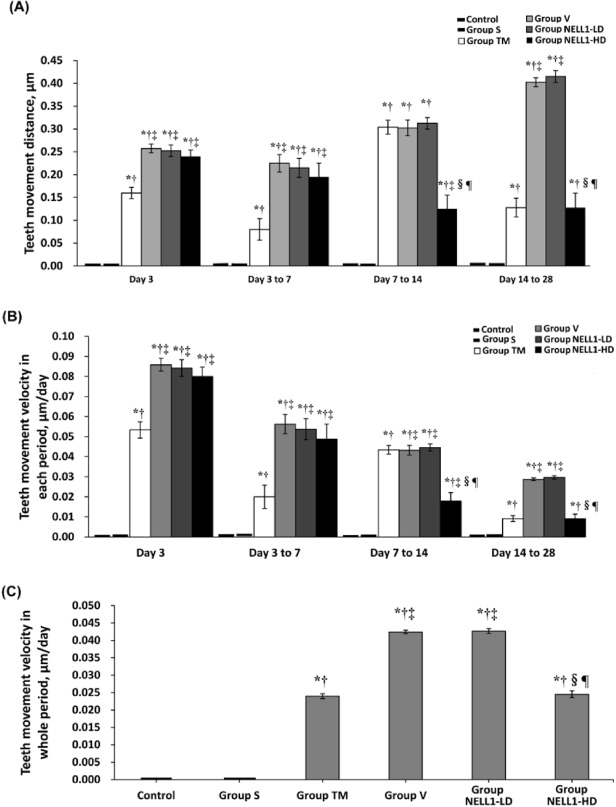
(A) Distance of tooth movement, (B) velocity of teeth movement in each period, and (C) velocity of teeth movement in entire study period (C). Data were presented as mean ± SD for each group. (n = 5 for Control, Group S and Group TM; n = 4 for Group V and Groups NELL1-LD and NELL1-HD). ∗†‡§¶ P < 0.05, significantly different compared to ∗Control, †Group S, ‡Group TM, §Group V, ¶NELL1-LD.
For tooth movement velocity, Group V, and Group NELL1-LD and Group NELL1-HD all showed greater velocity than Group TM during Day 0–3 and Day 3–7, periods (all p < 0.001). Group NELL1-HD had lower velocity than Group V and Group NELL1-LD during Day 7–14 and Day 14–28 periods (all p < 0.001) (Fig. 3B). For the entire period (Day 0–28), Group V and Group NELL1-LD had significantly higher velocity compared to Group TM (both p < 0.001). Additionally, the NELL1 high-dose group had lower velocity versus Group V or the low-dose NELL1 groups (both p < 0.001) (Fig. 3C).
Proximally, the PDL width was significantly decreased in Group TM, but increased in Group V, and Groups NELL1-LD and NELL1-HD compared to with the Control group and Group S (all p < 0.001) (Fig. 4A). Furthermore, the PDL width significantly increased in Group V, and Groups NELL1-LD and NELL1-HD compared to Group TM (all p < 0.001). Regarding the distal aspect, PDL width was increased in Group TM, Group V, Group NELL1-LD, and Group NELL1-HD versus the Control group and Group S (all p < 0.001) (Fig. 4B). Additionally, PDL width was increased in Group V, Group NELL1-LD, and Group NELL1-HD compared to Group TM (all p < 0.001).
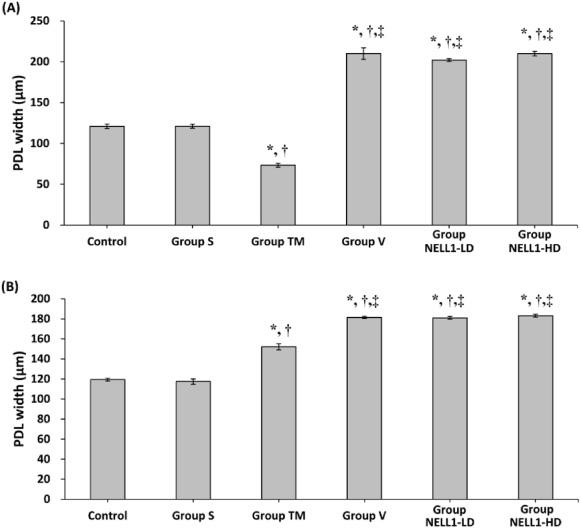
(A) Proximal and (B) distal periodontal ligament width. Data were presented as mean ± SD for each group (n = 5 for Control, Group S and Group TM; n = 4 for Group V and Groups NELL1-LD and NELL1-HD). ∗†‡ P < 0.05, significantly different compared to ∗Control, †Group S, ‡Group TM.
At both sites (proximal and distal), the vehicle group had significantly higher alveolar bone height compared with Control, Group S, and Group TM (all p < 0.001) (Fig. 5A, B). In addition, both Group NELL1-LD, and Group NELL1-HD groups significantly lower CEJ to ABC distance compared to Group V (all p < 0.001). There was no significant difference between Group NELL1-LD, and Group NELL1-HD.
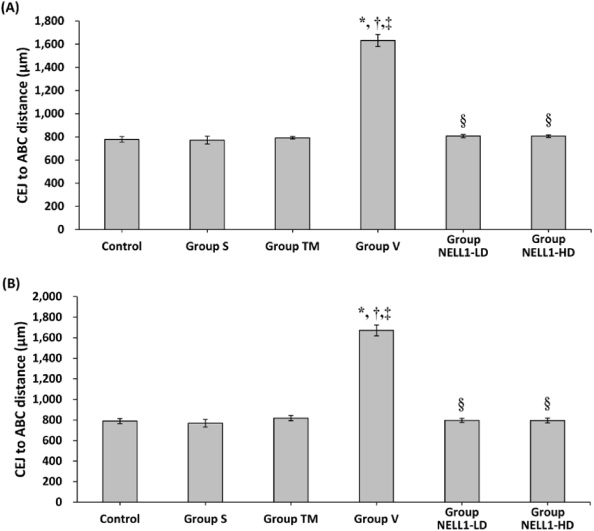
(A) Proximal and (B) distal CEJ to ABC distance. Data were presented as mean ± SD for each group. (n = 5 for Control, Group S and Group TM; n = 4 for Group V and Groups NELL1-LD and NELL1-HD). ∗†‡§ P < 0.05, significantly different compared to ∗Control, †Group S, ‡Group TM, and §Group V.
H&E staining did not show marked differences between groups associated with tooth movement (Fig. 6A). This possibly reflected reflecting inconsistent selection of plane samples due to tooth movement and variation in depth (Fig. 6B). There were discernable differences between select groups in the contact plane between the PDL of the upper left fist molar and alveolar bone. In the Control group and Group S, the contact plane between the PDL and the alveolar bone was smooth, whereas finger-like projections characteristic of bone remodeling extended into the alveolar bone in other groups. This phenomenon was especially conspicuous in the Group S, Group NELL1-LD, Group NELL1-HD. In the Group NELL1-LD and Group NELL1-HD, no alveolar bone was observed between roots on the buccal side near the site of decortications. In Fig. 7, the green ‘P’ marks the conspicuous finger-like projection in the Group TM, Group V, Group NELL1-LD, and Group NELL1-HD.

(A) Upper left-side hematoxylin and eosin stained sections by group (10× magnification). The range of the first molar is indicated by the red indicator above the image. (B) Diagram of the effects with respect to the tangential plane and depth.
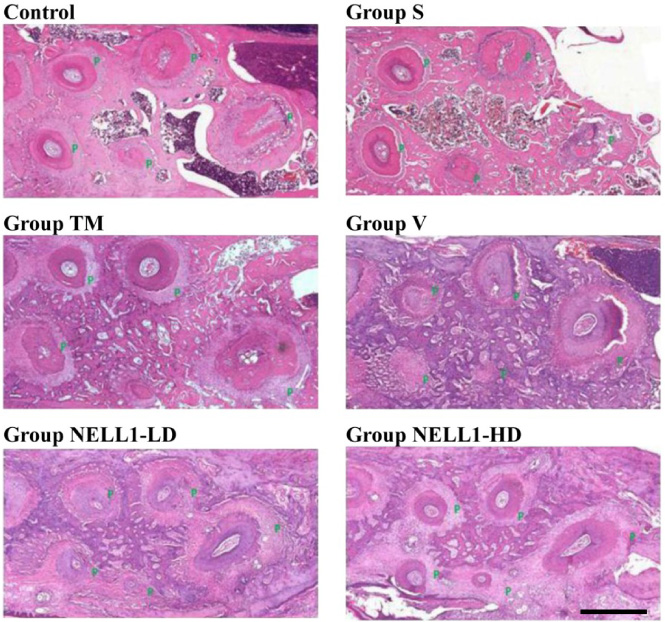
Hematoxylin and eosin staining of the contact plane between the PDL of the upper left first molar and the alveolar bone by group (40× magnification). Images are enlarged images of those presented on the right side of Fig. 6A. The scale bar in the right lower image = 1000 μm.
Based on representative micro-CT images, low-dose NELL1 did not inhibit tooth movement; bone formation caused by NELL1 did not affect bone absorption associated with tooth movement (Fig. 8). Tooth pulp loss caused by decortication was moderately compensated.
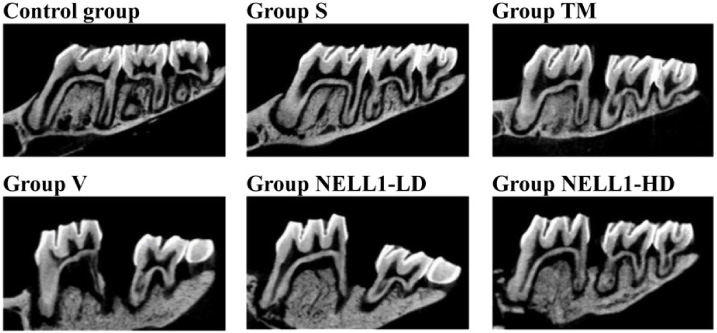
Representative CT images of the tooth root of the upper left first molar.
The current investigation evaluated the effects of NELL1 on corticotomy-assisted tooth movement and osteogenesis in a rat model. We found that treatment with high and low doses of NELL1 was associated with increased bone mineral density and bone fraction volume in the targeted region compared to vehicle. Tooth movement distance and velocity were greater with high- and low-dose NELL1 than with tooth movement alone in the early post treatment periods; however, high-dose NELL1 appeared to impede tooth movement over time. Consistent with tooth movement and remodeling, PDL width was increased in the high- and low-dose NELL1 groups compared to control on the compression (proximal) and tension (distal) sides.
Orthodontic tooth movement involves the periodontal tissues and alveolar bone and the ordered release of numerous substances from the dental tissues and surrounding structures. Remodeling changes in the compression and tension regions occur in which osteoclasts and osteoblasts are key cellular effectors [1,2] with bone resorption on the compressed side and bone formation on the tensile side. The mechanical stress loaded by orthodontic forces is transduced to cells in the PDL, which regulate resorption and formation of bone by signaling surrounding cells [2,3,16,17]. The result is a biochemical adaptive response including reorganization of the intracellular and extracellular matrix, and change in the periodontal tissue vascularity and blood flow in parallel with the synthesis of growth factors, metabolites, cytokines and various enzymes [4–6].
Corticotomy-assisted orthodontic treatment has been described in numerous reports with efficacy demonstrated in the clinical setting [18–22]. The procedure is performed to induce increased tissue turnover and a transient osteopenia, with consequent higher rate of orthodontic tooth movement [20,22]. The current authors have reported the successful application of augmented corticotomy-assisted orthodontics in the treatment of patients with Class III malocclusion [19,20].
In this procedure, the host site is decorticated to establish bleeding points in the cortical bone. When orthodontic force is applied, an acute inflammatory reaction takes place in the periodontium coincident with the mechanical responses [23]. Capillary vasodilatation promotes the migration of leucocytes into the periodontal tissue, where they synthesize and secrete proinflammatory cytokines and chemokines, growth factors and enzymes. Intensified osteoclastic activity results in transient bone resorption thereby providing a window for orthodontic movement.
The biological basis of this procedure is mediated by accelerated bone turnover (i.e., regional acceleratory phenomenon) in which osteoclastic activity results in osteopenia and increased bone remodeling involving simultaneous increase in RANKL levels [1,20,22,24–26]. RANKL and its receptor RANK regulate osteoclast formation and activation, through which many hormones and cytokines produce their osteoresorptive effect6. RANKL is expressed on the surface of cells, such as osteoblast cell lineage, which can support osteoclastogenesis [27]. RANKL signaling is inhibited by osteoprotegerin (OPG) [28], and the balance between RANKL and OPG mediates bone resorption [29]. Thus, bone remodeling is reflects a balance between RANK-RANKL binding and OPG production [6].
A number of reports have described the pharmacological induction of tooth movement by enhancement of osteoclastogenesis through local administration of prostaglandins [30], vitamin D3 [31]. Osteocalcin [32], or parathyroid hormone33. Prostaglandin E2, for example, may induce osteoclastogenesis through the prostaglandin E receptor subtype 4 (EP4) via increased RANKL and cyclic adenosine monophosphate in osteoblasts [34]. Conversely, other reports have described local administration of the osteoinductive substances, such as BMP-2, and successful orthodontic tooth movement in animal models [7,8,35].
Exogenous NELL1 represents an attractive therapeutic approach in orthodontic tooth movement because of its osteoinductive and vasculogenic properties [36]. This potent growth factor stimulates ameloblast and osteoblast differentiation and mineralization, and promotes cross-talk between osteoblasts and osteoclasts [37]. It may also play a role in the secretion and mineralization of the extracellular enamel matrix and root formation [38]. Because it is highly specific to the osteochondral lineage, NELL1 avoids the undesirable pleiotropic effects associated with BMP-2.
The present study reported findings on the use of NELL1-containing collagen membranes in a rat model of augmented corticotomy-assisted orthodontic tooth movement. Not surprisingly given its osteoinductive potential, both groups receiving NELL1 had significantly greater bone mineral density and bone mineral fraction (all p < 0.001) than the vehicle group without NELL1 application.
Decortification clearly promoted tooth movement as the vehicle and both NELL1 groups exhibited significantly greater movement than the tooth movement only group (all p < 0.001). Tooth movement distance and velocity were significantly greater in both NELL1 groups than in the tooth movement alone group during Day 0–3 and Day 3–7 (all p < 0.001). These parameters were similar in the low-dose NELL1 and vehicle groups, but were comparatively lower in the high-dose NELL1 group one week after treatment possibly reflecting increasing osteoinduction. Periodontal ligament width widened in the NELL1 groups more than in the tooth movement alone group, and both NELL1 groups had significantly lower alveolar bone height (all p < 0.001) than the vehicle group.
Hematoxylin and eosin staining did not show marked differences between groups possibly due to inconsistent selection of planes samples. Although the original study design took the occlusal surface as the reference surface, the selected planes of various samples might not have been consistent because of the gap between the anterior and posterior tooth planes produced during tooth movement. In addition, different results may have been obtained at different depths.
Conclusions
There was an observable enhancement in tooth movement distance and velocity with decortification and low-dose NELL-1 compared to tooth movement alone. Higher dose NELL1 appeared to have an inhibitory effect on tooth movement with time. Study measurements and imaging suggests that appropriate doses of NELL1 can be administrated during tooth movement to reduce the total time required by the tooth movement, and may shorten the treatment time in select populations such as patients with type II diabetes.
Footnotes
Acknowledgements
This study was supported by the Youth Research Fund of Shanghai Municipal Commission of Health and Family Planning (20144Y0125) and the Science and Technological Fund of Shanghai Jiao Tong University School of Medicine (12XJ10055).
Conflict of interest
None to report.