
Abstract
BACKGROUD:
Calcium phosphate biomaterials have excellent bone inductivity, and exercise can promote the bone formation of biomaterials in animals, but it is not clear which exercise mode is better.
OBJECTIVE:
To explore the effect of different exercise modes on osteoinduction by calcium phosphate-based biomaterials which were implanted in mice.
METHOD:
The collagen-thermosensitive hydrogel-calcium phosphate (CTC) composite was prepared and transplanted in the thigh muscle of mice, then all mice were divided randomly into four groups (n = 10): the uphill running group, the downhill running group, the swimming group and the control group (conventional breeding). Ten weeks later, the samples were harvested, fixed, decalcified, embedded in paraffin and stained with hematoxylin and eosin (H&E), and then the osteoinduction phenomenon was observed and compared through digital slice scanning system. The area percentage of new bone-related tissues and the number of osteocytes and chondrocytes were counted and calculated. Lastly, the immunohistochemistry of type I collagen (ColI) and osteopontin (OPN) was performed to identify the new bone tissues.
RESULTS:
The area percentage of new bone-related tissues and the number of osteocytes and chondrocytes were positively correlated; ordering from most to least of each group were as followings: the uphill running group > the swimming group > the downhill running group > the control group. The immunostaining of ColI and OPN results showed that both of the two proteins were identified in the new bone tissues, indicating that the CTC composite could induce ectopic bone formation in mice, especially training for uphill running and swimming.
CONCLUSION:
Our results show that uphill running or swimming is a form of exercise that is beneficial to osteogenesis. According to this, we propose treatment with artificial bone transplantation to patients who suffer from bone defects. Patients should do moderate exercise, such as running uphill on the treadmill or swimming.
Introduction
Artificial bone with excellent hardness and elastic modulus is urgently needed to repair the large segments of bone defects; meanwhile, the abilities of osteoconduction and osteoinduction are also very important for artificial bone [1,2]. Among them, osteoconductivity refers to the ability of the material to allow bone to grow into the process without being hindered, and osteoinductivity refers to the ability of the material to induce bone formation when it is implanted into non-osseous sites in the absence of osteogenic factors. The recruitment and migration of osteoblasts to the defect sites is related to the osteoconductivity of the material, and bone induction leads to the differentiation of osteoblast derived cells into osteoblasts to form new bone [3–5]. Calcium phosphate bioceramic is a kind of excellent artificial bone material, which has been widely used in animal experiments and clinical practice because of its similarity to natural bone inorganic components in recent years [6–8]. However, the traditional calcium-phosphorus ceramics are fragile with limited repair effect. At the same time, based on the influence of chemical composition and surface structure of the materials on the osteoinductivity [4], more and more calcium-phosphorus matrix composites have emerged, such as compositing with metallic elements [9], metal [10] and polymer [11]. In our previous study, one collagen-thermosensitive hydrogel-calcium phosphate (CTC) composite has been shown to have proper pore size and porosity, excellent hardness and water absorption, which was used to fill the load-bearing bone defects (4 mm-tibia defects) in mice, and the results showed that the CTC composite had excellent mechanical properties, osteoinductivity and load-bearing capacity [12]. Therefore, we would also apply this material to explore the effect of different exercise modes on osteoinduction in this study.
After bone repairing surgery, recovering bone health is crucial for patients, especially in the first two months. It has been shown that a moderate physical activity could aid in the treatment of bone damage [13,14]. Various exercises are considered to have the effect of stimulating bone growth and preserving bone mass, which is the best non-drug treatment, prevention and postoperative rehabilitation measures for some diseases. For example, certain exercise plans could help strengthen bone and prevent further bone loss in patients with osteoporosis [15,16]. Exercise could promote bone formation through the Wnt signaling pathway through boosting immunity in mice, and the proper exercise is beneficial to the recovery of bone damage [17]. In this regard, it is of profound significance to explore a better way of exercise and a suitable program for bone healing. Among all types of exercise, running in endurance sports and swimming in non-weight bearing exercise are two popular ways to keep fit nowadays, controlling the duration and intensity of both the two exercise also works for people fresh from surgery. However, not all exercise training is beneficial to bone repair. For example, low-intensity exercise may have no significant effect on bone healing [18], while excessive or strenuous exercise may cause secondary injuries after orthopedic surgery. So how to define moderate exercise? Especially after bone grafts. In 2020, the world health organization’s guidelines on physical activity and sedentary behavior recommend that all adults, including those with chronic diseases or physical disabilities, should undertake 150–300 min of moderate-intensity, or 75–150 min of vigorous-intensity physical activity, or some equivalent combination of moderate-intensity and vigorous-intensity aerobic physical activity, per week [19]. According to this guideline, running or swimming for 60 min of moderate-intensity for five consecutive days, and then rest for two days across one week is appropriate. Nevertheless, based on the characteristics of each disease and the treatment plan, different orthopedic diseases should have more accurate and appropriate exercise.
In this study, the CTC composite will be implanted into the muscle of mice, combined with swimming or running training of moderate-intensity after surgery to compare the osteoinductivity of material with the help of different exercise modes; in order to provide experimental basis for orthopedic patients to exercise after operation.
Materials and methods
Material preparation
The thermosensitive hydrogel (PLGA-PEG-PLGA polymer, Daigang Biomaterial, China) was dissolved in double distilled water to form the hydrogel solution, then the type I collagen from rat tail (Sigma-Aldrich, USA) was added into hydrogel solution, next, the tricalcium phosphate powder (Sigma-Aldrich, USA) was weighed and mixed with aforementioned mixture, to get a collagen-thermosensitive hydrogel-calcium phosphate (CTC) mixture, and the final ratio of the CTC composite was 25% collagen:15% thermosensitive hydrogel:60% calcium phosphate. Lastly, this mixed slurry was poured into the mold and got solidification at 37 °C, then crosslinked with 2.5% glutaraldehyde, washed with 95% alcohol, freeze-dried at −20 °C. The chemical characteristics and surface structures of the composites were measured by X-ray diffraction (XRD), scanning electron microscopy (SEM) and energy dispersive spectrometer (EDS). The composites were fabricated into Φ2 × 4 mm cylinders and steam-sterilized at 121 °C for 15 min before implantation.
Animal surgery
Forty BALB/c mice were purchased from Dossy Biological Technology Company (Chengdu, China). All animals were maintained in a temperature and light-controlled environment ventilated with filtered air. All animals were anesthetized with an intraperitoneal injection of pentobarbital sodium. The hair on both thighs was removed using an electric shaver and the skin underneath was disinfected with 75% ethanol, and then an approximately 10-mm muscle pouch was made which was parallel to the femur. Finally, a Φ2 × 4 mm CTC composite was implanted into the muscle pouch of the left and right thighs. Lastly, the incised muscle and skin were closed with nylon sutures, and penicillin was injected intramuscularly to prevent infection lastly. The Animal Care and Use Committee of Chengdu University approved the study. The operative procedures and animal care were performed in compliance with NIH guidelines on the care and use of laboratory animals, under the supervision of a licensed veterinarian.
Animal exercise
Firstly, forty mice with material implantation in muscle were divided randomly into four groups (n = 10) three days after surgery: the uphill running group, the downhill running group, the swimming group and the control group. In the two running groups, all mice were trained to run 6 m/h for 30 min on a treadmill per day, a total of three days without slope to get used to the intensity of the exercise. In the second week after surgery, the treadmill was set to a 5-degree upward sloping (the uphill running group, group 1) and a 9-degree downward sloping (the downhill running group, group 2), five mice were put on the treadmill to run for 60 min as 6 m/h speed for five consecutive days, and then rest for two days, a total of eight weeks. In the swimming group (group 3), all mice swam for 30 min per day, a total of three days to get used to the intensity of the exercise in a heated mouse swimming pool at 25 °C, then 60 min per day for five consecutive days, and then rest for two days, a total of eight weeks. In group 4, all mice were regularly fed without any treatment. The schematic diagram of animal grouping is shown in Fig. 1.
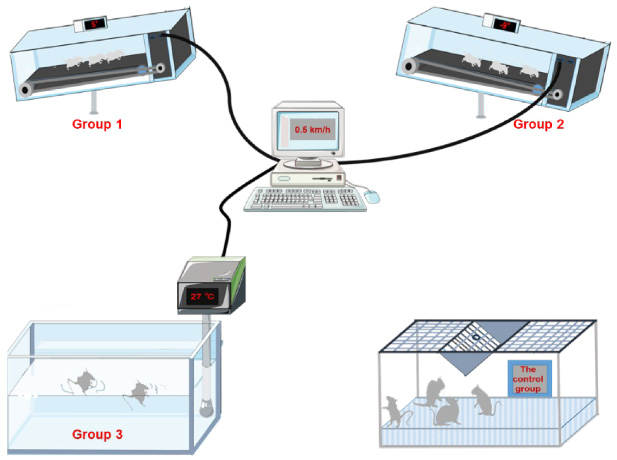
Schematic diagram of animal grouping: the uphill running group (group 1), the downhill running group (group 2), the swimming group (group 3) and the control group (group 4).
The samples were harvested at post-operative week 10. They were immediately fixed in 10% neutral formalin buffer solution for approximately 24 h at room temperature, decalcified in 10% ethylenediaminetetraacetic acid (EDTA), pH 7.0, for about 20 days at room temperature, washed with diethyl pyrocarbonate (DEPC) water, dehydrated and embedded in paraffin. The embedded samples were cut into 5 μm thick histological sections and transferred onto 3-aminopropyrytrietoxy silane-coated glass slides. The sections were stained with hematoxylin and eosin (H&E), ultimately scanned with the NanoZoomer Digital Pathology software.
Histomorphology
The osteoblasts and osteocytes were counted and analyzed using IPP (image pro plus) software; meanwhile, the areas of the new bone, cartilage, bone marrow and total tissues were measured, and the area percentage of new bone-related tissues (including new bone, cartilage and bone marrow tissues) was calculated as: new bone-related tissue area/total tissue area. The number of osteocytes and chondrocytes were also counted in the new bone and cartilage tissues.
Immunohistochemistry
The expression of type I collagen (ColI) and osteopontin (OPN) was analyzed by immunostaining. The sections were blocked through enzyme digestion, and then retrieved with a Tris–EDTA buffer (pH 9.0) in a 95 °C water bath. Next, the specimens were incubated with a mouse monoclonal antibody against ColI (1:1000, Abcam) and OPN (1:1000, Abcam), and a horseradish peroxidase (HRP)-labeled secondary antibody. Finally, they were developed with 3,3 ′ -diaminobenzidine (DAB) and counterstained with hematoxylin.
Statistical analysis
Data were expressed as means ± standard deviation and analyzed by paired ANOVA (SPSS version 13.0, SPSS, USA). A P < 0.05 was considered statistically significant.
Results
The characteristics of materials
The prepared collagen-thermosensitive hydrogel-calcium phosphate (CTC) composites were grinded to a fine powder in a mortar and passed through a 320-mesh sieve, and the chemical components were detected by XRD and analyzed by the software Jade 6.0. The results presented the main components of the CTC composite in XRD spectrum according to the software analysis (Fig. 2A), which was consistent with our previous study [12]. The composite was also observed under SEM after spraying with gold–palladium. The results showed that the pore size of the composite ranged from 20 to 100 μm (Fig. 2B); compared with SEM images of pure calcium phosphate materials, the SEM images showed that the thermosensitive hydrogel were mixed with calcium phosphate in the composite (Fig. 2C). The elemental analysis was also performed by EDS, which showed Ca, P, C, O, N elements in the CTC composite (Fig. 2D). In addition to this, the volumetric porosity of CTC composite was approximately 36.25%, the water absorption was about 87.38%, and the Shore hardness was approximately 94.35 based on our previous study [12].
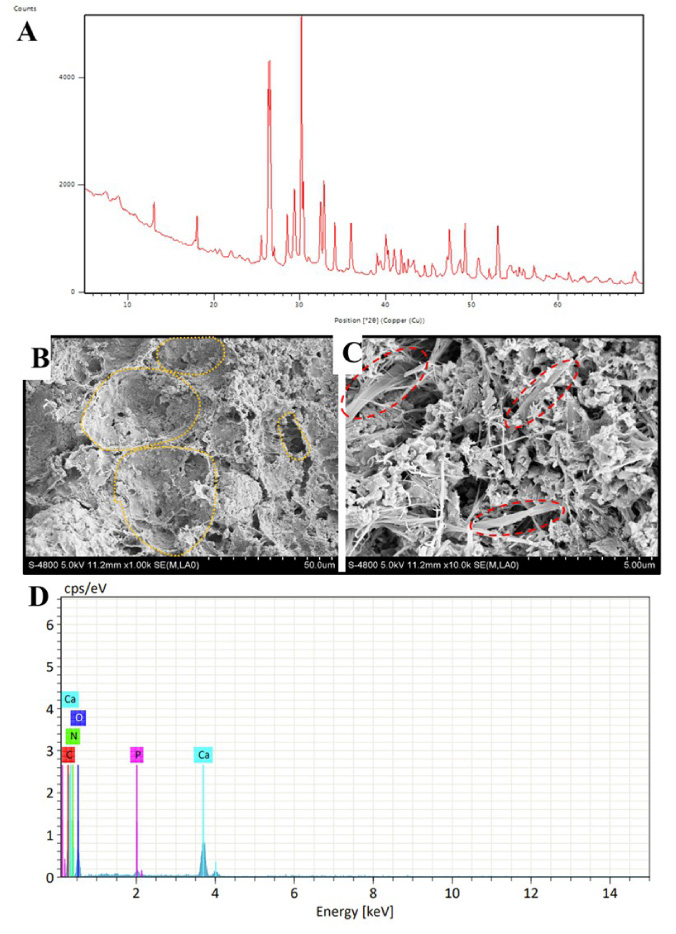
The physicochemical characteristics of CTC composite. (A) XRD spectrum, the peaks showed the main components in the composite according to the Jade software analysis. (B) SEM microstructure picture showed the pores with different size, most of them ranged from 20 to 100 μm. Yellow dotted box: pores. (C) The 10 times enlarged structure of Fig. 2B, which showed the hydrogel were mixed with calcium phosphate in CTC composite. Red dotted box: hydrogel. (D) The element energy spectrum of CTC composite was analyzed by EDS, Ca, P, C, O, N elements were analyzed.
After 10 weeks of training or conventional feeding, all animals were killed and the samples were harvested to perform histological staining. The HE staining indicated that the new bone tissues were induced in all groups, but the area percentage of new bone were significant different in the four groups. Lots of bone marrow tissues and mature bone tissues were observed in the uphill running group and the swimming group, meanwhile, a small number of new bone tissues were also induced in the downhill running group and the control group (Fig. 3A). Based on the results of IPP software, ordering from most to least of the area percentage of new bone-related tissues was as followings: the uphill running group > the swimming group > the downhill running group > the control group, which were (32.83 ± 7.92)%, (29.28 ± 6.53)%, (6.59 ± 1.38)% and (1.21 ± 0.22)%, respectively. Consistent with the area percentage of new bone-related tissues, the number of osteocytes and chondrocytes was 228 ± 35, 49 ± 12, 214 ± 43, 12 ± 3, respectively (Fig. 3B). The results showed that the area percentage of new bone-related tissues, the number of osteocytes and chondrocytes in group 1 and 3 were significantly higher than that in the control group (∗ P < 0.05), suggesting that uphill running and swimming could promote new bone formation of biomaterials in mice.
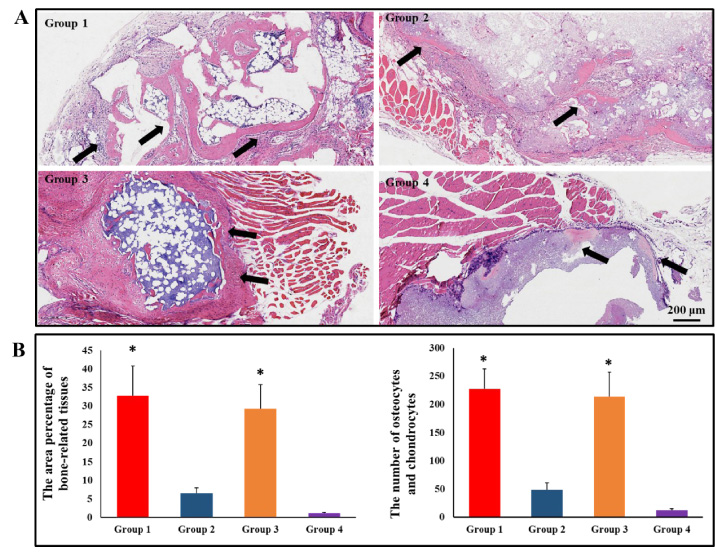
Bone induction of CTC composite in the four groups. (A) HE micrographs showed newly formed bone tissues, cartilaginous tissue, bone marrow tissues in the four groups, arrow: new bone tissues; bar: 200 μm. (B) The area percentage of new bone-related tissues and the number of osteocytes and chondrocytes counting based on HE staining sections, *P < 0.05.
The typical HE staining sections of group 1 was selected to analyze the osteogenic process, and we found that the process of osteoinduction with biomaterials could be divided into four stages: (1) Inflammation stage, lots of inflammatory cells appeared after the wound occurrence caused by transplantation surgery, such as lymphocytes, macrophages, dendritic cells, natural killer cells, etc. during this stage (Fig. 4A). (2) Angiogenesis stage, the bone formation was closely associated with angiogenesis, which could provide nutrients for new bone tissues (Fig. 4B). (3) Preosteogenic stage, some osteoid, cartilage, immature bone tissues appeared in this stage, which also determined whether osteogenesis is intramembranous or endochondral (Fig. 4C). (4) Osteogenic stage, mature bone tissues and bone marrow tissues formed and replaced the degraded materials gradually, the osteocytes also embedded in bone tissues (Fig. 4D). All these results indicated that moderate exercise could reduce inflammation, promote angiogenesis, and ultimately lead to the formation of large amounts of bone tissues, to promote the recovery of bone injury diseases as soon as possible.

The four stages of osteoinduction analyzed with HE staining. (A) Inflammation stage, (B) angiogenesis stage, (C) preosteogenic stage, osteoid (left) and cartilage (right), (D) osteogenic stage. Bar: 200 μm.
The type I collagen (ColI) and osteopontin (OPN) are two key indicators in the mineral bone, so we chose them to identify new formed bone tissues. The immunostaining of ColI and OPN results showed that both of the two proteins were identified in the new formed bone tissues, while the un-degraded materials are nonspecifically stained. On the contrast, the blank control is not colored (Fig. 5).
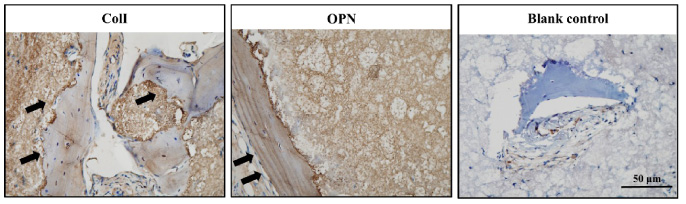
Immunohistochemistry of ColI and OPN showed both of the two proteins were expressed in the mineral bone. Arrow: target proteins. Bar: 50 μm.
Nowadays, sedentary behaviors could increase the risk of cardiovascular disease, type 2 diabetes, Alzheimer’s disease, cancer, and postoperatively delayed recovery [19]; therefore, the best way is to do moderate exercise every day. Exercise refers to planned, organized, and repetitive body movements performed to improve and maintain one or more parts of the body [20]. Among children and adolescents, an average of 60 min/day of moderate-to-vigorous intensity aerobic physical activity across the week provides health benefits. But for patients undergoing surgery, exercise of moderate-intensity would be more appropriate [21]. The authors took into account convenience and environmental factors, running on the treadmill and swimming in the swimming pool were selected as the exercise modes in this experiment. The common running styles include level running, uphill running and downhill running, which might have different effects on cardiorespiratory responses [22,23], muscular fatigue [24], endurance performance [25], etc.; however, few studies have shown the effects of different running styles on bone repair. Therefore, we compared the effects of osteoinduction between uphill running and downhill running, and the results showed the amount of new bone tissues in uphill running group was significantly higher than that in downhill running group, the reason might be that uphill running could promote the expression of some osteogenic factors, such as bone morphogenetic proteins (BMPs) and vascular endothelial growth factor (VEGF) [26,27]. Swimming is a non-weight-bearing exercise that reduces joint injuries by 90% compared to land exercise, which is suitable for the elderly, pregnant women and patients in the healing stage [28]. The study indicated that non-weight bearing exercise such as swimming had no effect on bone mass, while running had certain positive effect on bone mass [29], and the swimming could also promote osteoinduction to form more bone tissues, whose effect was similar to uphill running. And the sequence of osteoinduction effects is as follows: uphill running > swimming > downhill running > no exercise. The specific mechanism will be explored in future research.
Osteoinduction is biomaterial inducing bone formation at non-osseous sites in animals without the addition of any osteogenic biomolecules [5,30], which was related to osteogenesis, and could indirectly reflect the ability of bone repair [12,31,32]. Although this study investigated the osteoinduction properties of calcium-phosphorus based composites, it could also indirectly reflect the bone repair ability of the composites to a certain extent. The area percentage of new bone-related tissues was consistent with the number of osteocytes and chondrocytes, which could also determine the ability of osteoinduction. There are four stages of osteogenic process during osteoinduction, that is, inflammation stage, angiogenesis stage, preosteogenic stage and osteogenic stage; during the preosteogenic stage, we found that the occurrence of osteoid and cartilage at random, so the osteoinduction of biomaterials is a combination of intramembrane osteogenesis and endochondral osteogenesis. The biomaterials with excellent osteoinduction would be beneficial to bone repair, which would also be an excellent bone replacement material.
Conclusion
The collagen-thermosensitive hydrogel-calcium phosphate (CTC) composites have excellent osteoinductivity when they were implanted in the muscle of mice, and the ability of osteoinduction would be enhanced when combined with appropriate exercise, such as uphill running or swimming. Our study provides a proposal to patients who suffer from bone defects and artificial bone transplantation: do moderate exercise, such as running uphill on the treadmill or swimming in a swimming pool.
Footnotes
Acknowledgements
This work was supported by the Health Research Project of Health Department of Sichuan Province, China (19PJ161), Medical Scientific Research Project of Chengdu City, China (2021043), and Entrepreneurship training program for college students in Sichuan Province, China (S202111079028, S202111079043X, S202111079095, S202111079124X and S202111079041). The authors thank the Institute for Advanced Study, Chengdu University for the EDS analysis.
Conflict of interest
The authors report no conflicts of interest in this work.