
Abstract
BACKGROUND:
Many novel biomaterials have been incorporated in toothpastes to promote remineralization of tooth structure.
OBJECTIVES:
This study was carried out to compare the discrepancies between declared and actual total fluoride (TF) or total soluble fluoride (TSF) concentration of two modern toothpastes containing bioactive glasses; these were also assessed for their remineralization potential.
MATERIALS AND METHODS:
The TF and TSF concentration were assessed using a fluoride ion selective electrode. Enamel remineralization was evaluated through micro-hardness analysis. Eighteen enamel blocks were divided into three groups: 1 (n = 6; control), 2 (n = 6; Novamin® toothpaste), and 3 (n = 6; BiominF® toothpaste). The specimens were demineralized by 6 wt% citric acid (pH = 2.2). Subsequently, the specimens in group 1 were kept in artificial saliva (AS), while the specimens in groups 2 and 3 were stored in AS + Novamin® and AS + Biomin®, respectively.
RESULTS:
Both Novamin® or BiominF® showed less TF concentration than their label claims. BiominF® had more TF and TSF compared to Novamin® (p < 0.05). The BiominF® toothpaste presented higher micro-hardness values on remineralization.
Introduction
Dental caries is one of the most common diseases which is recognized as the primary cause of oral pain and tooth loss. It is a major public health oral disease which hinders the achievement and maintenance of oral health in all age groups [1]. The World Health Organization (WHO) pointed that the global problem of oral disease persists despite great improvements in the oral health of population in several countries. WHO also claimed that poor oral health may have a profound effect on general health as well as quality of life, and several oral diseases are related to chronic diseases [2]. In Saudi Arabia, such a clinical condition still affects nearly 70% of the children [3]. The formation of dental plaque (bacterial biofilm) on the tooth surface, along with its metabolic process characterized by the fermentation of dietary carbohydrates, creates a favorable acid environment that causes demineralization of the dental hard tissues (e.g. enamel and dentin) [4,5]. Over the past few decades, various mechanisms have been established to restrain the prevalence of dental caries, such as increasing fluoride exposure of teeth (by toothpastes or mouthwashes) [6,7], developing artificial sweeteners (e.g. sorbitol, xylitol) [8,9], introducing chlorhexidine gluconate products [10,11], and stimulating salivary flow [12].
The role of fluoride in preventing dental caries is important as it decreases the mineral solubility of tooth’s structure; its presence also increases the probability to replace the hydroxyapatite (HAP) with a more acid resisted mineral known as fluorapatite (FAP) [13]. Indeed, such a mineral exchange makes the enamel more resistant against dissolution induced by acids produced by bacteria as well as those from acidic food and drinks [14,15]. A further protective mechanism conceivably offered by fluoride is based on the fact that it may interfere with the bacterial metabolism and alters the composition of plaque biofilm [16]; this may reduce the incidence of caries.
Toothpastes are the most used products containing fluoride used at home for oral hygiene maintenance, which have been widley proven to be able to reduce dental caries prevalence [17]. Previous studies have shown that toothpaste’s effectiveness in caries prevention depends on the fluoride content and its available concentration [4,17].
Bioactive glass is a biocompatible and osteoconductive material typically used for bone repair and regeneration purposes [18]. However, its use in dental clinical applications has increased during the last decade due to its unique mineral composition, which is very similar to that of the bone and teeth [19]. Its first and most popular variant is Bioglass® 45S5 (BAG), which is composed of calcium sodium phosphosilicate. BAG is quite popular due to its ability to generate an intimate bond with the host tissue in less than 2 h [20]. Since the introduction of BAG in the late 1960’s by Prof. Larry Hench, such materials have been modified and various compositions have been synthesized [21]. In general, because of a controlled degradation over time, the ions released by such bioactive glasses can interact with the body tissues and offer various therapeutic effects such as repair and regeneration of bone and dental tissues [22]. In dentistry, they are currently being successfully used for enamel remineralization and dentin tubule occlusion [20].
Several toothpastes containing different fluoride concentrations, as well as further bioactive ingredients, are nowadays available in the market. Unfortunately, there is a deep lack of information on their real potential to remineralize enamel and to release fluoride. Thus, this study was aimed at evaluating the total fluoride (TF) and total soluble fluoride (TSF) concentration present in two commercial toothpastes containing having different bioactive glasses (Novamin® and BiominF®) as active principles. Moreover, their potential to remineralize the enamel was also assessed in this study through microhardness evaluation.
The null hypothesis of the study was that both Novamin® and BiominF® have the same TF concentration as their labels have claimed and possess a similar capability to repair demineralized enamel.
Materials and methods
Fluoride analysis
Setting up apparatus for fluoride analysis
The evaluation of TF and TSF concentration was performed using a multimeter (VWR® sympHony TM , USA) system equipped with a fluoride ion selective electrode (Orion 9609BN, 710A meter, South Burlington, VT, USA) as an indicator electrode and a reference electrode (silver - silver chloride or double junction). The working solution consisted of variable fluoride concentration (from 10−1 to 10−7 M) dissolved in 0.1 M sodium fluoride. Each standard solution with standardize volume of 0.1 M NaF was then mixed with 25.0 mL of total ionic strength adjustment buffer (TISAB) solution and diluted into a 100 mL volumetric flask. The entire process was repeated with the residual concentration. A clean and dry indicator along with a reference electrode were introduced into the solution, slightly whirled and the potential difference on the multimeter system was recorded. The electrodes were removed, rinsed with distilled water and air dried between analyses.
Total fluoride (TF) and total soluble fluoride (TSF)
For TF, a specified amount (1.0 gm) of each toothpaste (Novamin® and BiominF®) was placed into a glass beaker and the level was recorded. Subsequently, 25 mL of TISAB and 25 ml of distilled water were dispensed in the same beaker and the mixture was boiled for 5 mins in order to achieve a perfect dissolution of the ingredients of the pastes into the water solution. The mixture was then removed from the heater and left undisturbed at room temperature under continuous agitation (60 rpm). This mixture was then transferred into a 100 mL plastic volumetric flask for analysis.
Analysis of TSF involved the same steps as measurement of TF except before recording the potential difference; the sample solution was filtered to eliminate insoluble particles (e.g. abrasive particles) of the toothpaste. By using the standard calibration curve previously prepared, the fluoride concentration (Molarity: M) of an unidentified solution was calculated by an equation for the line. The results were plotted between y-axis (potential difference, mV) and x-axis (logarithm of the fluoride concentration). The following two formulas were used to calculate percentage and ppm of fluoride respectively:
Demineralization and remineralization cycle and surface micro-hardness analysis
Eighteen extracted non-carious human third molar teeth were collected under ethical approval (Ref: EA 2016017) obtained from the Scientific Research Unit/IRB. Their roots were cut using a water-cooled diamond saw (Isomet® 5000 Linear Precision Saw, Buehler Ltd, IL, USA) at a blade speed of 3,000 rpm and a feed rate of 15 mm/min. Their anatomical crowns were embedded in the acrylic blocks in such a way that only the buccal surface of enamel was exposed. Toothpaste slurries were prepared by mixing 1 g toothpaste with 5 mL artificial saliva (AS). Artificial saliva (AS) was formulated by mixing 0.400 g NaCl, 0.400 g KCl, 0.69 g NaH2PO4 H2O, 0.795 g CaCl2 H2O, and 0.005 g Na2S 9H2O in 1000 mL deionized water, as suggested by Fusayama et al. [23]. The pH of freshly prepared AS was adjusted to a neutral pH of 7.0 by the addition of 1 M sodium hydroxide (NaOH).
Before exposing the enamel specimens to toothpaste slurries, the specimens were exposed to 6 wt% citric acid (pH = 2.2) for 1 min to create a demineralization lesion as previously suggested by Farooq et al. [24]. The enamel blocks were randomly divided into following three groups (six blocks/each group) and received the following treatment post demineralization for 24 hours; Group 1: enamel blocks kept in AS (control group); Group 2: enamel blocks kept in a mixture of AS and Novamin®; Group 3: enamel blocks kept in a mixture of AS and BiominF®. The specimens were analyzed for changes in the values of surface micro-hardness and the data were collected at three stages; baseline (sound enamel), after demineralization, and after remineralization. The Vickers hardness number (VHN) values were measured using a digital micro-hardness tester (FM-ARS 9000; Future-Tech Corp, Kawasaki, Japan). In each sample, three indents were made on the marked area (Fig. 1) using a Vickers diamond indenter under a 100-g load applied for 10 seconds as suggested by Farooq et al. [25].

The shape and sequence of Vickers indentations to assess micro-hardness of enamel’s surface.
The summary of the experimental work performed for micro-hardness analysis is shown in Fig. 2.
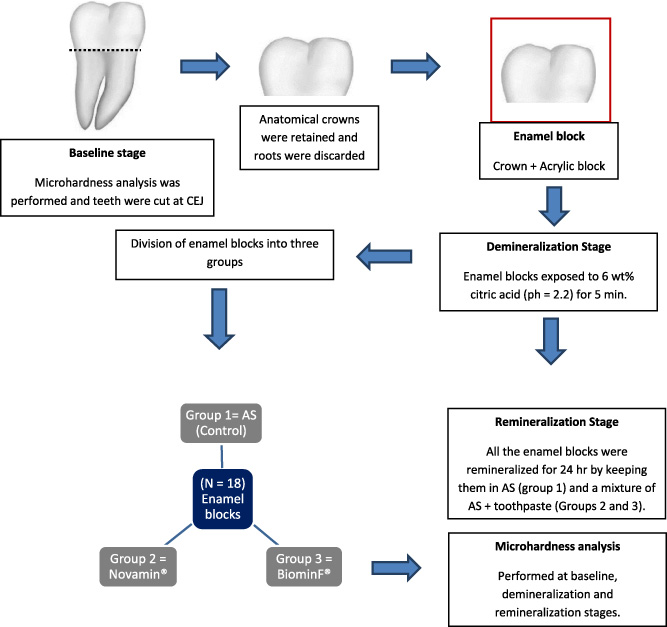
The summary of the experimental work conducted for micro-hardness analysis.
The data analysis was performed by using SPSS-20.0 (IBM, Chicago, IL, USA). For the fluoride analysis, differences were analyzed using a non-parametric Mann–Whitney U-test and non-parametric Kolmogorov–Smirnov one-sample test. The VHN results were presented as Mean ± Standard deviation and then analyzed using repeated measures analysis of variance (ANOVA) to compare the remineralization potential of the toothpaste containing Novamin® to that of BiominF® , as well as to the control group (no toothpaste treatment). Further, Post-Hoc Fisher’s least-significant difference test was applied to compare pair-wise mean effect between the groups (𝛼 = 0.05).
Results
Novamin® and BiominF® toothpastes showed less TF content compared to the values claimed by their own companies (1450 ppm and 530 ppm correspondingly). However, BiominF® presented more TF and TSF compared to the Novamin® toothpaste (Table 1). The mean TSF value for both groups was less then their mean TF values. For the Novamin® group, the mean values for TF and TSF were 90.35 ppm and 89.22 ppm, respectively.Whereas for BiominF® group, mean TF was 421.30 ppm and the TSF mean value was 414.52 ppm. The misplaced part of TSF compared with TF of these toothpastes corresponds to insoluble fluoride (InF) which is supposed to be bound to the abrasive. The significant differences (p < 0.05) in TF and TSF were found between groups 2 (Novamin®) and 3 (BiominF®) (Table 1).
Showing evaluated toothpastes, declared TF, mean TF ± SD, and mean TSF ± SD
Showing evaluated toothpastes, declared TF, mean TF ± SD, and mean TSF ± SD
∗ Non-parametric Mann–Whitney U-test, ∗∗ Non-parametric Kolmogorov–Smirnov one-sample test based on median value (label claim). a Significant difference of mean at 5% level of significance.
Micro-hardness analysis showed clear difference between remineralization and baseline value (post demineralization). The hardness values for all the groups were decreased after demineralization, and increased after remineralization. Although group 1 (control group) was able to remineralize the enamel structure after demineralization, 24 hours were still not enough for AS to restore the structure, not even back to the baseline values. For instance, group 3 (BiominF®) showed 82.09 VHN, followed by group 2 (Novamin®) = 80.14 VHN (Table 2). Both the groups 2 (Novamin®) and 3 (BiominF®), showed significant differences (p < 0.05) compared to the control group as well as to their own baseline values (Table 2).
Showing Vickers hardness number (VHN) for three groups evaluated for sound, demineralized, and remineralise human enamel
a Significant difference of mean between the groups versus control at 5% level of significance. b Significant difference of mean between within each group versus baseline at 5% level of significance.
Two bioactive glasses-based dentifrices were assessed in this study to evaluate their TF and TSF concentration. Furthermore, their remineralization potential was also evaluated by treating human enamel blocks with the tested toothpaste for 24 hours. Based on the results of this study, the null hypothesis that both toothpastes have the same TF as their label claims and possess same ability to remineralize enamel structure must be rejected. This study has demonstrated that the two tested toothpastes had significant less concentration of TF and TSF compared to the values descloused by their own manufacturers. Current results are in agreement with recent studies, which also reported a clear disharmony between the labeled and actual TF concentration [26-28]. This study showed that the toothpaste containing the novel active ingredient fluoride-containing bioactive glass (BiominF®) presented greater values in terms of TF and TSF concentration (421 ppm and 414 ppm respectively) compared to the conventional bioactive glass toothpaste (Novamin®) showed a TF concentration of 90 ppm and a TSF concentration of 89 ppm.
The addition of fluoride in toothpastes is beneficial for tooth structure. Indeed, the existing literature shows numerous studies about the relationship of fluoride and prevention of caries [29,30]. It is commonly accepted that the concentration of fluoride has a direct correlation with the prevention of caries; the higher the concentration, the better their effect in preventing caries manifestation [31]. Moreover, it has been widly reported that the presence of fluoride ions may prevent enamel demineralization and favour its remineralization [32,33]. It is important to mention that for a dentifrice in order to have an effective anti-carious function, it should not have only a higher concentration of total fluoride, but should it should also provide necessary soluble fluoride available for the enhancement of remineralization [34]. A possible explanation for BiominF® toothpaste to show better TF and TSF concentration could be credited to the fact that it contains fluoride in its glass composition, unlike Novamin®, which is based on traditional 45S5 composition (containing no fluoride) [25]. The presence of fluoride in the bioactive glass ensures long-term delivery which is particularly desirable for dental applications [25].
A further aspect of our study investigated the micro-hardness level of the surface enamel of samples. The surface layer has significant importance when it comes to the carious lesions, therefore changes in this area should be investigated and a suitable method is micro-hardness assessment [35]. As enamel is made up of crystals and is prone to cracking, micro-hardness analysis technique is therefore suitable for it as it is a quick, and non destructive [36]. BiominF® showed better remineralization potential of both the toothpastes when compared to the baseline values (of sound enamel) according to surface micro-hardness test by Vickers indentation, when placed for 24 hours in their respective slurries and after an acid challenge. Acidic challenge creates demineralization (low mineral content at the surface as compared with the normal enamel) and thus, shows a decreased hardness value [36]. Post-remineralization, although the difference was only a slight, still BiominF® demonstrated better remineralization potential than Novamin®. This suggests that there is a potentially enhanced remineralization potential for the BiominF® toothpaste. Traditional fluorides incorporated in toothpastes are usually washed away quickly by the salivary flow [37]. One example is Novamin® which requires the addition of soluble fluoride in the formulation process of the toothpaste as it lacks fluoride in its glass [38]. On the other hand, a likely sustained release of fluoride from BiominF® resulted in the formation of FAP instead of HAP (due to its composition containing fluoro-calcium phosphosilicate) [34].
Surprisingly, there are not many studies reported in the literature which have analyzed the remineralization potential of bioactive glass toothpastes. A study performed previously also showed successful remineralization potential of bioactive glass-based toothpaste in terms of treating dentine hypersensitivity [39]. Another recent in-vitro study demonstrated more tubule occlusion on dentin specimens achieved by Biomin® as compared to Novamin® and standard fluoride toothpaste [40]. A previous study performed on BiominF® and Novamin® showed better remineralization potential (demonstrated by micro-computed tomography and profilometry) by BiominF® toothpaste [25] and our results agree with that study. Palaniswamy et al. [35] utilized Vickers micro-hardness testing to analyse the effect of application of bioactive glass and amorphous calcium phosphate-casein phosphopeptide (ACP-CPP) on early enamel lesions. The authors concluded that both bioactive glasses remineralized early enamel lesions equally, although bioactive glass performed better than ACP-CPP at earlier stage. However, Mehta et al. [41] compared bioactive glass and ACP-CPP in terms of their remineralization potential of demineralized human enamel by Vickers hardness testing and concluded that the application of bioactive glass remineralized the carious lesions more effectively as compared with ACP-CPP [41].
In another earlier in-vitro study, Maçon et al. studied the bioactivity of bioactive glass toothpaste in a remineralizing media and found that HAP was formed on the surface of bioactive glass toothpaste after 1 hour [42]. Farooq et al. developed new fluoride containing bioactive glasses previously and demonstrated via fourier transform infrared spectroscopy (FTIR), formation of apatite within 6 hours of being exposed to Tris buffer solution (much faster than 45S5, traditional bioactive glass without fluoride) [43]. These evidences clearly suggest that bioactive glass can remineralize tooth structure, and if fluoride is present in its composition, it enhances formation of FAP.
One limitation of our study is its in-vitro nature. In actual in-vivo conditions, oral cavity continuously goes through cycles of demineralization and remineralization. In our study, it was assessed only once, but still, the results demonstrate better performance of BiominF® toothpaste.
Conclusion
BiominF® toothpaste demonstrated more TF and TSF content as compared to Novamin® and a considerable potential to promote remineralization of demineralized human enamel. Future in-vivo studies are suggested to analyze the clinical effectiveness of BiominF® toothpaste.
Footnotes
Acknowledgements
The authors are grateful to the staff of King Fahd University of Petroleum and Minerals for helping with the fluoride analysis. They are also grateful to Mr. Intisar Siddiqui for helping with the statistical analysis, Mr. Lindsey Mateo and Mr. Jim Santendar for assisting with the micro-hardness scanning.
Conflict of interest
None to report.