
Abstract
Background:
Isometric cervical flexor system exercise (ICF) and isometric cervical extensor system exercise (ICE) are cervical stabilization techniques that have been used to restore cervical crossed syndrome (CCS)-associated forward head posture. However, the therapeutic effects and underlying motor control mechanisms remain elusive.
Purpose:
The purpose of present study was investigating the concurrent therapeutic effects of ICF and ICE on muscle size, muscle imbalance ratio, and muscle recruitment sequence using ultrasound imaging and electromyography.
Methods:
A total of 18 participants (7 females;
Results:
Paired t-test analysis showed that sternocleidomastoid thickness was greater during ICF than ICE. Similarly, cross-sectional area and horizontal thickness of the longus colli were greater during ICE than ICF. The upper trapezius/lower trapezius muscle imbalance ratio and the pectoralis major/lower trapezius muscle imbalance ratio were significantly decreased during the application of ICE compared to ICF.
Conclusions:
These results provide compelling, mechanistic evidence as to how ICE is more beneficial for the restoration of neuromuscular imbalance than ICF in individuals with CCS.
Terminology
Cervical crossed syndrome Cross-sectional area Electromyography Isometric cervical flexor system exercise Isometric cervical extensor system exercise Lower trapezius Sternocleidomastoid Pectoralis major Upper trapezius
Introduction
Cervical crossed syndrome (CCS) is a common musculoskeletal impairment resulting from a neuromuscular imbalance between the tonic-flexor system (prone to overactive and short, usually superficial muscles) and the phasic-extensor system (prone to underactive and weak, usually deep stabilizing muscles) [1–3]. Normally, neuromuscular balance represents an optimal interaction between the tonic-flexor and phasic-extensor systems for coordinated posture and movement of the cervical spine [2,4]. Neuromechanically, this interaction generates balanced muscular forces to create an optimal arthrokinematic centration and neutral joint alignment, thereby creating upright postural stability during cervical movement [2,5]. Pathologically, CCS is characterized by overactivation of the tonic-flexors (e.g., the sternocleidomastoid, levator scapula, and upper trapezius on the dorsal side coupled with anterior crossing of the pectoralis major and minor) along with inhibition or weakness of the phasic-extensors (deep longus colli and capitis ventrally coupled with the middle and lower trapezius and serratus anterior). Subsequently, these overactive antagonistic tonic-flexors reciprocally inhibit the agonistic phasic-extensors [6], leading to muscular tightness or a reduction in sarcomere number [7]. Over time, this pattern of neuromuscular imbalance creates joint decentration (altered arthrokinematic motion), particularly at the cervical joints (e.g., atlanto-occipital joint, C4-C5 segment, cervicothoracic joint) [2,5]. This syndrome encompasses postural impairments (e.g., forward head posture, decreased cervical lordosis) and movement impairments (e.g., joint decentration). Recent clinical evidence demonstrated the relationship between impaired muscle coordination of the neck muscles and cervical pain [8–10]. For example, individuals with neck pain showed high amounts of electromyography (EMG) activity in the superficial neck flexors (sternocleidomastoid and anterior scalene), deactivated deep cervical flexor activity, a reduction in cervical range of motion [9], and impaired motor control of deep neck flexors during cranio-cervical flexion [8]. Also, Jull et al. observed an increase in sternocleidomastoid EMG amplitude in both insidious neck pain patients and whiplash patients compared to normal controls [10]. These findings suggest that the neuromuscular imbalance between the deep phasic neck muscles and superficial tonic neck muscles should be mitigated for effective management of CCS (Page, Frank & Lardner, 2010; Sahrmann, 2002) [2 ,11].
To restore neuromuscular balance, isometric cervical flexor system exercise (ICF) [12] and isometric cervical extensor system exercise (ICE) [2] are commonly used, but the therapeutic efficacy of the two sets of exercises have not been thoroughly compared. Conceptually, both isometric exercises are designed to strengthen underactive deep neck flexors and reduce the reliance on overactive superficial neck flexors in order to restore muscle balance in CCS. During ICF, resistance (20% of maximal voluntary isometric contraction) is applied by the individuals to their own forehead via shoulder flexion, shoulder adduction, and elbow flexion; this exercise primarily activates the synergistic flexor system or chain [12,13]. During ICE, the same amount of the load is applied by the individuals on the back of their head via an elastic band with shoulder extension, shoulder abduction, and elbow extension, which activates the synergistic extensor system or chain [2]. It has been theorized that ICF may further accentuate muscle activation of the inherently hyperactive flexor system that occurs in cervical flexion and forward head posture, including the sternocleidomastoid, pectoralis major, and upper trapezius muscles. At the same time, ICF may reciprocally inhibit the underactive longus colli in CCS. On the other hand, ICE activates the deep neck stabilizers (longus colli and capitis) coupled with the extensor system (middle and lower trapezius, serratus anterior) in the kinetic chain to upright the forward head posture and also provide cervical stabilization, thereby producing more balanced muscle activation than ICF [2]. Nevertheless, to the best of our knowledge, the underlying muscle imbalance mechanisms of these cervical stabilization techniques remain an open research inquiry. Hence, the specific aim of the present study was to compare the differences in muscle size, muscle imbalance ratio, and muscle recruitment sequence of ICF and ICE using ultrasound imaging and EMG measurements. Our basic hypothesis was that ICE would be more effective at increasing activation in the underactive longus colli and lower trapezius while inhibiting overactivation of the sternocleidomastoid, pectoralis major, and upper trapezius muscles compared to ICF.
Methods
Participants
A total of 18 participants (7 females, 24 ± 4.0 years) with CCS volunteered for this study. Informed consent was obtained prior to the study. The experimental protocol was approved by Our Human Studies Committee. Inclusion criteria included individuals with a history of cervical pain and a forward head posture characterized by anterior deviation of the ear lobe more than 1 cm from the vertical plumb line [14]. Exclusion criteria included any present medical conditions associated with neuromotor or musculoskeletal impairments or previous surgical history in the cervical and upper quarter including discectomy, arthroscopic shoulder surgery, or shoulder dislocation surgery.
Experimental procedure
All participants underwent baseline testing during rest and then were tested during both ICF and ICE. The tests included measurements of muscle size with ultrasound imaging and muscle activity with EMG.
The ICF procedure was described to the participants, while emphasizing the isometric upper extremity flexion movement pattern–shoulder flexion, adduction; elbow flexion; wrist and hand flexion. The ICE procedure was also relayed, focusing on the isometric upper extremity extension movement pattern–shoulder extension, abduction; elbow extension; wrist and hand extension. They then practiced for 5 minutes in an upright sitting position. Specifically, ICF involved the participant isometrically pushing his or her forehead against a self-induced resistance force (approximately 20% of the maximal voluntary isometric contraction, MVIC) with both hands in an upper extremity flexion pattern (Fig. 1(A)) [12,13]. ICE involved isometrically resisting a sustained low load (matched to the ICF exercise to equal approximately 20% of MVIC) applied on the back of the head via an elastic band in an upper extremity extension pattern (Fig. 1(B)) [2,13]. A handheld dynamometer was used to monitor the load and maintain a constant resistance.

The ultrasound imaging test during the intervention procedures: (A) isometric cervical flexor system exercise emphasizing isometric upper extremity flexion movement pattern (shoulder flexion and adduction, elbow flexion, wrist and hand flexion). (B) isometric cervical extensor system exercise focusing isometric upper extremity extension movement pattern (shoulder extension and abduction, elbow extension, wrist and hand extension).
SonoAce (X8, Medison Co., Ltd, Seoul, South Korea) with a 10 MHz transducer was used to unilaterally measure the size of the sternocleidomastoid and longus colli muscles (right side) during rest and during the ICF and ICE exercises. Initially, the participants were comfortably seated with both arms resting in their lap and with a neutral head and neck position. The longus colli was identified by palpating the thyroid cartilage, and a mark was made 2 cm below this anatomical landmark. Ultrasound gel (Powersonic, JJ Industry, Seoul, South Korea) was then applied to the transducer head, which was transversely positioned 2 cm inferior to the thyroid cartilage [15]. The transducer head was maneuvered to acquire the clearest images of the sternocleidomastoid and longus colli. Sternocleidomastoid thickness was defined as the distance between the ventral and dorsal muscle fasciae [16]. The longus colli cross-sectional area (CSA) was measured along with the horizontal and longitudinal thickness, because it has a relatively small diameter (Fig. 2) [15]. Thus, three images were obtained and used for statistical analysis.
Electromyography (EMG)
A surface EMG with a WEMG-8-type cable (Laxtha Inc., Daejeon, South Korea) was used to record the onset times and amplitudes of the upper trapezius, lower trapezius, pectoralis major, and sternocleidomastoid. Specific anatomical landmarks for EMG placements were identified according to the standard guidelines [17]. As in ultrasound imaging, the participant was seated in a comfortable chair. Skin preparation was first implemented to reduce skin impedance by dry-shaving the target muscle zones with a disposable razor, rubbing with sand paper, and cleaning with alcohol prior to the electrode placement. A pair of electrodes (interelectrode distance = 2.0 cm) was attached on the muscle bellies in parallel and a ground electrode was positioned over the acromion [17,18].
Telescan 3.06 software (Laxtha Inc., Daejeon, South Korea) was used to acquire EMG signals at a sampling frequency of 1024 Hz for 5 s while the participant performed either ICF or ICE. The participant began the exercise upon the initiation of the beeping signal. The raw EMG data was band-pass filtered at 20–450 Hz along with a 60 Hz notch filter. The root mean-square EMG data was normalized to the MVIC. The onset time for each muscle was set to three standard deviations of the mean resting amplitude recorded for at least 50 ms duration [19].
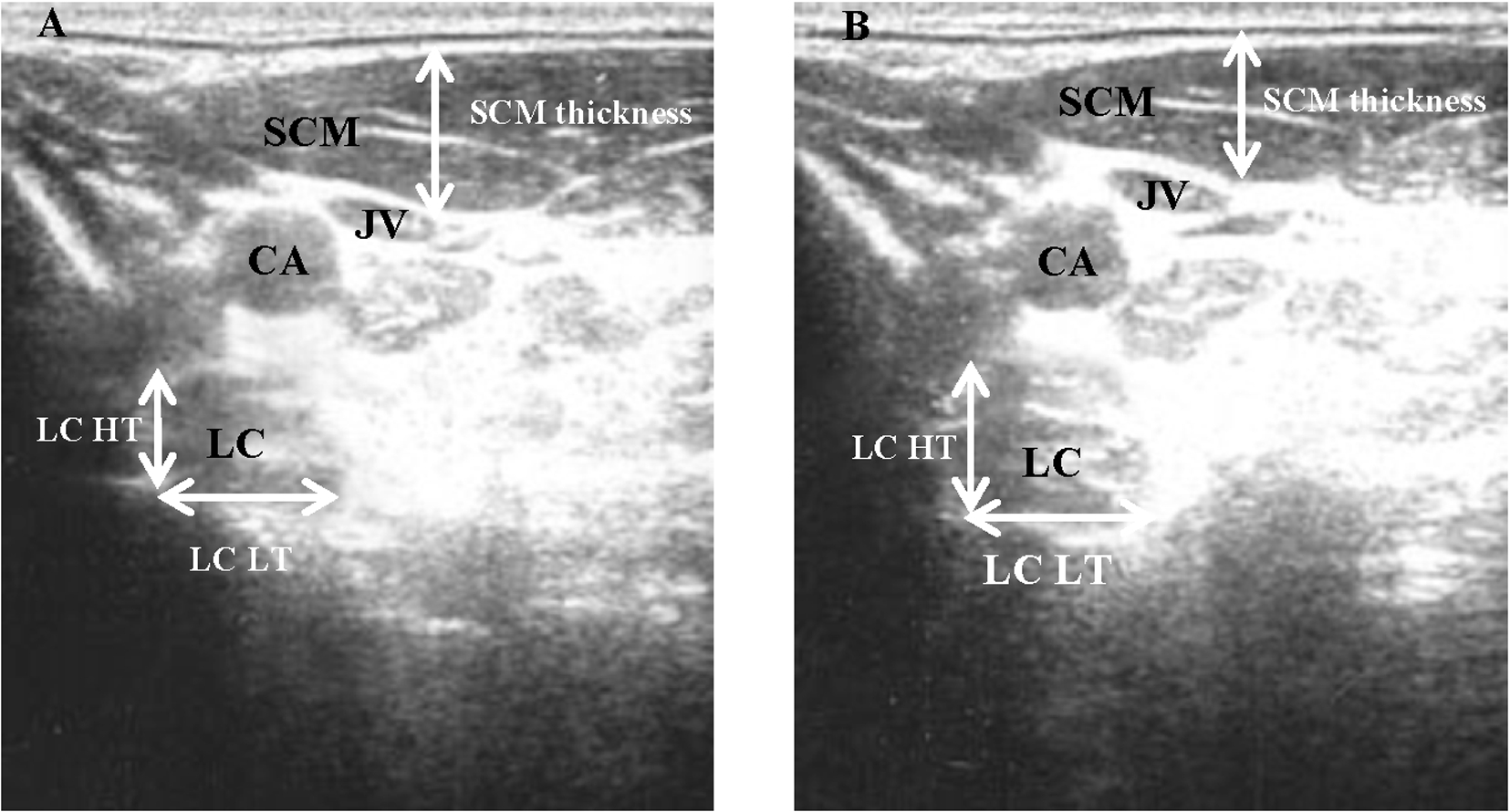
The comparative ultrasound images of longus colli and sternocleidomastoid muscles between the isometric cervical flexor system exercise (A) and isometric cervical extensor system exercise (B). SCM: Sternocleidomastoid. JV: Jugular vein. CA: Carotid artery. LC: Longus colli.
A handheld dynamometer (Commander Muscle Tester, JTECH Medical, Salt Lake City, UT, USA) was used to determine the maximal target force during MVIC and monitor the submaximal isometric resistance (20% of MVIC) during the test to ensure a consistent measurement.
Statistical analysis
Calculations of means and standard deviations and assessment of statistical significance were performed using the PASW Statistics Package 18 (SPSS Inc., Chicago, IL, USA). A paired t-test was used to compare mean muscle size and EMG amplitude between ICF and ICE. The level of statistical significance was set at
Results
Muscle size
Sternocleidomastoid thickness was greater during ICF than ICE (
Comparison of muscle size difference (intervention − rest, mm) between isometic cervical extensor system exercise (ICE) and isometric cervical flexor system exercise (ICF)
Comparison of muscle size difference (intervention − rest, mm) between isometic cervical extensor system exercise (ICE) and isometric cervical flexor system exercise (ICF)
SCM: sternocleidomastoid; LC CSA: longus colli cross sectional area; LC HT: longus colli horizontal thickness; LC LT: longus colli longitudinal thickness.
Paired t-test showed a significant difference in the relative muscle size between the interventions at
The muscle imbalance ratio of the upper trapezius/lower trapezius (UT/LT) muscle group was significantly less during ICE compared to ICF (
Comparison of muscle imbalance ratio (MIR) between isometic cervical extensor system exercise (ICE) and isometric cervical flexor system exercise (ICF)
Comparison of muscle imbalance ratio (MIR) between isometic cervical extensor system exercise (ICE) and isometric cervical flexor system exercise (ICF)
UT/LT: the ratio between %maximum voluntary isometric contraction (MVIC) of upper trapezius and %MVIC of lower trapezius; SCM/LT: the ratio between %MVIC of sternocleidomastoid and %MVIC of lower trapezius; PM/UT: the ratio between %MVIC of pectoralis major and %MVIC of upper trapezius.
Paired t-test showed a significant difference in the muscle imbalance ratio between the interventions at
In regard to the motor recruitment sequence, during ICE, the lower trapezius was activated first in the majority of the participants, followed by either the pectoralis major or sternocleidomastoid, and then the upper trapezius. In contrast, during ICF, either the sternocleidomastoid or lower trapezius was activated first, followed by the pectoralis major, and then the upper trapezius (Fig. 3).
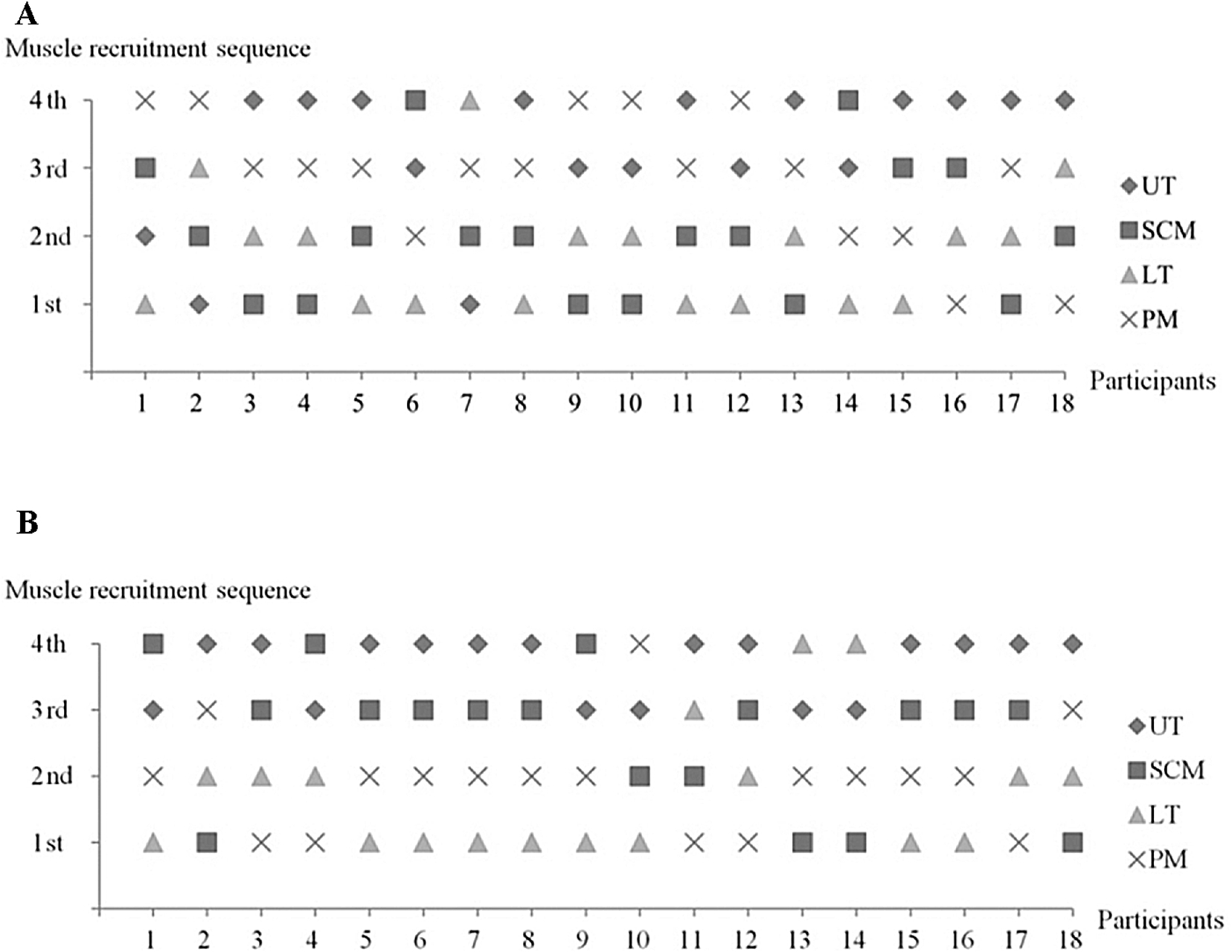
Muscle recruitment sequence during isometric cervical flexor system exercise (A) and isometric cervical extensor system exercise (B).
The present study highlighted the comparative effects of ICE and ICF in individuals with CCS and associated forward head posture and muscle imbalance. As we anticipated, the muscle activation that occurs during ICE better lends itself to restoring muscle imbalance than ICF, which is the conventional treatment. Most importantly, this is the first evidence quantitatively demonstrating the therapeutic mechanisms of ICE using ultrasound imaging and EMG measurements. However, this makes it difficult to compare our results with previous data from other studies.
Using ultrasound-imaging data, we demonstrated that ICE significantly activated the underactive longus colli and deactivated the overactive sternocleidomastoid, supporting a superior effect of ICE over ICF. This finding is consistent with other EMG studies [20,21]. For example, Jull et al. (2008) observed that individuals with neck pain initially showed lower EMG amplitude in deep cervical flexors and relatively greater EMG amplitude in the sternocleidomastoid and anterior scalene, resulting in neuromuscular imbalance [20]. However, after training, neuromuscular imbalance, associated cervical pain, and motion were significantly improved. Jull et al. (2009) compared the effect of low-load cranio-cervical flexion and neck flexor strengthening exercises on EMG amplitudes in the longus colli, anterior scalene, and sternocleidomastoid in patients with neck pain and found increased deep neck flexor activation and decreased superficial neck flexor activation (sternocleidomastoid and anterior scalene) in the low-load cranio-cervical flexion exercise group [21]. This finding indicates that low-load cranio-cervical flexion exercises promote the restoration of the neuromuscular balance, and these exercises may be more effective for restoring cervical muscle balance than the conventional approach [21]. Similarly, a recent case report examined the effect of progressive deep cervical flexion exercise including low-load training (weeks 1–4) with PBU, joint motion sense training, higher load, and sudden load, followed by integration with function. They demonstrated improved muscle balance, improved cervical spine range of motion, and decreased pain and dizziness, as well as a full recovery of functional activities [22]. In the present study, ICE was associated with better neuromuscular balance in individuals with CCS who pathomechanically exhibited forward head posture, excessive craniocervical extension, excessive cervical flexion, and compromised neuromuscular imbalance (inhibited or underactive, weak longus colli vs. overactive, strong, and short sternocleidomastoid and scalene muscles). Such mechanisms of ICE may provide a neuromechanical rationale as to how ICE can centralize or neutralize a deranged cervical spine along with the shoulder and pelvis. These improvements, in turn, can improve joint position and kinesthetic proprioception inputs as well as the muscle length-tension relationship. Consequently, accurate sensory feedback and muscle length-tension can help restore the ability of the longus colli to stabilize the neck up righting in coordination with other global pattern muscles [2].
Further EMG analysis of the muscle imbalance ratios revealed that the upper trapezius, the pectoralis major, and the sternocleidomastoid muscles are prone to overactivation while the lower trapezius is prone to inhibition; these activation patterns are improved during ICE. This result corroborates Janda’s notion that ICE is more beneficial than ICF for restoring muscle imbalance between the tonic-flexor and phasic-extensor systems, due to the fact that it reciprocally deactivates the overactive muscles (e.g., the upper trapezius) and activates the underactive muscles (e.g., the lower trapezius) [2,6]. As a result, this restored muscle balance can correct an altered cervical spinal alignment and length-tension relationship, thereby creating optimal joint centration during cervico-cranial movement in individuals with CCS-associated neuromuscular imbalance and CCS-associated forward head posture. Kluemper et al. (2006) investigated the effect of the combination of stretching the anterior shoulder muscle and strengthening the posterior shoulder muscle to address muscle imbalance in competitive swimmers and showed a significant reduction in excessive forward shoulder posture [23]. Although this study demonstrated that ICE can be effective at restoring muscle balance and, eventually, improve postural alignment and associated movement impairments, it remains unknown whether or not such improvement is dependent on relative neuromuscular reciprocal inhibition of the anterior scapular muscles. Our present EMG findings showed that the pectoralis muscle was relatively deactivated during ICE, while the posterior scapular muscles (e.g., the lower trapezius) were more activated. Moreover, in the present study, the lower trapezius was first activated during ICE, followed by either the pectoralis major or sternocleidomastoid, and then the upper trapezius; during ICF, either the sternocleidomastoid or lower trapezius was activated, followed by the pectoralis major and the upper trapezius. Because ICE facilitated earlier activation of the scapular stabilizers (e.g., the lower trapezius) while delaying activation of the dominant pectoralis major and sternocleidomastoid muscles, proper stabilization occurred prior to the dynamic shoulder movement; this pattern is in agreement with Janda’s concept of re-establishment of neuromuscular balance [2,24]. Research into the biomechanics revealed that the lower trapezius acts as important shoulder stabilizer because it balances the scapular rotation coupling forces [25,26]. Several studies found that overhead athletes with shoulder impingement exhibited relatively overactive upper trapezius activation [27,28], but reciprocally deactivated serratus anterior and lower trapezius muscles. This observation also supports Janda’s diagnostic notion of CCS that the upper trapezius and pectoralis major and minor muscles tend to be overactive and tight while the lower trapezius and serratus muscles are susceptible to inhibition and weakness [2,29]. EMG activation onset time and EMG amplitude of the trapezius were compared between normal individuals, overhead athletes, and those with impingement and were found to be delayed and less active when compared to the upper trapezius [27,30,31]. Over time, this neuromuscular imbalance results in scapular elevation rather than upward rotation, creating an arthrokinematic imbalance or decentration of the glenohumeral and scapulothoracic joints and consequent neck-shoulder dysfunction. Moreover, underactivation of the lower trapezius or overactivation of the upper trapezius may lead to an alteration of scapular rotation, which in turn leads to an upward decentration or migration of the axis of rotation of the glenohumeral joint, thus causing the impingement [2].
There are several limitations to the present study. First, the current study validated a short-term effect and invites further study to evaluate a long-term clinical effect. Second, EMG activation of the longus colli was not determined, and it was difficult to examine the actual activation pattern. Nevertheless, ultrasound imaging implemented in the current experiment is a more compliant and safe measurement and muscle size was reported to be closely correlated with EMG activation in previous studies [32–34]. Lastly, the change in the kinematics of forward head posture was not quantified; however, we visually monitored and ensured that all participants exercised the correct cervical and shoulder alignment.
Collectively, these results suggest that ICE should be more effective at normalizing neuromuscular balance in the neck and shoulder muscles in individuals with excessive CCS-associated forward head and neck posture when compared to ICF.
Conclusions
The present investigation demonstrated that ICE should be more beneficial for the restoration of neuromuscular imbalance between the superficial and deep neck flexors than the conventional ICF. The results provide new important clinical rationale and evidence for the use of ICE in the management of neuromuscular imbalance and associated CCS or neck-shoulder pain syndrome.
Footnotes
Acknowledgements
Both Lee and Kim equally contributed to this project.
Conflict of interest
The authors declare that there is no conflict of interest regarding the publication of this paper.