
Abstract
BACKGROUND:
It is of great significance to understand the effect of the different corrosion behaviors of magnesium (Mg) alloys manufactured using different casting methods and implanted with different methods on the long-term implantation to expand the application of Mg-based biomedical implants.
OBJECTIVE:
The effects of four different casting and rolling speeds on the microstructure of an Mg–rare earth (Mg–Re) alloy were analyzed using electron backscatter diffraction (EBSD).
METHOD:
Four Mg alloys were obtained using vertical two-roll casting (TRC) at 10 m/min, 16 m/min, 24 m/min, and 30 m/min, and their microstructure, corrosion behavior and bone reaction in vivo were studied.
RESULTS:
The corrosion resistance of the alloy increases with an increase in casting speed and finer grain size of the cast-rolled parts. The Mg–Re alloys with TRC-10 m/min and TRC-30 m/min were selected for animal experiments. The two Mg alloys were made into metal rods and inserted into the rat femur to simulate the effect of Mg–Re on femoral healing under an injury condition. The rods were implanted for a long time to judge the effects of the Mg–Re alloy on the body. The TRC-30 m/min implants obtained highly mature new bone tissue in the case of bone injury.
CONCLUSION:
The in vivo experiments showed that the corrosion resistance of the TRC-30 m/min implant was better than that of the TRC-10 m/min implant. After 32 weeks of implantation, there were no pathological changes in the liver, heart, or kidney of rats in the TRC-30 m/min group, and the cell structure was normal.
Introduction
In recent years, magnesium (Mg) alloys as metal matrix biomaterials have attracted the attention of scholars, and in vivo and in vitro studies have shown that they exhibit biocompatibility, undergo a biodegradation process that does not produce toxic metal ions, are absorbed by the human body [1], do not trigger systemic inflammatory responses, and do not affect the blood cell composition [2–5]. In vitro cytological experiments have also shown that Mg alloys have no inhibitory effect on the growth and differentiation of mouse bone marrow cells, and they enhance the adhesion function of osteoblasts [6–8]. The above characteristics indicate that Mg and its alloys are promising new absorbable internal fixation materials with no toxicity and no immunogenicity. However, in most cases, Mg-based alloys with large grain sizes and many grain boundaries (GBs) are significantly limited in their application because of significant grain boundary corrosion [9,10]. Optimizing the microstructure of Mg-based materials is an effective method to improve the corrosion resistance of materials. For example, casting or deformation processes can improve the corrosion resistance of Mg-based alloys by refining grains and optimizing the secondary phase distribution [11,12]. However, it is difficult to obtain superfine, nanocrystalline, and even amorphous biodegradable Mg alloys using traditional casting techniques.
Compared with the traditional casting process, two-roll casting (TRC) may be an effective method for the preparation of ultrafine, nanocrystalline, or amorphous structural materials because of its fast solidification rate. Previous studies have shown that the vertical TRC process can produce biodegradable Mg-based materials with nanostructures or amorphous structures [13,14]. Additionally, Wang et al. [15] demonstrated the effect of casting process parameters on the microstructure and corrosion resistance of an Mg alloy; for example, in a 12-week in vivo experiment, an Mg–rare earth (Mg–Re) alloy with a faster casting speed promoted more extensive femur growth than the other alloys tested. However, in those studies, the surgery was performed with healthy bones. Therefore, further experimental studies are needed to determine whether Mg–Re has therapeutic effects on the clinical healing of fractures or bone injuries. Additionally, in clinical animal experiments, the degradation of an Mg alloy and the impact on internal circulation over long-term implantation is still very limited. A specific amount of elemental Mg in the body can promote the normal metabolism of bone and regulate the metabolism of hormones. However, excessive intake of Mg ions and exclusion disorders can lead to hypermagnesia [16–18], which can lead to the imbalance of human hormone regulation [19], liver and kidney diseases, and eventually neuromuscular and cardiovascular system abnormalities. Severe cases can lead to death [20]. Therefore, it is of great significance to understand the effect of the different corrosion behaviors of Mg alloys manufactured using different casting methods and implanted with different methods on the long-term implantation to expand the application of Mg-based biomedical implants.
The effects of four different casting and rolling speeds on the microstructure of an Mg–Re alloy were analyzed using electron backscatter diffraction (EBSD). For in vivo experiments, two representative Mg alloys, TRC-10 m/min and TRC-30 m/min, were used to make metal rods that were directly inserted into the femur of rats, and micro-CT and histological data were monitored at different times. This study aimed to provide ideas for the efficient preparation of Mg–Re alloys, and to evaluate the corrosion and bone reaction of the two Mg–Re alloys in vivo and their long-term effects on the circulation in rats for their potential application as biomaterials.
Experimental methods
Materials preparation
The experimental Mg–Re material was prepared using a copper mold casting method. Pure Mg, magnesium–aluminum–zinc alloy (AZ31) ingot, magnesium–10lanthanum (Mg–10La), and magnesium–cerium (Mg–20Ce) (in wt.%) were used as raw materials. The melting process was conducted in an electronic resistance furnace under the protection of a CO2 and sulfur hexafluoride (SF6) gas mixture. The TRC experiments were based on a vertical TRC with a roll width of 100 mm, roll radius of 150 mm, and roll gap of 0 mm. When the alloy was melted completely, the melt was introduced into the roll gap between the left and right rolls via an asbestos casting nozzle. To avoid further grain growth, the cast sheet was dipped into an oil tank under the rotating rolls to quickly solidify the alloy. In this study, four casting and rolling speeds of 10 m/min, 16 m/min, 24 m/min, and 30 m/min were used.
Implant method
All animal experiments were reviewed by the Animal Care and Use Committee of the Saitama Institute of Science and Technology (Approval No. 2021-1). Twenty rats (Wistar, male, 20 weeks of age, 330 ± 15 g) were selected from the School of Medicine, University of Tokyo and randomly divided into four groups. Owing to limited experimental conditions, two representative materials with a minimum speed of 10 m/min and maximum speed of 30 m/min were selected for animal experiments. In this study, unthreaded and uncoated smooth cylindrically shaped pins were used. The 10 m/min and 30 m/min Mg–Re rods with a diameter of 2 mm and length of 7 mm were implanted into the femoral fixation model of rats in group 1 and group 2, respectively. The third group of rats without implants served as the control group. Implants were sterilized with ethylene oxide before surgery. The implantation process is shown in Fig. 1. First, the right hind limb of each rat was shaved and sterilized, and an incision of approximately 20 mm was marked in the dorsolateral right hind limbs, as shown in Fig. 1(a). Subsequently, screw holes were drilled in the rat femur and disinfected, as shown in Fig. 1(b). A metal rod was attached to the bone, as shown in Fig. 1(c). Finally, the fascia was sutured to the muscle, and the skin was sealed with a non-absorbable metal needle. Daily clinical observation was performed after implantation. Postoperative behavioral abnormalities of pain and distress, and food and water intake were observed. Intramuscular injection of buprenorphine hydrochloride (0.01–0.05 mg/kg three times a day for one week) and carprofen (5 mg/kg every week for four weeks) analgesics were used to suppress postoperative pain. Penicillin was used to prevent postoperative infection (0.2 mg/kg three times a day for one week).
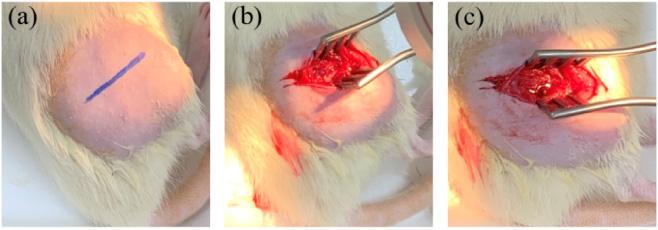
Main stages of the Mg–Re implant surgery of Wistar rats: (a) marking, (b) screw holes were created in the rat femur, and (c) a metal rod was attached to the bone.
EBSD electron microscopy (scanning electron microscopy – SEM, Gemini300, Germany and EBSD, C-Nano, Oxford, UK) was used to characterize the microstructure of the samples, and Channel 5 analysis software was used to analyze the EBSD results.
Micro-CT and histological assessments
After 2, 8, 16, and 32 weeks of implantation, 3D models of the femur and metal plates (R. M-CT, Rigaku, Tokyo, Japan) were created using micro-CT (R. M-CT) to assess new bone formation. The microstructure of the right femur was measured. Trabecular volume/tissue volume (BV/TV) parameters were quantified using Bone-J software [6].
In vivo degradation tests
At 8, 16, and 32 weeks after implantation, the central part of the right femur of rats was removed, and the cross section at the intersection of the implant and femur was observed using SEM and energy dispersive spectroscopy (EDS). According to the elemental composition of the cross section, the corrosion of the two Mg–Re alloy rods in the rat and promotion of femoral growth were evaluated.
Histological observation
At 8, 16, and 32 weeks, the heart, liver, and kidney of the experimental groups were removed. Histological sections of the heart, kidney, and liver were evaluated by routine paraffin embedded formalin and eosin (H&E) staining of 4-μm thick slices.
Serum diagnosis
At 4, 8, 16, and 32 weeks, 10 ml of blood was collected from the heart of each rat. The blood was centrifuged and 3 ml of the serum supernatant was sent to Yeast Industry Co., Ltd., Japan for serum diagnosis to categorize the physiological health of the rats.
Results and discussion
Microstructures
EBSD was used to study the microstructure evolution of TRC-10 m/min, TRC-16 m/min, TRC-24 m/min, and TRC-30 m/min Mg alloys in the RD, TD, and ND directions. The compression directions RD, TD, and ND are the rolling, transverse, and normal directions, respectively. Figure 2 shows the reverse pole map (IPF) plots for the RD, TD, and ND samples. The IPF diagram shows the Mg alloy prepared by vertical TRC and the microstructure from the direction along the RD, TD, and ND. The colors in the figure indicate the orientation of the compression axis with respect to the local lattice according to the IPF triangle. Dynamic recrystallization occurs with a decrease in the casting speed.
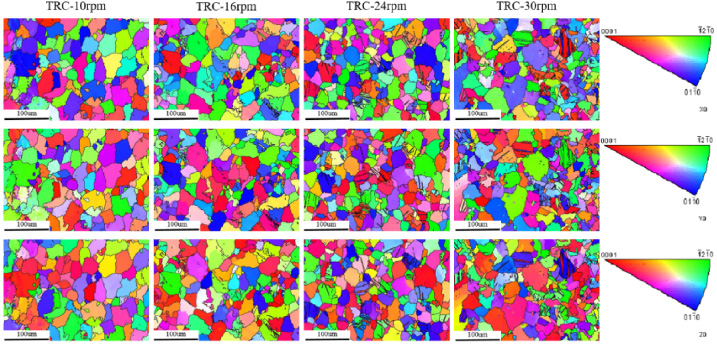
EBSD micrographs of the four magnesium alloys.
As shown in Figs 3a-3d, the average grain size of the alloy decreased from 29.2 μm to 25.5 μm with an increase in casting speed. As shown in Figs 3e–3h, the low-angle grain boundary (LAGB) decreased from 53.8% to 38.3% with an increase in casting speed. Previous studies showed that, the local orientation errors in the grain led to higher corrosion rates. The larger the LAGB value, the larger the local orientation error. In the absence of local orientation error, the grain orientation had limited influence on the corrosion rate [21]. The GB orientation deviation of the Mg alloy decreased with an increase in the casting speed. Therefore, the TRC-10 m/min alloy had the highest corrosion rate and the TRC-30 m/min alloy had the lowest corrosion rate among the four Mg alloys.

(a–d) Grain size distribution and (e–h) grain boundary orientation deviation.
Figure 4(a) shows representative 3D micro-CT reconstruction images of the rat femur 2, 8, and 16 weeks after the operation. The two Mg alloy implants remained in place, and the white part was bone and metal. A small amount of callus formation was observed at 8 weeks compared with 4 weeks after surgery. In the TRC-10 m/min group, the space around the metal rod was filled with new bone at 24 weeks; however, compared with the original bone, the growth was incomplete. In the TRC-30 m/min group, new bone formation was observed near the metal rod 8 weeks after surgery, and the space around the metal rod was completely filled with new bone at 16 weeks.
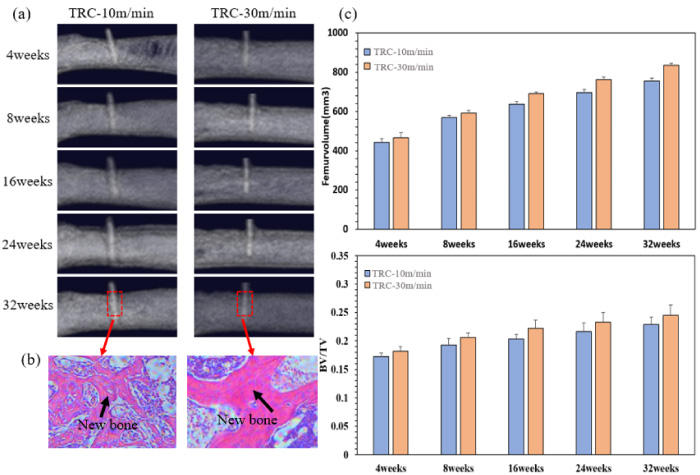
(a) Representative 3D micro-CT reconstructions showing the bone response of the TRC-10 m/min and TRC-30 m/min Mg–Re alloy implants at 4, 8, 16, 24, and 32 weeks after surgery. The red box is the area of interest. (b) After 32 weeks in vivo, decalcified sections were stained with hematoxylin and eosin (H&E) to visualize the morphology of the original bone and new bone around the implant. (c) Statistical analysis of the femoral parameters according to the horizontal section of interest. BV/TV: bone volume/tissue volume.
Figure 4(b) shows a stained section of rat femur 32 weeks after the operation. The bone is pink and the bone marrow is purple. The section site is the area where the metal rod was fixed (red dashed box in 4a). The damaged part of the femur fixed with the TRC-10 m/min Mg alloy produced new bone tissue, which is still growing and has not formed a complete new bone structure. The damaged part of the femur fixed with the TRC-30 m/min Mg alloy produced a large amount of bone tissue, and a relatively mature new bone structure was formed.
As shown in Fig. 4(c), a large amount of new bone tissue was formed at both interfaces of the Mg alloys, and the direction of bone formation was toward the implant. The increases in periosteum formation and new bone volume were similar for the two Mg alloy groups. When the mean quantitative parameters of bone morphometry were evaluated, the BV/TV values were greater in the TRC-30 m/min group, indicating a higher intensity of new bone formation in this rat model. Previous studies have confirmed that Mg2+ can promote osteocyte adhesion and bone tissue growth for new bone formation [22–24]. However, with the degradation of Mg-based materials, excessive ion release can inhibit the formation of new bone tissue [25], and hydrogen produced in the corrosion process can lead to tissue separation [26]. According to the EBSD analysis of several alloys, the degradation rate of the TRC-30 m/min Mg alloy is less than that of the TRC-10 m/min Mg alloy, possibly because of the high corrosion resistance of the TRC-30 m/min Mg alloy, which leads to a relatively low release rate of Mg ions. Therefore, the Mg alloy of the TRC-30 m/min group better promoted new bone formation than the TRC-10 m/min Mg alloy.
The in vivo experimental results confirmed that the internal implant material stimulates the local tissue to form new bone as the magnesium alloy degrades to produce Mg2+, which helps the damaged part to heal, and a second operation is not required to remove the implant. From this perspective, the performance of magnesium alloy as an internal implant material is better than that of titanium alloy.
Figure 5a shows a representative sample of the intersection of the TRC-10 m/min Mg–Re alloy rod and femur 8 weeks after implantation in the rat femur, and the results of the surface EDS line scan analysis. There is a clear boundary of element distribution in the sample, which is approximately 50 μm to the left of the starting point of the line sweep. On the left side of the Mg–Re alloy of the sample, the Mg content is very high, and the content of other elements, such as Ca, P, and O, is low. The distribution of Mg elements decreases sharply as it approaches the boundary 50 μm to the left of the sample, and the distribution amplitude of Mg elements in the corrosion layer changes greatly, indicating that the Mg–Re alloy at the junction is seriously corroded and uneven. On the right side of the femur, the content of Mg continued to decrease slowly; however, the Ca and P content increased significantly, which is consistent with the hydroxyapatite composition of bone. In addition, the content of O is slightly greater near the junction, which may be attributed to an oxide layer at the boundary. The content of elements, such as C and Ce on both sides of the sample, is still evenly distributed, and there is no obvious boundary. Figure 5b shows the results of the surface EDS linear scan analysis of the intersecting part of the TRC-30 m/min Mg–Re alloy rod and femur 8 weeks after implantation in a rat femur. Elements similar to Fig. 5a had different trends; however, in the samples on the left side of the Mg–Re alloy, the Mg element was close to the fast distribution of the Mg alloy in a lower leg junction. Alternatively, as shown in Fig. 5a, the extent of the corrosion layer of the Mg element distribution was slight, indicating the junction of the Mg–Re alloy corrosion is not serious and very even. On the side of the femur, the content of Mg in both samples slightly increased approximately 10 μm away from the junction, which may indicate a small amount of Mg diffused into the femur.
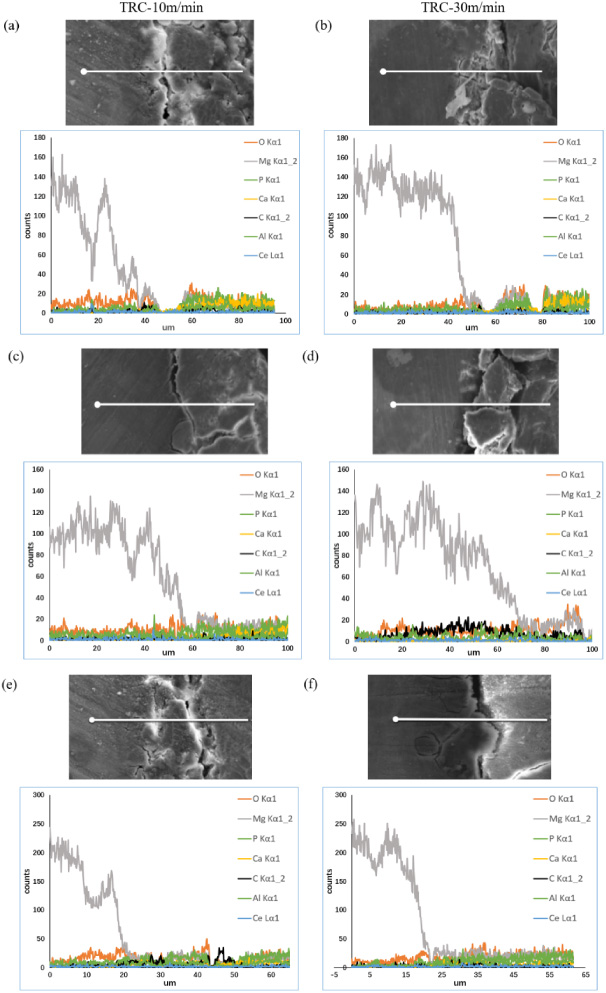
EDS line scanning observations of the (a, c, e) TRC-10 m/min and (b, d, f) TRC-30 m/min magnesium alloys and intersecting bone sections at 8, 16, and 32 weeks of implantation.
Figure 5c shows the results of the surface EDS linear scan analysis of the sample at the intersection of the TRC-10 m/min Mg–Re alloy rod and femur 16 weeks after implantation in a rat femur. The sample still has a clear boundary, namely the joint of the Mg–Re alloy and femur, approximately 60 μm to the left of the starting point of the line sweep. This indicates that there was still a small gap between the sample and rat femur. Figure 5d shows the sample of the intersection part of the TRC-30 m/min Mg–Re alloy rod and femur 16 weeks after implantation in a rat femur. The results of the EDS linear scan analysis showed that there was no obvious boundary in the sample, indicating that there was no gap between the Mg–Re alloy rod and femur and it was filled with new bone. Moreover, the Mg distribution at the joint of the Mg–Re alloy rod and femur was relatively uniform, indicating that the Mg element in the Mg–Re alloy was partially and uniformly diffused into the femur.
Figure 5e shows the results of the surface EDS linear scan analysis of the sample at the intersection of the TRC-10 m/min Mg–Re alloy rod and femur 32 weeks after implantation in a rat femur. The sample still has a boundary with the joint of the Mg–Re alloy and femur approximately 25 μm to the left of the starting point of the line sweep. This indicates that there was still a small gap between the sample and rat femur. Figure 5f shows the sample of the intersection of the TRC-30 m/min Mg–Re alloy rod and femur 32 weeks after implantation. The results of the EDS scan analysis show that there was no obvious boundary in the sample, and Mg elements were relatively evenly distributed at the junction of the Mg–Re alloy rod and femur. The Mg element in the Mg–Re alloy partially and uniformly diffused into the femur, and the content of Mg element in the junction of the Mg–Re alloy and femur was significantly greater than that in the TRC-30 m/min Mg–Re alloy 16 weeks after implantation.
To evaluate the biocompatibility of the two Mg alloys in vivo, we evaluated the histocompatibility of representative samples of the liver, myocardium, and kidney. As shown in Fig. 6, compared with the control group, there was no significant difference in the size and morphology of cells and nuclei of the TRC-10 m/min group and TRC-30 m/min group. No necrotic tissue was observed. No morphological changes, edema, or degeneration were observed in the endomyometrium and nucleus of myocardium. Clear and intact proximal convoluted tubules were observed in the kidney specimens, indicating no inflammation or tissue damage in either group. Hepatocytes in the TRC-10 m/min group were obviously injured, and with an increase in time in vivo, the larger the area of the vacuoles, the greater damage, while hepatocytes in the TRC-30 m/min group had a normal structure and no signs of damage. According to the implant corrosion analysis, the implants in the TRC-10 m/min group corroded too fast and released too much Mg, which caused hepatocyte injury.
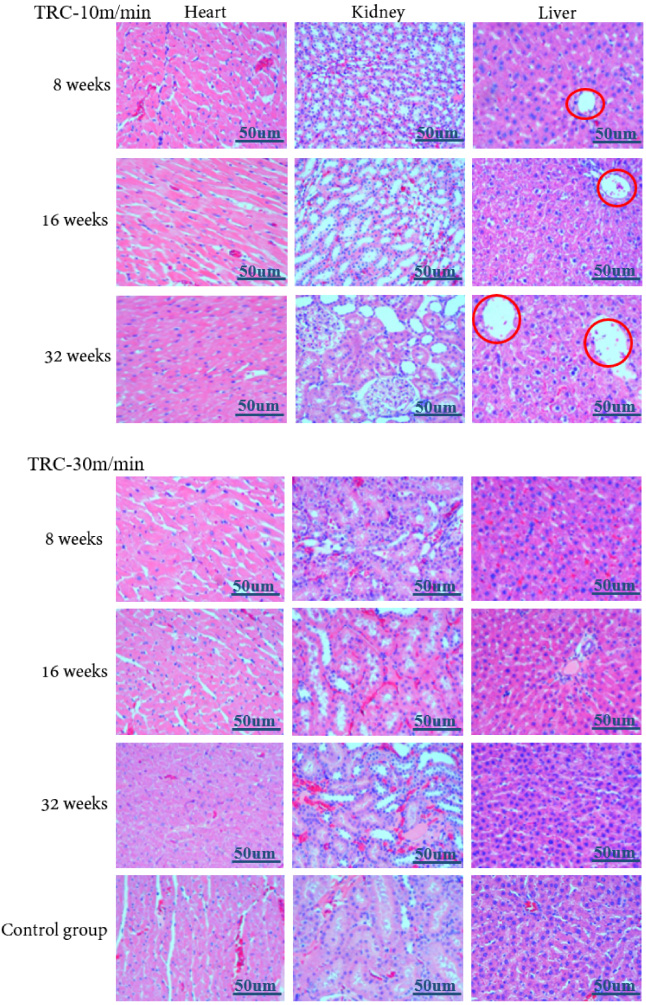
Representative HE staining of liver, myocardium, and kidney tissue 8, 16, and 32 weeks after implantation.
As shown in Fig. 7, during the implantation process, the values of aspartate aminotransferase (AST) and alanine aminotransferase (ALT) in the control group and TRC-30 m/min group were similar. AST and ALT are indicators of early myocardial infarction, hepatocyte necrosis, degeneration, liver cirrhosis, liver cancer, and other diseases, indicating that the liver function of rats in the TRC-30 m/min group did not change significantly because of the alloy, while the amount of AST and ALT in the TRC-10 m/min group was greater than that in the control group over the entire in vivo period. The reason for this change may be that the Mg alloy in the TRC-10 m/min group decomposed too fast 8 and 16 weeks after implantation in the rat femur, leading to an excessive Mg ion concentration in the body, thus causing damage to the liver function that is consistent with the results of the visceral sections of rats in the experimental group.
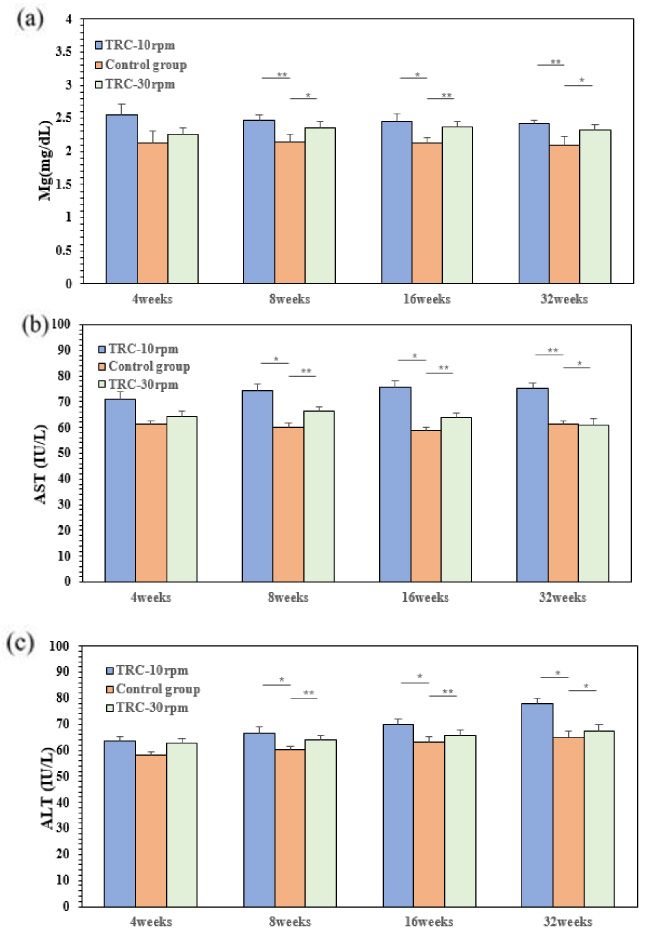
Mg2+ concentration and main liver function indexes of experimental animals at 4, 8, 16 and 32 weeks after operation (∗ P < 0.05, ∗∗ P < 0.01).
The results of microscopic observations and serum tests of visceral specimens indicate that the slowly corroding magnesium alloy does not cause abnormal circulation and visceral lesions in rats. Moreover, the magnesium alloy is as non-toxic as titanium alloys of the same medical instrument standard.
The microstructure, corrosion behavior, and bone reaction in vivo of Mg–Re alloys prepared by the TRC method with four casting speeds, and the effect of long-term fixation on systemic circulation were discussed. The following conclusions were drawn: The microstructures of Mg–Re alloys with casting speeds of 10 m/min, 16 m/min, 24 m/min, and 30 m/min were studied in detail. With an increase in casting speed, the grain size of the cast-rolled pieces was finer, and the corrosion resistance of the alloy increased. Among the four Mg–Re alloys, the corrosion resistance of the Mg–Re alloy with TRC-30 m/min was the best. The results of the animal tests showed that the TRC-30 m/min group produced more bone tissue than the TRC-10 m/min group. The new bone produced by the TRC-30 m/min group fused with the original femur, and the element composition and content of the new bone were similar to the original femur. The staining of the rat heart, liver, and kidney showed that the corrosion reaction of the TRC-30 m/min Mg–Re alloy did not cause an abnormal cell morphology, and damage of the rat liver in the TRC-10 m/min group was more serious at longer timepoints. The serum of rats in the TRC-30 m/min group was similar to that in the control group, while the AST and ALT contents in the TRC-10 m/min group were greater than those in the control group throughout the in vivo period, indicating that the liver might be damaged. Therefore, the long-term implantation of the TRC-30 m/min Mg–Re alloy will not damage the body’s circulation and immune system, and is not harmful to the human body.