
Abstract
For medical devices directly or indirectly contacted with blood, hemocompatibility assay is of great importance during the biological evaluation. In ISO 10993-4:2017 - Biological evaluation of medical devices part 4, a selection of tests for interactions with blood is given with the rationale for selection of tests based on their intended use specified, however, the specific testing protocols may vary significantly when performing the hemocompatibility assays. In recent years, medical catheters have been widely used in clinical practice. Moreover, a lot of surface modified catheters emerged in the market to enhance their performance of hemocompatibility especially for hydrophilic coating catheters. Unfortunately, to date, the hemocompatibility of hydrophilic coating still remains controversial due to the inherent complexity of the hemocompatibility test itself and lack of validated test methods. In this study, through determining the hemocompatibility performance for a micro-catheter with a typical hydrophilic pyrrolidone coating regarding haemolysis test, partial thromboplastin time (PTT), prothrombin time (PT) and thrombogenicity test in dogs, we have established a series of tentative hemocompatibility protocols for these tests. Hopefully, our study could not only provide some useful information for hemocompatibility evaluation on medical catheters with a hydrophilic coating but could also contribute to the development of neo-type hemocompatible medical devices for better clinical practice.
Introduction
When in contact with blood, cardiovascular biomaterials and medical devices may trigger a series of complex biological reactions involved in cell components, factors and proteins in the blood, and then cause potential health risks such as haemolysis, coagulation and thrombosis. Hemocompatibility tests should therefore always be performed before their clinical application [1,2]. Due to the design, material composition, intended use, application environment of the biomaterials and medical devices should be considered during the selection and design of hemocompatibility tests, therefore, how to reach a sound consensus for the scientific and effective hemocompatibility assay is still a worldwide problem [3–5].
Micro-catheters have now been widely used to deliver the contrast agent or drug to the designated part of the vascular system during clinical interventional operation. In order to enhance their performance of hemocompatibility, a lot of surface modified catheters have been recently developed and released in the market, and hydrophilic coating catheters in particular. Some studies have already proved that this hydrophilic surface modification could improve hemocompatibility of the indicated devices by reducing mechanical friction, protein adsorption and platelet adhesion [6–8]. Furthermore, others claimed that hydrophilic heparin coating may have better hemocompatibility performance due to its anticoagulant ability to selectively adsorb plasma protein [9–11].
In the present study, we focused on hemocompatibility tests in terms of haemolysis, partial thromboplastin time (PTT), prothrombin time (PT) assay and thrombogenicity tests in dogs of a kind of typical micro-catheter with a hydrophilic pyrrolidone coating. We have established some tentative standard operation practices for these test methods. Hopefully, our study could not only provide some useful information for hemocompatibility evaluation on medical catheter with a hydrophilic coating, but could also contribute to the development of neo-type hemocompatible medical devices for better clinical practice.
Materials and methods
Materials
Legally marketed miro-catheters with hydrophilic pyrrolidone coating and comparator coated micro-catheter were obtained from commercial sources. The black rubber was purchased from Sigma Company. The scan electron microscopy (SU8010) and spectrophotometer (U-3900H) were both purchased from Hitachi Limited, Japan.
Animals
Adult male Beagle dogs (15 kg–20 kg) and adult male rabbits (200 g--300 g) were purchased from the Shandong Jinfeng Animal Center. The animals were housed in stainless steel cages and identified by collar tags. The temperature of the room was within a range of 20 °C–26 °C. The humidity range of the room was 30%–70%. All animal-related procedures were approved by the Institution Committee of Ethics in Animal Experimentation.
Haemolysis test
Briefly, rabbit blood is freshly collected in anticoagulation tubes. 8 ml of the pooled whole rabbit blood was diluted sufficiently in 10 ml of physiological saline (SC). The test article was prepared based on a ratio of 2 g was covered with 10 ml of SC in triplicate, all tubes were incubated in a (37 ± 1) °C water bath for approximately 72 h ± 2 h. Negative control was prepared by 10 ml in triplicate and positive control was prepared as 10 mL portion of distilled water in triplicate. Then, based on the ratio of 0.2 mL diluted blood/10 mL test solution, the diluted blood was added to all the tubes. Maintain tubes for another 60 min at (37 ± 1) °C in a water bath. After incubation, the solutions of all tubes were collected and centrifuged for 5 min at 800 g. Finally, the absorbance of each supernatant was determined by the spectrophotometer at 545 nm. The mean of the three readings for the test article, negative and positive controls was calculated respectively. The average of negative controls should be less than 0.03 and the positive controls should be within 0.8 ± 0.3. The haemolytic rate was calculated as:
HR — the haemolytic rate of test article, %
A — the absorbance value of test article group
B — the absorbance value of negative control group
C — the absorbance value of positive control group.
For PTT assay, briefly, the test article and positive control (black rubber) were placed, in six replicates, in polypropylene tubes and then the appropriate volume of citrated normal human plasma was added to each tube and exposed for (1 ± 0.1) h at (37 ± 1) °C, 60 rpm in water bath. The negative group was treated with the same way. At the end of the exposure period, the plasma was removed from the tubes and placed in new test tubes. The plasma samples were maintained in an ice bath until the PTT values of all tubes were determined. The average coagulation times were calculated for the test article, positive and negative controls. The percentage in the mean PTT value of the test article and the positive control compared to the negative control were calculated following ASTM F2382 criteria, as shown in Table 1 [12]. For PT assay, the positive control was set up based on the ratio of 200 mg:20 mL, a 20 mg portion of the Oxalic Acid was covered with 2 mL of citrated human plasma and then incubated at (37 ± 1) °C for (1 ± 0.1) h with agitation at 60rpm and then the PT values were determined. Normal PT is within 10 s–14 s, if the mean value for the negative control exceeds this range by ±1 second, the study will be considered invalid.
Acceptance criteria for coagulation of test articles
Acceptance criteria for coagulation of test articles
Briefly, a 14-gauge venous catheter was percutaneously placed in the animal’s left cephalic vein and connected to an IV drip with 0.9% normal saline at first. The animal was then sedated with 10 mg/kg of ketamine and 0.04 mg/kg of atropine intramuscularly. All the animals underwent endotracheal intubation, maintenance of the anesthetic plan with isoflurane and monitoring of their heart rhythms, heart rates, and oxygen saturation. The neck region was shaved and scrubbed with povidone iodine. A simple cut-down procedure was performed to expose each jugular vein. The test article and control article were threaded down the right jugular vein and the left jugular vein, respectively. The portion of the article outside the vessel was anchored to the skin using sutures. For both insertion sites, the exposed tissues were partially closed to prevent excess drying. At approximately 4 hours after insertion, each dog was systemically heparinized by intravenous injection of heparin sodium at approximately 50 U/kg body weight to prevent post-mortem clotting. After 5 min, but not more than 15 minutes, each dog was exsanguinated and the jugular veins with test or control articles were dissected free and removed. The test and control articles and associated vessel were examined for evidence of thrombus formation. The extent of thrombus formation is outlined in Table 2.
Scoring system for thrombus formation
Scoring system for thrombus formation
The location of the thrombus formation (on the vessel wall or the device) was recorded and representative photographs were taken and the weight of each thrombus was also recorded. Differences between test and control articles were based on examination of the scores and photographs. Usually, scores 0–2 were considered passing.
The micro-catheter samples were analyzed by a low-power scan electron microscopy (SEM) to demonstrate the microscopic surface changes before and after thrombogenicity assay under the instruction [13]. Briefly, the test sample was rinsed and fixed with 0.1 M PBS and 0.1 M phosphate-buffered 1.25% glutaraldehyde for 2 h on ice. After fixation, the samples were cut to about 3 cm pieces and post-fixed with similarly buffered 2% osmium tetroxide and then rinsed with PBS three times. The samples were treated by dehydration in ethanol, immersion in t-butanol and lyophilization. Finally, the surface was sputter-coated with gold ion then under observed.
Statistical analysis
The significance of the differences between different groups and controls was analyzed by the Student’s t-test. p < 0.05 was regarded as significant.
Results
Haemolysis assay
The haemolytic rate of the micro-catheter with hydrophilic coating was determined by the spectrophotometer at 545 nm. The results have shown that the haemolytic rate for micro-catheter with hydrophilic coating was 0.2%, which could meet the evaluation criterion of the medical devices that the haemolytic rate should be less 5% [14], as demonstrated in Fig. 1.
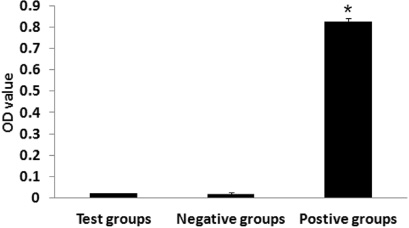
Results of haemolysis assay. The haemolysis property of the miro-catheter samples were determined based on the 5 g/10 ml ratios using diluted blood prepared from human red cells and the haemolytic rate is calculated according to the specified equation (n = 3). ∗ p < 0.05 means significant differences between positive groups and test groups.
We then performed the PTT and PT assay in accordance with the method above. As is shown in Fig. 2A, the PTT results of the test article exhibited no significant differences with the negative control. At the same time, the percentage in the mean PTT value of the test article and the positive control compared to the negative control were 90.4% and 40.6%, respectively. Both the test article and the positive control meet the acceptance criteria of PTT and the test article could be regarded as a minimal activator of intrinsic coagulation pathway. Additionally, the average PT value for the test article (13.1 seconds) and negative control (13.0 seconds) were also within the normal range for the coagulation functioning ability of prothrombin (10.0 to 14.0 seconds) and there was no coagulation in the positive groups. Statistical analysis indicates that there was no significant difference between the PT values of the test article and the negative control.
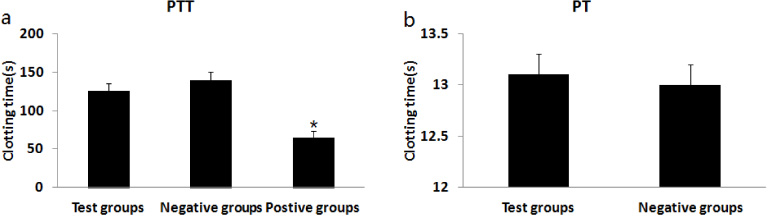
PTT (a) and PT (b) values of all tubes were determined. The percentage in the mean PTT value of the test article and the positive control compared to the negative control were calculated following ASTM F2382 criteria. The clotting time of the plasma solution is recorded with a chronometer. The tests are repeated three times for each six parallel groups.
In vivo thrombogenicity test using dog jugular vein models were performed to determine the thrombus formation of micro-catheter after 4h application. The results have shown that of all three micro-catheter samples exhibited minimal clotting at multiple locations, that is, slight thrombosis which equals 2 points. For the comparator control micro-catheter, the points were 2, 2 and 2, respectively. The average weight of the thrombus from the micro-catheter with hydrophilic pyrrolidone coating was 0.169 ± 0.05 (g), compared with the comparator control, which was 0.098 ± 0.03 (g) (see Fig. 3).

Results from the thrombogenicity study using jugular veins of the dogs. (a) Photographs of the thrombus from three micro-catheter samples after 4h application. (b) Photographs of the thrombus from three comparator micro-catheter samples after 4h application. (c) The averaged thrombus weight of test samples and the comparator control. There was no significant difference between test samples and the comparator control (p > 0.05).
The surface of the micro-catheter sample was observed by SEM to evaluate fibrin deposition, leukocyte and platelet adhesion scenarios before and after thrombogenicity assay. The result showed that the surface of the micro-catheter overall looked smooth before insertion in the vessel, as is shown in Figs 4a and 4b. However, the high magnification images showed that there was a lot of fibrin deposited on the surface of the micro-catheter since the coating surface has become discontinuous after 4h constant contacting with the blood (see Figs 4c and 4d).
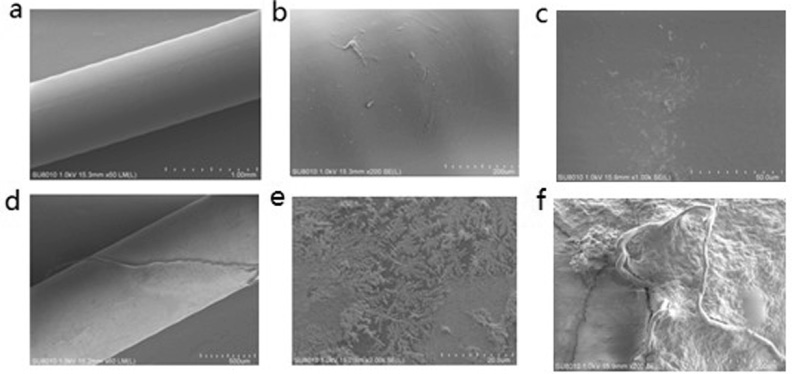
SEM images of the surface of micro-catheter before insertion (a, b, c) and after 4h in vivo application (d, e, f), respectively.
In recent years, micro-catheters with hydrophilic coating have been widely used in clinical practice. Based on ISO 10993-4:2017, micro-catheters are classified as external communicating devices directly contacting circulating blood, therefore, a series of in vitro and in vivo tests should be performed to evaluate the hemocompatibility performance, including haemolysis assay, coagulation assay and thrombogenicity assay. However, different facilities may hold different visions with the hemocompatibility tests available so far. Typically, the presence of haemolysis usually indicates that the material may induce red cell lysis to the patients in clinical use. In our study, the haemolytic rate of the micro-catheter test sample is 0.2%, that is, less than 5% evaluation criterion, which means that test sample have no hemolytic potential when contacting with circulating blood (see Fig. 1).
PTT is the clotting time of citrated normal human plasma exposed to medical materials. A shortened PTT following contact with a material indicates activation of the intrinsic coagulation pathway of blood coagulation [10]. PT is also regarded as an indicator of the extrinsic pathway activation. In parallel with PTT, a prolonged PT represents an enhanced anticoagulant activity of biomaterials and medical device [15,16]. In this study, the percentage in the mean PTT value of the test article compared to the negative control was 90.4%. It was concluded that the micro-catheter had a minimal effect on intrinsic coagulation pathway. The average PT value for the test article was 13.1 seconds and negative control was 13.0 seconds. Both values were within the normal range for the coagulation functioning ability of prothrombin (10.0 to 14.0 seconds), which indicates that the test article was not a robust activator of extrinsic coagulation pathway.
For a given medical device contacting with circulating blood, in-vivo thrombogenicity assay is one of the most important performance that should be evaluated. To date, 4-hour dog model has been considered as a robust method regardless of specie of dogs, the acceptance criteria, and the use of anticoagulant since 1980’s. In this study, the thrombogenicity scores of the three test articles were 2, 2 and 2 respectively while the comparator controls were 2, 2 and 2. The results showed that there were no obvious difference between the test article and the comparator control.
Furthermore, we investigated the device-biological interface of the test article using SEM, due to SEM has the advantage providing greater detail about fine structure of components being examined at the intact material/device-biological interface [17]. Results have shown that there were a lot of fibrin and leukocyte and platelet adhesion with the destructive coating surface of the test article after 4h application, which could mainly contribute to the thrombus formation. In addition, since the type and concentration of anticoagulant could influence the results of hemocompatibility assay, therefore, the use of anticoagulants in in vivo and ex vivo hemocompatibility tests should always be avoided unless the device is designed to use under anticoagulant circumstance. Our previous study demonstrated there was no thrombus formation when the dogs were heparinized during the test which fully simulated the actual clinical practice (data not shown). These also provided us a useful way to interpret the results from in vitro and in vivo hemocompatibility assay for biomaterials and medical devices ready to be released in the market.
In conclusion, our studies have established a series of methods for hemocompatibility assay of a coated micro-catheter involving in vitro and in vivo assay. Further studies will focus on identifying the impacts for affecting hemocompatibility performance and develop standardization methods for these medical devices contacting with blood.
Footnotes
Acknowledgements
This work was funded by the Shandong Science and Technology Development Plan Project (2017GSF218004) and partly by the National Key Research and Development Project (2016YFC1103205).
Conflict of interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.