
Abstract
BACKGROUND:
Periprosthetic joint infection is a major complication of total joint arthroplasty, with treatment requiring a two-stage exchange procedure and 6 weeks of systemic antibiotics. However, depending on the infection site, intravenous delivery of antibiotics like vancomycin (VCM) can have poor tissue transferability, thus reducing their therapeutic effect.
OBJECTIVE:
This study demonstrates the 24-week in vivo release profile and antibacterial activity of VCM from calcium phosphate cement impregnated with VCM (CPC/VCM) and compares them with those from polymethylmethacrylate impregnated with VCM (PMMA/VCM).
METHODS:
Rats were implanted with the test specimens between the fascia and quadriceps. After implantation for 24 weeks, the test specimens were removed and residual VCM was extracted to calculate the concentration of VCM released into rat tissues. We also examined the antibacterial activity of releasable VCM from the removed test specimens by placing them directly onto the surface of agar.
RESULTS:
CPC/VCM released greater concentrations of VCM for a longer period of time within the 24 weeks than PMMA/VCM. Moreover, CPC/VCM released 1.4 to 26.1-fold more VCM than PMMA/VCM. Using Staphylococcus aureus, antibacterial activity was logarithmically correlated with VCM concentration across the entire concentration range tested (12.5–800 μg/mL). While the area within which inhibition was observed—the inhibition zone—for both CPC/VCM and PMMA/VCM formed and gradually shrank with time after implantation, that for CPC/VCM was significantly larger than that for PMMA/VCM in each week after implantation.
CONCLUSION:
CPC/VCM releases greater amounts of VCM with antibacterial activity for longer periods of time than PMMA/VCM, suggesting that CPC is effective for facilitating the release of antibiotics for local action in patients with established postoperative infection.
Introduction
Periprosthetic joint infection is a major complication that can occur following total joint arthroplasty. It can result in extended hospitalization times, complicated revision procedures, and even complete failure of the implant, which may need to be removed with secondary surgery. These outcomes place great economic burden on patients and increase their mortality rate [1,2]. The gold standard of treatment for periprosthetic joint infection in recent years has proved successful, and involves a two-stage exchange procedure and 6 weeks of systemic antibiotics [3,4]. However, depending on the infection site, intravenous delivery of antibiotics like vancomycin (VCM) can have poor tissue transferability, thus reducing their therapeutic effect [5]. Combining VCM with a carrier in the first stage of the two-stage procedure is one way to improve therapeutic potential because the carrier retains antibiotic release and antibacterial activity to the infection site [6].
Calcium phosphate cement (CPC) and polymethylmethacrylate (PMMA) are some of the types of carrier materials used to retain VCM to infection sites in clinical settings [7–12]. We previously reported that CPC has a longer VCM retention time in vitro and in vivo, and has the potential to release a larger volume of VCM for a longer period of time than PMMA in in vitro and in vivo elution tests conducted across 8 weeks [13,14]. CPC/VCM and PMMA/VCM composites typically release VCM for between 8 and 12 weeks after the first stage [15]. However, some clinical cases may require long-term release for more than 8 weeks [16–18]. It is unclear whether CPC retains its VCM release profile in vivo during longer follow-up periods.
Several studies examining in vitro eluates have reported that antibiotics released from cement materials inhibit bacterial growth [13,19]. Moreover, in vitro antimicrobial testing by Kelm et al. showed that PMMA containing VCM and gentamicin exerts antimicrobial effects 3 to 14 weeks after implantation [20]. However, the duration of the antimicrobial effects of implanted CPC/VCM remains unclear.
We implanted CPC impregnated with VCM into rat tissue and examined the VCM release profile over 24 weeks. We also verified the presence of antibacterial activity against Staphylococcus aureus (S. aureus) after removal of the test specimen using the Halo (inhibition zone) Method.
Materials and methods
Materials
We followed the methods of Ken Sugo et al. [14]. CPC (Biopex-R Advance) and PMMA cement (Surgical Simplex P Bone Cement) were purchased from HOYA Technosurgical (Tokyo, Japan) and Stryker (Tokyo, Japan), respectively, and injectable VCM hydrochloride from Shionogi (Osaka, Japan). S. aureus strain (NBRC 12732) was obtained from the Biological Resource Center, National Institute of Technology and Evaluation (Chiba, Japan). All other chemicals were purchased from FUJIFILM Wako Pure Chemical (Osaka, Japan).
Test specimens
All procedures were conducted under aseptic conditions. CPC powder (24 g), VCM (2 g), and a dedicated solvent (5.6 mL) were thoroughly combined to form a paste, and an additional 1.6 mL of solvent was added to improve handling (final volume 7.2 mL). The weight of VCM (2 g) matched that used by our clinical team. The paste was transferred to a silicone sheet containing 60 molds (𝜑10 mm × t2 mm), and incubated for 3 h at room temperature until hardened. To produce PMMA cement, polymer powder (24 g), VCM (2 g), and liquid monomer (12 mL) were thoroughly combined to form a paste, and hardened as described for CPC. The hardened test specimens were removed from their molds and designated CPC/VCM and PMMA/VCM. The CPC/VCM and PMMA/VCM specimens were divided such that 40 were used for in vivo tests and the remaining 20 as reference specimens that were not implanted and as spares.
In vivo study
All in vivo studies received approval from the Kitasato University School of Medicine and Hospital Ethics Committee (Approval No. 2017-098). Ten-week-old Wistar rats were given 0.3 mg/kg medetomidine (Domitor, Nippon Zenyaku Kogyo, Fukushima, Japan), 0.5 mg/kg butorphanol (Vetorphale, Meiji Seika Pharma, Tokyo, Japan), and 0.5 mg/kg midazolam (Midazolam “Sandoz”, Sandoz, Tokyo, Japan) as an anesthetic. Subsequently, 40 rats were implanted with CPC/VCM and PMMA/VCM between the fascia and quadriceps on the left and right side, respectively. Immediately after suturing the fascia and skin, the rats were free to move around in their cages. Test specimens were extracted following animal sacrifice in weeks 4, 8, 12, and 24 (n = 10 each).
VCM extraction
To calculate the concentration of VCM released into rat tissues, remaining VCM in the test specimens was extracted from 5 out of the 10 removed specimens in each of weeks 4, 8, 12, and 24. For CPC/VMC, after grounding down the removed specimen in a mortar, 10 mg of the powder was added to 0.3 mL of 1 M hydrochloric acid and then 2.7 mL of water for dissolution. Chromatographic mobile phase solution was then added to dilute the solution 10-fold. For extraction from PMMA/VCM, the specimen was crushed using an osteotome, and 10 mg pieces were added to 3 mL of acetone for complete dissolution. Chromatographic mobile phase solution was added to dilute the solution 10-fold, before centrifuging at 5,000 × g for 5 min at 25 °C (#3700, Kubota, Tokyo, Japan) to remove precipitates. We also extracted VCM from test specimens that were not implanted as a reference (week 0). All extracted VCM was analyzed using high-performance liquid chromatography (HPLC) as described below.
VCM concentration
A range of VCM standard solutions of known concentration were made in phosphate-buffered saline (PBS) and applied to a CAPCELL-PAK C18 UG120 column (5 μm, 𝜑4.6 mm × h250 mm; Osaka Soda, Osaka, Japan) in an Elite LaChrom HPLC system (Hitachi High-Technologies, Tokyo, Japan) containing a L-2455 Diode Array Detector (Hitachi High-Technologies). HPLC was performed using a column temperature of 30 °C; mobile phase A comprising triethylamine buffer (pH3.2)/acetonitrile/tetrahydrofuran at a 92:7:1 (v/v) ratio; isocratic elution as phase A (20 min); flow rate of 1 mL/min; wavelength of 280 nm; and injection volume of 20 μL. To produce a calibration curve, the peak area of VCM was measured in each standard solution and graphed against the VCM concentration. The concentration of VCM in each test specimen was deduced using HPLC under the same conditions used for the standard solutions.
Antibacterial activity
Antibacterial activity was determined according to the Japanese Industrial Standards (JIS L 1902:2015), with some modifications, using the Halo Method [21]. S. aureus (NBRC 12732, Gram-positive bacterium) was used as the test strain. Freeze-dried bacteria were inoculated onto nutrient agar and incubated at 35 °C for 1 day. Subsequently, nutrient broth was inoculated with a single colony of bacteria and incubated at 35 °C for 18 h. A series of 10 mL of the Mueller-Hinton agar medium containing approximately 106 colony-forming units (CFU) of bacteria was poured into Petri dishes and cooled under a laminar airflow hood. A disc of filter paper (𝜑10 mm × t1.1 mm, ADVANTEC, Tokyo, Japan) that was soaked in a known concentration of VCM, used to produce a calibration curve to determine the correlation between VCM concentration and antibacterial activity, was placed on top of the agar and pressure was gently applied to make certain the disc made complete contact with the agar surface. Furthermore, the remaining 5 of the 10 test specimens removed from rats were placed directly onto the surface of the agar to confirm the antibacterial activity of releasable VCM. After incubating at 35 °C for 1 day, the diameter of the area in which inhibition was observed, referred to as the inhibition zone, was determined in each quintuplicate test and used to calculate the halo width (W) as follows:
In vivo release and antibacterial activity findings were analyzed using the Brunner-Munzel test as a non-parametric test without considering normality or variance. HAD software (version 16, Kwansei Gakuin University, Hyogo, Japan) was used for all statistical comparisons. p-values less than 0.05 indicated statistical significance.
Results
In vivo release
To determine the concentration of VCM released into rat tissues, the amount of VCM extracted from removed test specimens was subtracted from that extracted from reference specimens that were not implanted. Figure 1 shows the average amount of VCM released from 5 test specimens across a period of 24 weeks. CPC/VCM released significantly more VCM over a longer period of time than PMMA/VCM in vivo. Furthermore, CPC/VCM released 1.4 to 26.1-fold more VCM than PMMA/VCM at all time points (all p < 0.05).
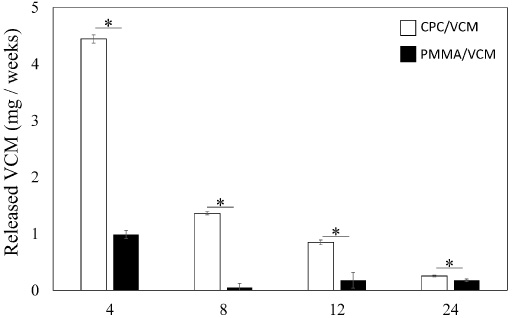
Amount of VCM released from CPC/VCM and PMMA/VCM in vivo at 4, 8, 12, and 24 weeks after implantation. Values are mean ± standard deviation in quintuplicate (*p < 0.05).
Calibration curve
Using HPLC, serially diluted concentrations of VCM prepared at 12.5, 25.0, 50.0, 100, 200, 400, and 800 μg/mL were actually determined to be 11.2, 22.9, 49.3, 102, 197, 393, and 793 μg/mL, respectively. These concentrations were plotted against the halo width obtained in the antibacterial test. We found a logarithmic correlation between VCM concentration and antibacterial activity (Fig. 2).
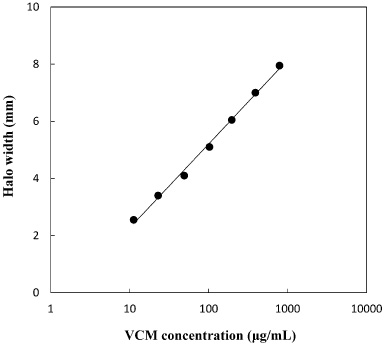
Calibration curve to determine the correlation between VCM concentration and antibacterial activity. Halo width was plotted against serial concentrations of VCM previously quantified by HPLC to be 11.2, 22.9, 49.3, 102, 197, 393, and 793 μg/mL.
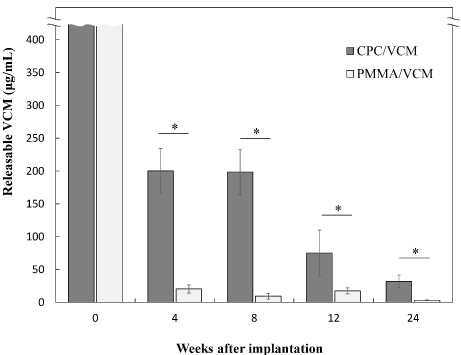
Removed test specimens were placed directly onto the surface of agar to determine the antibacterial activity of releasable VCM. Figure 3 shows images of the inhibition zone formed by released VCM. While the inhibition zone formed by VCM released from CPC/VCM and PMMA/VCM gradually shrank in size with time after implantation, the zone remained visible throughout the study. Figure 4 shows the locally releasable fraction of VCM in vivo in each week after implantation, calculated by converting the halo width values shown in Fig. 3 to VCM concentration using the calibration curve shown in Fig. 2. The concentration of releasable VCM in weeks 4, 8, 12, and 24 after implantation was 200 ± 34.3 μg/mL, 199 ± 34.7 μg/mL, 75.3 ± 34.8 μg/mL, and 32.0 ± 9.66 μg/mL for CPC/VCM and 20.3 ± 6.33 μg/mL, 9.30 ± 4.35 μg/mL, 17.4 ± 4.53 μg/mL, and 3.15 ± 0.595 μg/mL for PMMA/VCM, respectively. The concentration of releasable VCM in week 0 was significantly higher than that measurable using the calibration curve for both specimens. These results indicate that CPC/VCM can release significantly greater concentrations of intact VCM with antibacterial activity for longer periods of time than PMMA/VCM (p < 0.05, for all measured time points).
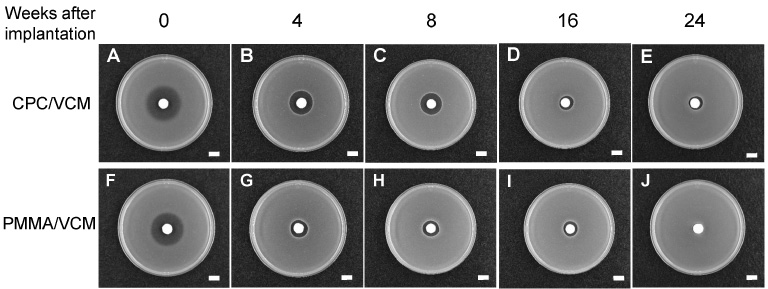
Images of the inhibition zone formed in the antibacterial test using S. aureus when VCM was released from test specimens removed in weeks 0 (A and F), 4 (B and G), 8 (C and H), 12 (D and I), and 24 (E and J). (A), (B), (C), (D), and (E) show the results for CPC/VCM and (F), (G), (H), (I), and (J) show those for PMMA/VCM. Scale bars: 10 mm.
PMMA is an amorphous polymer with a glass transition temperature (T g ) of approximately 105 °C, which undergoes a number of changes in physical property through the T g , such as increased permeability and fluidity [22]. Therefore, PMMA materials generally do not undergo a phase transition or diffuse additives at body temperature, resulting in limited release of hydrophilic drugs after an initial burst [23,24]. However, our findings indicate that PMMA/VCM releases hydrophilic VCM with antibacterial activity for at least 24 weeks in vivo. This result suggests that penetration and diffusion in PMMA/VCM may be enhanced in vivo by hydrophobic interactions between the polymers in PMMA and blood plasma, and partially by phagocytosis by macrophages recognizing the test specimen as a foreign body [25], to enable moderate-sustained drug release.
CPC/VCM released more VCM over a longer period of time across 24 weeks than PMMA/VCM in vivo, releasing 1.4 to 26.1-fold more VCM than PMMA/VCM throughout the experiment. Long-term evaluation revealed that CPC/VCM can release VCM even in a lower fluid volume environment in vivo. A previous study reported that the porosity of calcium phosphate composites influences the VCM release profile [26]. We previously reported that CPC and PMMA specimens had different pore size distributions, with mode values of 0.22 μm and 0.011 μm for CPC/VCM and PMMA/VCM, respectively [14]. The larger pore size in CPC may enable gradual release of VCM from deep within the specimen and explain why CPC/VCM can release greater concentrations of VCM with antibacterial activity for longer periods over 24 weeks than PMMA/VCM. The reconstruction surgery performed as part of the two-stage exchange procedure to treat periprosthetic joint infection is typically performed 6–8 weeks (or after 12 weeks or more in some cases) following debridement and antibiotic-impregnated cement implantation [16,17,27]. Our results indicate that while PMMA/VCM shows only moderate release, CPC/VCM is effective for facilitating antibiotic release for the necessary period in the clinic.
S. aureus were used as the representative bacteria in our antibacterial test as it is responsible for 80% of human osteomyelitis cases [28]. Antibacterial activity was logarithmically correlated with VCM concentration for the full concentration range tested (12.5–800 μg/mL). Because the Halo Method does not enable measurement of the inhibition zone below the width of the paper disc or test specimen, the detection limit corresponded to a halo width of 0 mm and a VCM concentration of 1.69 μg/mL, with values below these limits used to indicate negative antibacterial activity. We confirmed the antibacterial activity of releasable VCM from the removed test specimens by placing them directly onto the surface of agar and examining the inhibition zone. The released VCM produced a fuzzy inhibition zone in week 0 and sharp a zone thereafter in both groups that gradually shrank in size with time after implantation; however, the inhibition zone remained visible throughout the experiment. The halo width values shown in Fig. 3 were converted to VCM concentrations using the calibration curve shown in Fig. 2 to determine the locally releasable fraction in vivo in each week after implantation. The concentration of releasable VCM in week 0 (at least ≥800 μg/mL) in both groups was significantly higher than that measureable using the calibration curve. Fuzzy inhibition zone margins in week 0, as shown in Figs 3A and 3F, indicate delayed growth or lysis, where the shadows of bacterial colonies are present [29]. While fuzzy margins are generally considered a component indicating complete inhibition, it is possible that a drug-bacterial antagonistic reaction may be occurring at the fuzzy margin, indicating that the results are close to a plateau. The results of a previous investigation and our study indicate that VCM is stable inside cement materials, even in thermally-polymerized PMMA [30]. Furthermore, CPC/VCM was capable of releasing approximately 32.0 μg/mL VCM with antibacterial activity in week 24, while PMMA/VCM released less than 32.0 μg/mL VCM even early on in week 4, indicating that CPC/VCM can release significantly greater concentrations of intact VCM with antibacterial activity for longer periods of time than PMMA/VCM, and that PMMA/VCM would show little antibacterial effect against resistant strains with a minimum inhibitory concentration ≥32 μg/mL [31].
VCM has a narrow therapeutic index, the ratio of the toxic to effective dose of a drug. Treatment of an infection with an inadequate concentration of VCM can lead to the development of resistant bacteria [32]. In contrast, treatment with too high a dose can result in serious side effects, including hearing loss (ototoxicity) [33] and kidney damage (nephrotoxicity) [34,35]. Therefore, extended release of VCM using CPC may cause problems. Monitoring VCM levels is very important because its effectiveness relies on keeping blood levels above a minimum concentration for the entire duration of therapy [36]. Further investigations that monitor blood levels of VCM and CPC/VCM-transplanted sites are needed to determine the efficacy and safety of CPC/VCM.
Conclusions
CPC/VCM can release significantly greater concentrations of intact VCM with antibacterial activity for longer periods of time than PMMA/VCM, suggesting that CPC is a useful material for facilitating the release of local antibiotics for the treatment of established postoperative infection in clinical settings.
Footnotes
Acknowledgements
We would like to express our gratitude to the Food Research Laboratory, Tokyo Food Sanitation Association for their technical advice on the antibacterial test.
Conflict of interest
None to report.