
Abstract
BACKGROUND:
Portable blood glucose meters are the main method for detecting the blood glucose status of clinical patients.
OBJECTIVE:
To investigate the accuracy of detecting blood glucose in haemodialysis patients by sampling two blood glucose meters through the haemodialysis line.
METHODS:
Convenient sampling was used to select 80 patients with maintenance haemodialysis. The patients were sampled through the arterial end of the haemodialysis line within three minutes of being put on the machine. One specimen was tested by glycemeter1, which can identify the type of blood in the arteries and veins, and glycemeter2, which can only detect blood glucose in the capillaries for bedside blood glucose testing. The other specimen was sent to the laboratory biochemical analyser for blood glucose testing.
RESULTS:
When the blood glucose value of the first blood glucose meter (No. 1) was compared with the laboratory biochemical analyser, the correlation coefficient was r = 0.805 (p < 0.05), the out of value of the first blood glucose meter accounted for 4.4%, and the consistency reached 95% (p < 0.05). When the blood glucose value of the second blood glucose meter (No. 2) was compared with the laboratory biochemical analyser, the correlation coefficient was r = 0.800 (p < 0.05), the out of value of the second blood glucose meter accounted for 4.4%, and the consistency reached 95% (p < 0.05).
CONCLUSIONS:
For patients with maintenance haemodialysis, the blood glucose values detected by the two bedside blood glucose meters using arteriovenous mixed blood in the pipeline do not affect the accuracy and can respond more realistically.
Introduction
The portable blood glucose meter, in short referred to as the blood glucose meter, has the advantages of convenience and speed, and has become the main method for detecting the blood glucose status of clinical patients [1]. Glucose meters usually take capillary blood from fingers. Haemodialysis nurses also use this method to monitor blood sugar during dialysis to prevent hypoglycaemia [2]. Hypoglycaemia is one of the most dangerous complications of haemodialysis, and its incidence is as high as 16.9–47.6% [3,4]. Diabetic haemodialysis patients often need to collect finger capillary blood for blood glucose measurement during dialysis. Due to the heparinization of the whole body during haemodialysis, frequent finger punctures can cause problems such as subcutaneous stasis and difficulty in haemostasis [5,6]. In addition to pain, the patient’s compliance with blood glucose monitoring is reduced; the circulation of the fingertips is poor in patients with hypotension during dialysis, and the blood is diluted by tissue fluid when the fingertip is pressed too hard. All of these factors affect the accuracy of blood glucose monitoring. In haemodialysis, the patient’s blood continues to circulate in extracorporeal circulation, and there are sampling points on the pipeline.
In order to reduce the discomfort of the patient’s needle pricking blood collection and to increase the accuracy and convenience of blood glucose measurement, the arteriovenous mixed blood on the pipeline is used for the blood glucose meter to determine the blood glucose value at the bedside in our hospital at times. The results of individual test showed that the accuracy of using arteriovenous mixed blood on the pipeline was high. But is it accurate enough? Is the sensitivity related to the brand and function of the blood glucose meter? These questions need to be answered by further experiments.
Therefore, in this study, we used two types of blood glucose meters and considered maintenance haemodialysis patients from June 2019 to December 2019 as the main research object. The traditional finger capillary blood sampling was changed to the sampling point of the haemodialysis tube and uses the No. 1 blood glucose meter that can identify the type of arteriovenous blood and the No. 2 blood glucose meter that can only detect capillary blood sugar. By comparing the correlation and consistency between the two detection methods and the laboratory biochemical blood glucose value to verify the accuracy of blood sampling in the dialysis pipeline, thus provide new ideas for blood glucose monitoring during dialysis, and provide a more reliable theoretical basis for clinical nursing work.
Materials and methods
Research objects
This is a cross-sectional survey. The main research subjects are maintenance haemodialysis patients from June 2019 to December 2019. In order to explore the accuracy of bedside detection of the blood glucose values of haemodialysis patients by two blood glucose meters, the No. 1 blood glucose meter that can identify the type of arteriovenous blood, the No. 2 blood glucose meter that can only detect capillary blood glucose, and an automatic biochemical analyser were used to compare the blood glucose measured by the two blood glucose meters. There is no interest related to either of the two manufacturers of blood glucose meters used in this study. This study complies with the Declaration of Helsinki and has been approved by the ethics committee of Renji Hospital. All patients signed an informed consent form prior to participation.
Inclusion and exclusion criteria
Inclusion criteria: (1) Patients with maintenance haemodialysis ≥ three months and vascular access with arteriovenous fistula; (2) Older than 18 years old; (3) Patients who regularly undergo fasting for blood glucose laboratory biochemical testing; (4) Patients who can tolerate fasting for ≥4.5 hours on the day of blood glucose measurement; (5) Patients who have good cognitive ability and can cooperate to complete the research; (6) Patients who have signed an informed consent form.
Exclusion criteria: (1) Taking drugs that affect blood sugar during dialysis, such as: glucocorticoids, contraception drugs, anti-asthmatic drugs, anti-tuberculosis drugs, diuretics, adrenaline, antipsychotics, immunosuppressive drugs, etc.; (2) Suffering from mental or neurological diseases; (3) If patients fasting for more than 4.5 hours have hypoglycaemia symptoms or cannot tolerate fasting, timely oral glucose is recommended, they were not included in this study; (4) Patients with frequent hypoglycaemia recently; (5) Patients with incomplete case data.
Research methods
Assigned nurses were in charge of the operation of this study. Slow pump technology was used to collect 0.5 ml of blood from the sampling point of the dialysis pathway within three minutes of the patient being connected to the machine. Two nurses used two blood glucose meters to test at the same time, and immediately obtained two bedside blood glucose test values and recorded them separately.
The blood glucose test done by the biochemical laboratory in the hospital’s clinical laboratory was also conducted by nurses. The blood samples were collected from the sampling point of dialysis pathway within three minutes of the patient being connected to the machine. The samples were collected in biochemical laboratory test tubes and sent to the laboratory within 30 minutes. The biochemical team in the laboratory was responsible for maintenance, commissioning, quality control, calibration, traceability, and blood glucose measurement.
Statistical methods
In this study, Epidata software was used to enter and check the patient data, and SPSS 23.0 statistical software was used for statistical analysis. Measurement data was expressed as mean ± standard deviation. Counting data was expressed in percentages (%). As for correlation analysis, the two variables were linearly correlated, and Spearman’s correlation coefficient was used when it conformed to the bivariate joint skew distribution, ranging from −1 to 1. The larger the absolute value, the stronger the correlation. The consistency evaluation was analysed by the Bland–Altman method, and the degree of consistency of the two variables was evaluated according to the spread trend of the Bland–Altman diagram and the inner width of the consistency limit. P < 0.05 indicates that the difference is statistically significant.
Results
General information
In this study, a convenient sampling method was used to select 80 patients with maintenance haemodialysis in the hospital, including 43 males (53.75%) and 37 females (46.25%), aged 23–82 years old, with an average age of 61.93 ± 13.38 years old.
Correlation analysis between the blood glucose value of the No. 1 blood glucose meter and the laboratory biochemical blood glucose value
The results of this study showed that the blood glucose value measured by the No. 1 blood glucose meter at the bedside was 6.39 ± 2.99 mmol/L, and the laboratory biochemical blood glucose value was 5.83 ± 2.67 mmol/L. The results of the two detection methods have a significant correlation, and the correlation coefficient r = 0.805, P < 0.001. See Fig. 1 for details.
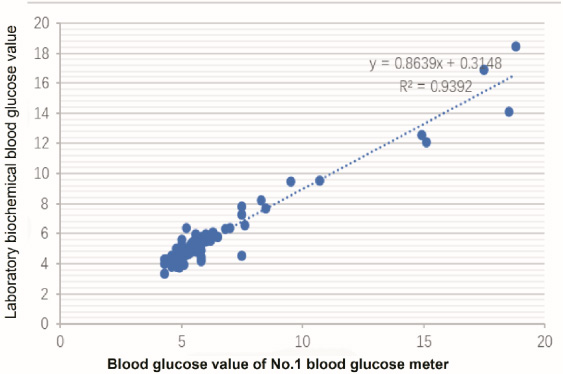
Correlation analysis between the blood glucose value of the No. 1 blood glucose meter and laboratory biochemical blood glucose value.
The difference between the blood glucose value of the No. 1 blood glucose meter and the average blood glucose value of the laboratory biochemistry is 0.55 mmol/L, the standard deviation of the difference is 0.77 mmol/L, and the 95% consistency limit is 0.55 ± 1.96 ∗ 0.77 mmol/L, which is (−0.96 mmol/L, 2.06 mmol/L). According to the Bland–Altman analysis result, 4.4% (6/137) points are outside of the 95% consistency limit; within the consistency limit, the maximum absolute value of the difference between the blood glucose value of the No. 1 blood glucose meter and the biochemical blood glucose value of the laboratory is 1.63 mmol/L, which is within an acceptable range. Therefore, it can be considered that the results of the two measurements are in good agreement (p < 0.05). See Fig. 2 for details.
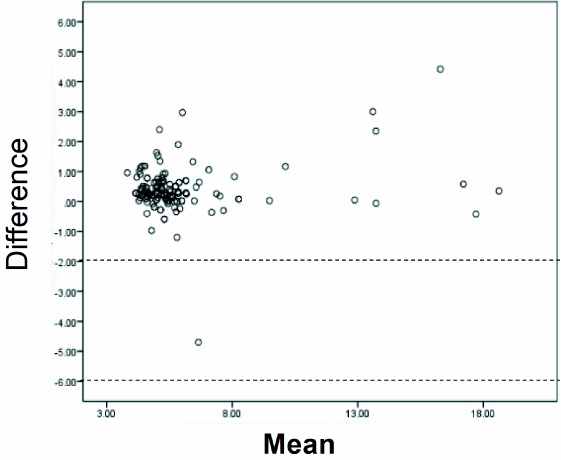
Bland-Altman chart of the blood glucose value of the No. 1 blood glucose meter and laboratory biochemical blood glucose value.
The results of this study showed that the blood glucose value of the No. 2 blood glucose meter was 6.80 ± 3.14 mmol/L, and the laboratory biochemical blood glucose value was 5.84 ± 3.00 mmol/L. The results of the two detection methods have a significant correlation, with the correlation coefficient r = 0.800 (p < 0.001). See Fig. 3.

Correlation analysis between the blood glucose value of the No. 2 blood glucose meter and laboratory biochemical blood glucose value.
The average of the difference between the blood glucose value of the No. 2 blood glucose meter and the laboratory biochemical blood glucose value is 0.97 mmol/L, and the standard deviation of the difference is 0.77 mmol/L, then the 95% consistency limit is 0.97 ± 1.96 ∗ 0.77 mmol/L, which is (−0.54 mmol/L, 2.48 mmol/L). According to the Bland–Altman analysis results, 4.4% (6/137) of the points are outside the 95% consistency limit; within the consistency limit, the maximum absolute value of the difference between the blood glucose value of the No. 2 blood glucose meter and the biochemical blood glucose value of the laboratory is 2.36 mmol/L. This difference is within the acceptable range, so it can be considered that the two measurement results have a good agreement (p < 0.05). See Fig. 4 for details.

Bland-Altman chart of the blood glucose value of the No. 2 blood glucose meter and laboratory biochemical blood glucose value.
According to the ‘Guidelines for the Prevention and Treatment of Type 2 Diabetes in China’ [7], biochemical analyser detection of venous plasma glucose is used as the diagnostic standard for diabetes and the calibration of the blood glucose meter. In previous studies, when it is necessary to measure whether a certain type of testing instrument or method is accurate, a biochemical analyser is often used as a comparison standard. Ye et al. [8] discussed the difference and correlation between the rapid blood glucose meter measuring venous whole blood glucose and the biochemical meter measuring venous plasma blood glucose. As a result, instead of peripheral blood, venous blood can be used to measure blood glucose. Therefore, in this research, laboratory biochemical blood glucose was used as the standard to test and measure the accuracy of the blood glucose values in the pipeline measured by the two blood glucose meters. Our results show that the blood glucose value of the No. 1 and No. 2 blood glucose meters are significantly correlated with the laboratory biochemical analyser. Therefore, the blood glucose values detected by the two types of blood glucose meters at the bedside can accurately reflect the patient’s blood glucose status.
The subjects of this study are all haemodialysis patients with autologous arteriovenous fistulas. Due to the particularity of arteriovenous fistulas [9,10,11], the blood samples obtained from the sampling port of the arterial end of the dialysis line are all arteriovenous mixed blood. The No. 1 rapid blood glucose meter in this study has its own calibration function, which can automatically identify arterial blood, venous blood, finger capillaries, and umbilical cord blood and detect blood sugar. Compared with the laboratory biochemical analyser, the blood glucose value of the No. 1 blood glucose meter is significantly correlated and the consistency reached 95%. The No. 2 blood glucose meter is one of the most widely used blood glucose meters in clinical practice. The instructions for use of the No. 2 blood glucose meter only apply to capillary blood. Compared with the laboratory biochemical analyser, the blood glucose value of the No. 2 blood glucose meter is significantly correlated, and the consistency is as high as 95%. Through this study, it was found that the correlation coefficients of the blood glucose values obtained by the two blood glucose meters and the biochemical analyser are both greater than 0.8, which is very strong; the consistency reached 95%, and is considered to be good. Therefore, although the scope of application of the two types of blood glucose meters is different, the measured blood glucose values at the bedside are accurate and reliable and can truly reflect the patient’s blood glucose status. This shows that the method of blood glucose monitoring in dialysis patients is not only suitable for the No. 2 blood glucose meter which can only recognize capillary blood, but also suitable for the No. 1 blood glucose meter which can recognize various types of blood and has complex functions.
If a biochemical analyser is used to measure blood glucose, the amount of blood collected is large, the measurement time is long, and the cost is relatively high [12,13,14,15]. In this study, the average waiting time for obtaining the blood glucose value from the laboratory is 98 minutes, which is not conducive to making timely and rapid judgments regarding the patient’s blood glucose changes during haemodialysis. Thus, among the 80 patients enrolled in this study, 95% tended to choose blood sampling through a dialysis pipeline to monitor blood glucose.
Various complex cases encountered in clinical practice will lead to inaccuracy of the fingertip blood sample monitoring of the portable blood glucose meter [16]. If the pathophysiological mechanism of severe patients is complicated, tissue ischemia and hypoxia, microcirculation disorder, application of catecholamine drugs or peripheral vascular disease, etc. can lead to insufficient peripheral perfusion, making it difficult to collect peripheral blood. Taking into account the various drawbacks of traditional blood glucose monitoring methods in haemodialysis, this study selected a dialysis pipeline as the sampling point. The Standard Operating Procedures for Blood Purification (SOP) 2020 Edition points out that biochemical tests such as renal function can be sampled through a dialysis pipeline (there is a red sampling port before the blood is drawn into the blood pump). Slow pump technology is used by slowing down the blood flow rate to 50–100 ml/min, maintaining it for 15 seconds so there is no recirculating blood in the arterial needle circuit and arterial blood circuit, and then slowing down the blood pump flow rate or turning off the blood pump. Blood sampling through the sampling port of a haemodialysis pipeline can reduce the pain caused by repeated fingertip puncture, which is conducive to improving the compliance of blood glucose detection and can be used as the sampling site for blood glucose detection in dialysis. Using dialysis pipeline sampling points to collect blood instead of interdigital capillary blood sampling can effectively reduce the patient’s pain and relieve tension. More importantly, blood sampling is more conducive to observing the occurrence of asymptomatic hypoglycaemia and can correct hypoglycaemia in a timelier manner.
This study still has a few shortcomings. First, this study is a cross-sectional study, not a randomised controlled experiment. Second, this study is a single-centre clinical study, and the sample size included is small. It is still necessary to increase the sample size and conduct multi-centre clinical research. Finally, this study only used the two most commonly used blood glucose meters in clinical practice. Whether it is suitable for all rapid blood glucose meters requires further research.
Strengths and limitations
In haemodialysis, the patient’s blood continues to circulate in extracorporeal circulation, and there are sampling points on the pipeline. In order to reduce the discomfort of the patient’s needle pricking blood collection and the increase the accuracy and convenience of blood glucose measurement, the arteriovenous mixed blood on the pipeline is used for the blood glucose meter to determine the blood glucose value at the bedside in our hospital at times. The results of individual test showed that the accuracy of using arteriovenous mixed blood on the pipeline was high. But its accuracy and sensitivity need more results of test to verification, and the relation of its accuracy and function of the blood glucose meter also need further experiments to explore.
In order to verify the accuracy, and explore the relation of the accuracy and function of the blood glucose meter, we used two types of blood glucose meters and considered maintenance haemodialysis patients from June 2019 to December 2019 as the main research object in this study. The traditional finger capillary blood sampling was changed to the sampling point of the haemodialysis tube and uses the No. 1 blood glucose meter that can identify the type of arteriovenous blood and the No. 2 blood glucose meter that can only detect capillary blood sugar. By comparing the correlation and consistency between the two detection methods and the laboratory biochemical blood glucose value to verify the accuracy of blood sampling in the dialysis pipeline, thus provide new ideas for blood glucose monitoring during dialysis, and provide a more reliable theoretical basis for clinical nursing work.
Conclusion
For the maintenance of haemodialysis patients, whether it is the No. 1 blood glucose meter that can identify the type of arteriovenous blood, or the No. 2 blood glucose meter that can only detect capillary blood glucose, the blood glucose values measured by them using the arteriovenous mixed blood in the pipeline do not affect the accuracy and can respond more realistically. The method of blood glucose monitoring in dialysis patients may be suitable for a variety of blood glucose meters.
Footnotes
Author contributions
Conception and design of the research: Zhang HF. Acquisition of data: Lai LSH, Zhao L. Analysis and interpretation of the data: Zhao SY. Statistical analysis: Liu Q, Fang NN. Obtaining financing: None. Writing of the manuscript: Zhang HF. Critical revision of the manuscript for intellectual content: Zhang HF, Yang Y. All authors provided final approval of the version to be published.
Conflict of interest
None of the authors have any personal, financial, commercial, or academic conflicts of interest related to this work.