
Abstract
BACKGROUND:
The marginal adaptation of root-end filling materials and the effective antibacterial control in a surgical site are crucial for the successful outcome of endodontic surgery.
OBJECTIVE:
This study aimed to evaluate the effect of retrograde application of photodynamic therapy on the marginal adaptation of Biodentine used as a root-end filling material.
METHODS:
Twenty single-rooted anterior teeth were selected, instrumented and obturated with gutta-percha and AH Plus. The apical 3 mm of the roots were resected and root-end cavities were prepared with an ultrasonic retro-tip. The teeth were randomly divided into two groups (n = 10). In the first group, photodynamic therapy (PDT) was applied in the retrograde cavity prior to the root-end filling. In the second group retro cavity was filled without PDT. All specimens were obturated with Biodentine and afterwards sectioned longitudinally. The gap width at the material-dentin interface was measured using a scanning electron microscope. The results were statistically analyzed.
RESULTS:
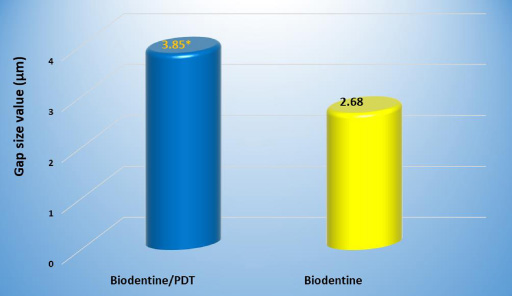
The produced gap width by Biodentine/PDT was 3.85 μm versus 2.68 μm in the Biodentine control group with significant differences in-between.
CONCLUSION:
Under the conditions of this study, PDT has a negative effect on the marginal adaptation of Biodentine used as root-end filling material.
Introduction
Apical surgery is an important branch of modern endodontics and is a reliable therapeutic alternative in case of failure of conventional endodontic treatment. The causes of failure can be attributed to bacterial invasion from inadequate cleansing or obturation of the root canal system, procedural errors or extra radicular biofilm [1,2]. In case of persistent peri-radicular pathology when retreatment via an orthograde route is unsuccessful or unfeasible, apical surgery is indicated [3].
Since the periapical surgical procedure is now more routinely performed using the surgical operating microscope, microsurgical and ultrasonic instruments, it is also referred to as endodontic microsurgery [4]. The prognosis and long-term success of endodontic surgery depends on many factors, such as case selection, instrumentation technique, suitable equipment, the clinician’s qualification, skill and experience, and the age of the patients [5,6].
Setzer et al. identified the following possible reasons for failure of endodontic surgery: inadequate root-end filling, missed anatomy, and incomplete resection [7]. Therefore, the choice of the appropriate retrograde filling material plays a critical role. One of the most important requirements for this material is the ability to achieve the hermetic apical seal of communication between the pulp and periodontium in order to prevent the percolation of tissue fluids and microorganism penetration via the apical foramen [3,8].
Historically, a wide range of materials have been applied for obturation of the retrograde cavity. Recently, calcium-silicate cements (CSCs) have been considered an ideal root-end filling material due to their specific properties. They may provide not only an excellent and effective physical sealing, but also a biological seal due to their ability to form newly mineralized tissues [9–11].
Teeth with inadequate root canal treatments and periapical lesions usually harbor persistent obligate anaerobic microorganisms [5]. It is crucial during apical surgery procedures to influence the available infection and prevent re-infection by achieving the three-dimensional hermetic seal of the apical area [1,4]. Recently, along with the conventional medicaments and devices for standard antibacterial irrigation protocol, some new modern systems and techniques designed to improve the intracanal bacterial decontamination by a specific chemical action, such as photodynamic therapy (PDT), ozone therapy, and direct laser action, were introduced [12–14].
Photodynamic therapy has been proposed as a new adjunctive method for additional disinfection of the root canal system using a specific light source like a laser or light-emitting diode acting over a photosensitizer (PS) and thus liberating reactive oxygen and/or free radicals that eliminate a wide range of persistent gram-positive and gram-negative microorganisms, especially Enterococcus faecalis. One very important advantage of PDT is its activity inside the dentinal tubules [15,16].
Several studies on the antimicrobial effectiveness of PDT have been conducted [15,17,18] but its impact on the retrograde marginal adaptation of calcium-silicate cements in the dentin-cement interface so far has not been investigated. Considering the lack of research in this area, this study aimed to evaluate and compare the marginal adaptation of Biodentine used as root-end filling material in different testing condition - with or without preliminary disinfection of the retrograde cavity using PDT. Based on previous reports on the effectiveness of this method, the accepted null hypothesis stated that there was no significant difference in the gap size values produced by Biodentine associated with PDT and Biodentine used per se.
Materials and methods
Sample construction
A total of 20 freshly extracted human maxillary anterior teeth were collected and used in this study, obtained from the Department of Oral and Maxillofacial Surgery. A pre-selection of single-rooted teeth was performed by clinical observation and preliminary radiographs in different projections for further assessment to confirm the single canal of roots and the absence of internal resorption, calcification, and cracks.
The inclusion criteria for the teeth were: (1) single root and patent single canal with minimum apical diameter of size 15 K file; (2) completely formed roots with closed apex (3) straight root without curvature; (4) an intact pulp chamber. The exclusion criteria were: (1) fractured roots or with open apices; (2) calcified root canals; (3) teeth with root curvature; (4) prior root canal treatment; (5) internal or external resorption; (6) severe caries or large coronal restoration; (7) visible evidence of cracks on examination.
After extraction, the teeth were fixed in 10% buffered formalin for 2 weeks. Then they were cleaned using an ultrasonic scaler and Gracey curettes (Hu-Friedy, Leimen, Germany) to remove remaining soft tissues and calculus, and afterwards were immersed in a mixture of 2.6% sodium hypochlorite and 3% hydrogen peroxide for 24 hours. Finally, they were rinsed under tap water and stored in a 0.2% thimol solution before use.
Root canal preparation
A standardized endodontic access cavity was made in each tooth using a high-speed Endo access diamond bur followed by an Endo-Z bur (Dentsply Sirona, Ballaigues, Switzerland). The working length (WL) was determined at 1mm shorter than the apical foramen to ensure an instrumentation of the root canal to the apical constriction. A size 10 and 15 K files were used to establish a reproducible glide path.
The root canal shaping was performed with ProTaper Gold nickel-titanium rotary instruments (Dentsply Sirona, Ballaigues, Switzerland) at the established WL up to size F3/0.09 file using X-Smart TM Plus Endomotor and handpiece (Dentsply Maillefer, Ballaigue, Switzerland) according to the manufacturer’s protocol. A size 10 K file was used to maintain apical patency between rotary file insertions.
During instrumentation, after each rotary file, root canals were repeatedly irrigated with 2.5% NaOCl (Medicinos Linija UAB, Siauliai, Lithuania). The smear layer was removed using 17% EDTA (IMICRYL, Konya, Turkey), 40% citric acid (Cerkamed, Stalowa Wola, Poland) and final flush with distilled water. The instrumented canals were dried and filled using a single cone technique with F3/0.06 gutta-percha points ProTaper Universal (Dentsply Maillefer, Ballaigues, Switzerland) coated with epoxy resin root canal sealer AH Plus (Dentsply DeTrey GmbH, Konstanz, Germany).
Postoperative radiographs were made to evaluate the filling quality. The obturation procedure was repeated when a lack of homogeneity was observed. The coronal access of all specimens was sealed with light cured composite resin material 3M Filtek TM Z250 Universal Restorative (3M ESPE Dental Products, St. Paul, MN, USA).
Root-end cavity preparation
The apical 3 mm of all specimens were resected perpendicular to the long axis of the tooth using a high-speed Lindemann surgical carbide bur (Dentsply Sirona) under continuous water cooling. The retrograde cavities were performed with a universal micro retrotip P14D (Acteon Satelec, Mérignac, France), intended for the preparation of canals in anterior teeth (diamond-coated 30 μm, length 5 mm, taper 7%), using piezoelectric ultrasonic device Suprasson P5 Booster (Acteon Satelec, Mérignac, France). The cavities were prepared on all teeth parallel to the long axis of the tooth to a depth of 3 mm and diameter of 1.2 mm with light pressure in a brushing motion with constant irrigation. The root-end cavity dimensions were checked with the help of graduated William periodontal probe (R&S Dental Products, Paris, France) and hand plugger (Dentsply Maillefer, Tulsa, OK, USA).
The study was conducted in two groups of 10 teeth in each:
Group 1 – Biodentine/PDT: In this group a PDT was applied as a complementary technique, which contributes to additional disinfection prior to obturation of the cavity with Biodentine.
Group 2 – Biodentine per se: In this group the retro cavity was rinsed only by 2 mL of normal saline, dried, and obturated with Biodentine, and thus served as a control group.
Photodynamic therapy
In the first group a photodynamic therapy with photosensitizer toluidine blue O - FotoSan Agent (CMS Dental, Copenhagen, Denmark) in low viscosity with concentration of 0.1 mg/ml, was performed immediately before the placement of Biodentine. The PS (0.2 ml) was inserted into the retrograde cavity by syringe with bendable application tip 22 G. Afterwards, red light was applied by using a LED light source FotoSan 630 (CMS Dental, Copenhagen, Denmark) to activate the chemical. Since toluidine blue O (TBO) absorbs light at a wavelength of 630–638 nm, the applied wavelength was 630 nm and the output intensity of the LED diode was 2,000-4,000 mW/cm2. According to the manufacturer instruction the light was applied to each tooth twice for 30 seconds using endo tip of 0.5 mm diameter which was introduced into the root-end cavity [19]. After irradiation, the photosensitizer was washed out of the cavity with 2 ml of normal saline and dried by paper cones.
The retrograde cavities were obturated with Biodentine (Septodont, Saint-Maur-des-Fossés, France). Biodentine was prepared in an amalgamator according to the manufacturer‘s instructions. Five drops of liquid were added to predosed capsule that was placed on a capsule mixer GC Silver Mix (Dubai Medical Equipments, UAE) at a speed of 4000 rotations/min for 30 seconds. After mixing, the cement was inserted into the retrograde cavity in increments using MAP One syringe (Micro-apical Placement system, Produits Dentaires SA, Vevey, Switzerland), and lightly compacted vertically to the level of resected root surface with hand pluggers (Dentsply Maillefer, Tulsa, OK, USA) and absorbent paper points #60–70 (Meta Biomed, Korea). Binocular magnifying lenses Labo-clip (Eschenbach, Nürnberg, Germany) with ×2.5 magnification were used by the operator.
In group 2, PDT was not performed and the retrocavity was rinsed only with 2 mL of normal saline and dried. Afterwards, they were also obturated with Biodentine using the aforementioned technique. After removing the access material from the apical surface, all teeth were stored in an incubator at 100% humidity at 37 °C for 24 hours to allow the filling materials to set. All procedures were performed by one researcher. In the next step, the teeth were sectioned longitudinally in a mesiodistal direction through the center of the material using a slow-speed diamond disc (PHM, Plovdiv, Bulgaria) under copious amounts of water spray.
Scanning electron microscopy (SEM) analysis
Thereafter, all specimens were mounted on aluminum stubs, gold sputtered and examined under high-vacuum scanning electron microscope (SEM) TM4000, (Hitachi, Tokyo, Japan) at an accelerating voltage of 15 kV and analyzed at different magnifications – from ×30 to ×1000 to verify marginal adaptation of Biodentine. The magnification ×1000 was chosen to be the most suitable for measuring the gap size in the dentin-material interface. The images obtained at magnification ×30 were divided mentally into 3 equal parts and four symmetrical points were chosen and magnified at ×1000 (Fig. 1A). The extent of the gap (distance between the dentine wall and cement) was evaluated and measured to the nearest 0.0x μm at another four equidistant points on these new micrographs by relevant software (Fig. 1B). Overall, 16 measurements for each sample were made, i.e. 160 measurements per group and the mean gap width was calculated.
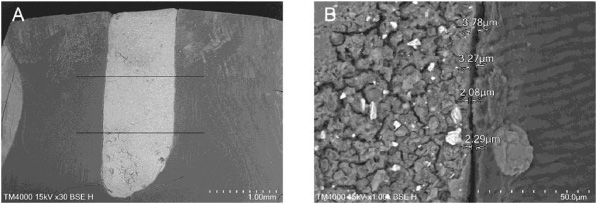
Representative SEM photomicrographs: (A) the retro cavity filled with Biodentine and divided into three parts (magnification ×30); (B) measurements of the gap size at other 4 points (×1000).
All data were entered and processed with the statistical package SPSS Statistics v. 25.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics (mean, standard error, standard deviation, confidence interval) were used to evaluate the gap size produced by Biodentine in the two groups. The results were also subjected to the following tests: (1) nonparametric test of Shapiro–Wilk to check the normality of the distribution of the data; (2) Levene test to check the homogeneity of the variance; (3) student’s independent samples t-test to evaluate the significance of the differences between the groups; (4) nonparametric Mann–Whitney U test for comparison between two independent samples; (5) graphical analysis to visualize the results. 𝛼-level was set at 0.05 and P-value less than 0.05 (p < 0.05) was considered statistically significant.
Results
The SEM examination of the samples’ longitudinal sections showed that gap sizes produced by Biodentine at the material-dentinal wall interface varied under different testing conditions. No specimens without a gap were recorded. The descriptive statistics concerning the marginal gap mean width values in the both groups as well as the statistical differences between them are summarized in Table 1 and presented in Fig. 2.
Gap size values (in μm) produced by Biodentine depending on the PDT application (p = 0.002)
Gap size values (in μm) produced by Biodentine depending on the PDT application (p = 0.002)
∗Different superscript letters indicate intergroup statistically significant difference (p < 0.05); SD – standard deviation.
Comparison of the marginal adaptation (gap size in μm) of Biodentine in the two groups.
The mean value of the gap width found in the Biodentine/PDT group was 3.85 ± 0.85 μm and in the Biodentine without PDT group—2.68 ± 0.35 μm with statistically significant differences in-between (p < 0.05). The statistical analysis of the overall results showed that Biodentine with PDT produced a larger gap size with a maximum value of 5.04 μm and a minimum value of 2.48 μm per specimen, whereas in the Biodentine control group, these values ranged from 1.90 to 3.17 μm. Representative photomicrographs for the gap size in both groups are shown in Fig. 3. Moreover, in some specimens of the second group, zones with barely noticeable gaps even at ×1000 magnification with minor size were detected (Fig. 4).

Representative SEM micrographs of gap width (magnification ×500) produced by (A) Biodentine/PDT; (B) Biodentine per se.

Representative SEM micrographs of Biodentine control group with minor gap size (A) at magnification ×500; (B) at magnification ×1000.
Recently, photodynamic therapy has been used to eliminate microorganisms of the root canal system in vitro and in vivo [15–17]. This study evaluated and compared the marginal adaptation of Biodentine used as root-end filling material after application of the final disinfection protocol with FotoSan 630 LAD System for PDT. The method is called Light Activated Disinfection (LAD) and according to the manufacturer is very efficient in infection control within the fields of periodontology and endodontics [19]. To the best of the authors’ knowledge, this is the first experimental in vitro study investigating the effect of the retrograde application of photodynamic therapy prior to the root-end filling on the marginal adaptation of Biodentine in terms of gap width.
Biodentine, relatively new synthetic tricalcium silicate-based material, is developed on the basis of unique Active Biosilicate Technology as a bioactive dentine substitute. It refers to the 3rd generation of calcium-silicate cements and is one of the main representatives of the bioceramics group [20,21]. Overall, recently, Biodentine is probably the most tested calcium-silicate cement. It is claimed that it is superior to other CSCs due to its exceptional properties in terms of sealing ability, marginal adaptation, high mechanical strength, improved handling characteristics, short working time, etc. [22–24].
According to some recent investigations, Biodentine can be considered the best root-end filling material [25–27]. Moreover, according to Nica et al. concentric areas of diffuse penetration of Biodentine into the dentinal tubules were observed, surrounding almost the entire contour of the root-end cavity [28]. For these reasons, Biodentine was chosen for the purposes of this study.
Only a few studies evaluating the marginal adaptation of Biodentine used as root-end filling materials were found in the literature as the established results by various researchers were very divergent as absolute values. Bansal et al., compared retrograde marginal adaptation of Biodentine with ProRoot MTA and MTA Plus and found the least margin gap of 2.44 μm with Biodentine at the interface, whereas maximum gap score of 5.63 μm was observed in the group of ProRoot MTA [29]. These results are consistent with those found in the present study in regard to Biodentine applied per se (control group).
Bolbolian et al. confirmed the superiority of Biodentine used as root-end filling material in comparison with other CSCs. Unlike other researchers, they measured and calculated on resin replicas not only the size of transverse gaps but also the size of longitudinal gaps. Biodentine exhibited the best marginal adaptation in the longitudinal section, followed by RetroMTA and ProRoot MTA (4.49 μm, 8.55 μm, and 14.34 μm, respectively), with statistically significant differences between the three groups [25]. The gap width of Biodentine found in this study is approximately twice as wide as that measured by us in the control group, and even larger than that of Biodentine/PDT group.
Other researchers registered significantly lower average gap size values produced by Biodentine in retrograde cavities. Soundappan et al. reported a gap size of 1.446 ± 0.367 μm. In contrast to most researchers, they found that ProRoot MTA (0.792 ± 0.201 μm) was superior when compared to Biodentine [30]. In another study Bolhari et al. evaluated the marginal adaptation of four root-end filling materials (MTA, CEM cement, Biodentine and BioAggregate) in the presence and absence of blood on epoxy resin replicas of the apical portion of samples, without longitudinal sections. They reported that there was no significant difference between the four cements. Biodentine specimens, in particular, which were exposed to fresh whole human blood, showed a gap size of 1.58 μm versus 0.5 μm gap size produced by specimens exposed to normal saline [31].
In a recent study Vanti et al. found lowest mean marginal gap of 0.46 μm seen with Biodentine and highest marginal gap of 0.83 μm seen with MTA Angelus. Additionally, they suggested that root-end preparation done using ultrasonics showed best marginal adaptation of the CSCs than preparation done using diamond points [32]. The results found in the present study were significantly higher than those reported by most of the aforementioned researchers [30–32], in which gap width ranged from 0.5 to 1.58 μm and were not consistent with them.
The quality of marginal adaptation is of great importance because it may have an indirect or direct correlation with the sealing ability of retro-filling materials. In clinical conditions it may depend on exposure of the materials to irrigants, intracanal medicaments, blood or different tissue fluids with an acidic pH as a result of periradicular inflammation. In laboratory conditions, the material may also be exposed to different immersion media such as simulated tissue fluids (STF) in order to mimic more closely the clinical environment [30,33].
There is no consensus yet in the dental literature regarding the influence of environmental conditions on the physicochemical properties of CSCs. The results found by different researchers are equivocal or even divergent [34–36]. In particular, the impact of the PDT has not been investigated so far.
According to some researchers, blood contamination does not affect the sealing ability and marginal adaptation of Biodentine used as root-end material [31,37]. Conversely, Salem Milani reported that exposure to blood during setting has a negative effect on retrograde marginal adaptation of MTA compared to STF-exposed MTA [38]. Moreover, Shalabi et al. found that blood contamination resulted in significant reduction of bond strength values of Biodentine and affected negatively the amount of apatite deposition on the material surface and interfacial spaces [39].
In the present study the control group in which the retrograde cavity was rinsed only with normal saline showed better marginal adaptation of Biodentine. Interestingly, in similar testing conditions, contrary to our results, Thakkar et al. found that the control group of Biodentine irrigated with 0.9% normal saline showed maximum leakage at all the time intervals (24 hours, 4th day and 7th day) in comparison with the groups where the retrograde cavity was irrigated with 7% Maleic acid or Irritrol [40].
In general, in this study we found that PDT affected negatively the marginal adaptation of Biodentine used as root-end material and definitely increased the gap width. A probable reason for this could be the incomplete removal of the photosensitizer toluidine blue from the retrograde cavity. These remnants may represent a barrier between the dentin and Biodentine, thus interfere with the good adaptation of the cement to the cavity walls. One of the limitations of PDT is that PS is a viscous substance that impregnates the dentine surface, thus forming a chemical smear layer, which can lead to microleakage and a decrease in the bond strength of root filling materials to dentine [41]. Moreover, PDT was unable to remove the smear layer in any of the root areas [42].
In the present study, the photosensitizer provided consisted of a toluidine blue O solution (Fotosan Agent® in Low viscosity) at a concentration of 0.1 mg/ml. It is available in three different viscosities (low, medium, and high), all with the same concentration of active ingredient. The low-viscosity PS is intended for endodontic application [19] and one might assume that it washes out of the root canal most easily. The manufacturer does not report what other ingredients the FotoSan Agent contains, what amount of water is needed to wash it off completely, and what its pH is. Only in one previous study do researchers state that the high-viscosity FotoSan Agent consisted in a TBO solution dissolved in 1% xanthan gel [43].
The question of whether Biodentine and TBO interact chemically also arises. On one hand, toluidine blue (tolonium chloride) is a basic thiazine metachromatic dye of the quinone-imine family widely used in histology and clinically. It is cationic and acidophilic in nature with high affinity for acidic tissue components such as DNA, sulfates, carboxylates, and phosphate radicals [44]. Toluidine blue basically has 3 isoforms, namely, ortho-toluidine, para-toluidine, and meta-toluidine. Toluidine Blue Ortho (TBO) is available as a powder and is partially soluble in both water and alcohol [45]. It is used in dentistry for PDT as a photosensitizer due to its in vitro efficiency, low toxicity to human cells, and high rate of reactive oxygen species generation. Its transmembrane permeability coefficient is higher than that of other PS solutions, a fact that possibly makes TBO more effective in bacterial destruction [46].
Biodentine, on the other hand, produced a high alkaline pH as calcium-silicate cement [20]. Being basic in nature, according to the Lewis theory of acid-based reactions, TBO cannot interact with another base [47]. Therefore, from a chemical point of view, it could not interfere with the Biodentine setting process and its marginal adaptation at the material-dentin interface. Atmeh et al. investigated the interfacial properties of Biodentine and found a formation of tag-like structures alongside an intermediate layer called the mineral infiltration zone, where the alkaline caustic effect of the cement’s hydration products degrades the collagenous component of the interfacial dentin. This process leads to the formation of a porous structure which facilitates the permeation of high concentrations of Ca(2+), OH(−), and CO(3) (2−) ions, leading to increased mineralization in this region [48].
Conclusion
Within the limitations of the present study, the gap width produced by Biodentine per se was superior to that of Biodentine/PDT. The analysis of the results clearly shows that the photodynamic therapy has a negative effect on the retrograde marginal adaptation of this bioceramic material. The clinician should carefully consider the advantages and disadvantages of application of this technique during apicoectomy. Further research is needed to assess whether PDT has the same effect on other calcium-silicate cements.
Footnotes
Acknowledgements
The authors would like to thank the laboratory technicians at the Scanning Electron Microscopy Laboratory, University of Sofia, Bulgaria.
Conflict of interest
None to report.
Funding
None to report.