
Abstract
BACKGROUND:
Currently, quadrilateral anterior cervical plate (QACP) is a highly prevalent ACP.
OBJECTIVE:
This study aims to design a novel ACP using topology optimization (TOACP).
METHODS:
A completed model for C1–C7 cervical segments was established and validated. QACP and TOACP cage systems were implanted within two cervical vertebrae models, respectively, and peak stresses and stress distributions for screw, plate, endplate and cage displacement were investigated under differing exercise modes.
RESULTS:
Stress levels upon QACP screw were maximized for over-extension exercise (243.3 MPa, 3.35% > TOACP screw). Stress level upon TOACP plate was maximized for over-extension exercise (118.2 MPa, 7.26% > QACP screw). Following QACP cage system implantation, stress on endplate and cage displacement were maximized for extension exercise, which were 27.1%, and 6.3% > TOACP cage system, respectively. Finite element analysis results revealed that topological optimization of the plate can effectively reduce screw stress, thereby enhancing cervical segments’ stability during surgery. Furthermore, stress on endplate and cage displacement decreased, indicating great potential in cage sinking and fusion enhancement.
CONCLUSIONS:
Topological optimization of the plate equips the cage system with advantages in clinical applications and biomechanical performance, providing alternative solutions and a theoretical basis for ACP design.
Keywords
Introduction
The prevalence of desk work among the contemporary workforce has led to an increasing incidence rate of cervical spondylosis. Despite several such cases can be relieved with conservative therapy, a proportion of patients still require surgery to be cured [1]. During cervical spondylosis surgery, the anterior cervical discectomy and fusion (ACDF), which is commonly used in clinical practice, is regarded as a golden rule for the treatment of cervical diseases [2]. Currently, in order to improve the fusion rate, most of the anterior cervical surgeries are designed with an additional anterior cervical plate (ACP) system, and the most prevalent ACP system is the quadrilateral anterior cervical plate (QACP). This design is widely used with good clinical results [3].
Conventional ACP system improved stability of the cage system, though several challenges still exist, including screw loosening and fracture, steel plate fixation failure, cage sinking and cage stress shielding [4,5]. Presently, multiple research efforts are underway to evaluate and design ACP systems to reduce the potential risk of these complications. Hakan et al. [6] designed an articulated, collapsible quadrilateral steel plate to evaluate the impact of novel pre-bending plate on patients, from a biomechanics perspective. Peterson et al. [7] analyzed the impact of differing stiffness in ACP systems upon stress distribution, using quadrilateral plates with differing stiffness. Mackiewicz et al. [8] investigated the differences in stability and mechanical properties of trapezoidal, quadrilateral and semi-constrained plates in single-segment ACDF, post-operatively.
This study aims to design a novel ACP using topology optimization (TOACP), by building finite element models with two differing ACP systems in ACDF, to analyze and evaluate peak stress and stress distribution, as well as cage displacement of the two fixation systems under differing post-operative exercise modes (forward flexion, lateral flexion, rotation, and back extension).
Materials and methods
Finite element modeling of cervical vertebrae
A 24-year-old volunteer (height = 181 cm, weight = 67 kg) was enrolled in this study. X-ray examination revealed no history of neck trauma or cervical spondylosis. The study was approved by the Ethics Committee of the School of Mechanical Engineering, Xinjiang University, and participants signed the relevant informed consent forms.
The CT scan was performed on the cervical vertebrae, where the scan layer spacing and layer thickness were both set to 1 mm. The scanned data were stored in DICOM format and imported into Mimics Research v17.0 (Materialise Inc., Leuven, Belgium). Subsequently, the cervical spine was reconstructed in 3D format and exported as a stl file after exporting as a 3D model. Within Geomagic Studio 2012® (Geomagic Inc., Morrisville, NC, USA), the solid model was constructed by processing the stl file and subsequently exporting into an IGES file. Within Hypermesh® 14.0 (Altair Engineering, Inc., Troy, MI, USA), the IGES file was imported and the completed cervical spine solid model was meshed. Within finite element analysis, the body of cervical vertebrae could be divided into cortical bone, cancellous bone, endplate, and rear structure. Cortical bone was simulated using a triangular shell unit with a thickness of 1 mm; cancellous bone was simulated as a mixture of tetrahedral and pentahedral units; the endplate was simulated using a rectangular unit. The annulus fibrosus matrix, the nucleus pulposus, and the articular cartilage were simulated using an eight-node hexahedral unit, with a non-linear surface contact between the cartilages, with a friction coefficient of 0.05. The human ligament, which is only subject to tension, was simulated using a 1D rod truss unit. The ligaments included anterior longitudinal ligament, posterior longitudinal ligament, ligamentum flavum, interspinous ligament, joint capsule ligament, posterior capsule ligament, and the position of each ligament was determined anatomically [9–11].
Topological optimization of ACP
Topological optimization technology is a design method to optimize the material distribution in a given area to remove redundant material, which can optimize material distribution of the implant, reduce implant elastic modulus and reduce stress shielding [12]. While finite element analysis can simulate real force conditions, these can be combined with topological optimization technology, in order to apply real loads and constraints - based upon biomechanical features of implant materials [13].
Within this study, common ACP tissue (see Fig. 1a) was simplified in SolidWork®2013 (SolidWorks Corp., Waltham, MA, USA) and exported into ABAQUS® 14.0 (Simulia Inc., Providence, RI, USA) as IGES format to select material type, meshed, and topological optimized. To ensure best biocompatibility in plates, the optimization objective was set as the volume fraction <50%, strain energy was minimized, boundary contour of the plate was frozen, and load applied to the plate was perpendicular to the plate. The target number of iterations was set to 20 [14]. The result was imported into SolidWork®2013 in stl format for further simplification, which is illustrated in Fig. 1.
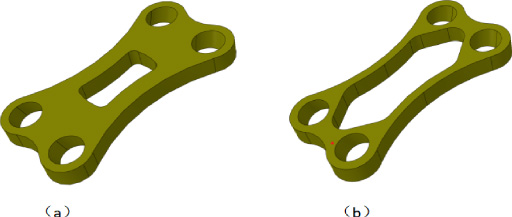
Schematic diagram of the two ACPs (a) ACP prior to topological optimization; (b) ACP post-topological optimization.
Due to high morbidity in segments C5–C6 within cervical vertebrae, this study simulated implanting segments C5–C6 in-cage [15]. The intervertebral cage was designed and constructed using polyetheretherketone (PEEK), and appropriately trimmed for insertion into the C5–C6 intervertebral space. The cage was placed at a distance of 1.5 mm and 3 mm from the anterior and posterior edges of the vertebral body, respectively, to prevent the cage slip from protruding into the spinal cord, and the bone graft was a hollow portion of the cage, to be filled with surgically-removed cancellous bone or other autologous bones of the patient [16,17]. Figure 2a shows the geometry and placement condition of the bone graft-cage.
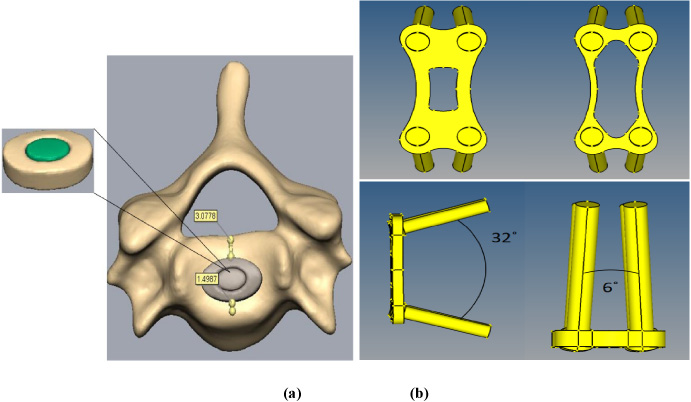
Cage system parameters: (a) cage-grafts geometrical pattern and spatial location; (b) 3D geometry structures of two ACP systems.
The plate height should be spaced by 5 mm from adjacent disc, to avoid bone impingement with the anterior edge of the adjacent vertebral body. The screw into the bone in single-segment ACDF operation was 32 degrees outwards in the sagittal plane, and 6 degrees inwards in the cross-sectional plane, to maintain enhanced stability of the cage system [18], which is 14 mm in length and 3.5 mm in diameter (Fig. 2b). During simulation, all screws were simplified, with no threads. The material of plate and screw for both internal fixation systems was medical titanium alloy.
Figure 3 shows the established models. Complete cervical vertebrae model, cervical vertebrae model of implanted QACP and TOACP cage system were imported into ABAQUS® 14.0, and unit type and material properties were defined. The composing material attributes and units were selected based upon previous studies [9–11], as shown in Table 1.
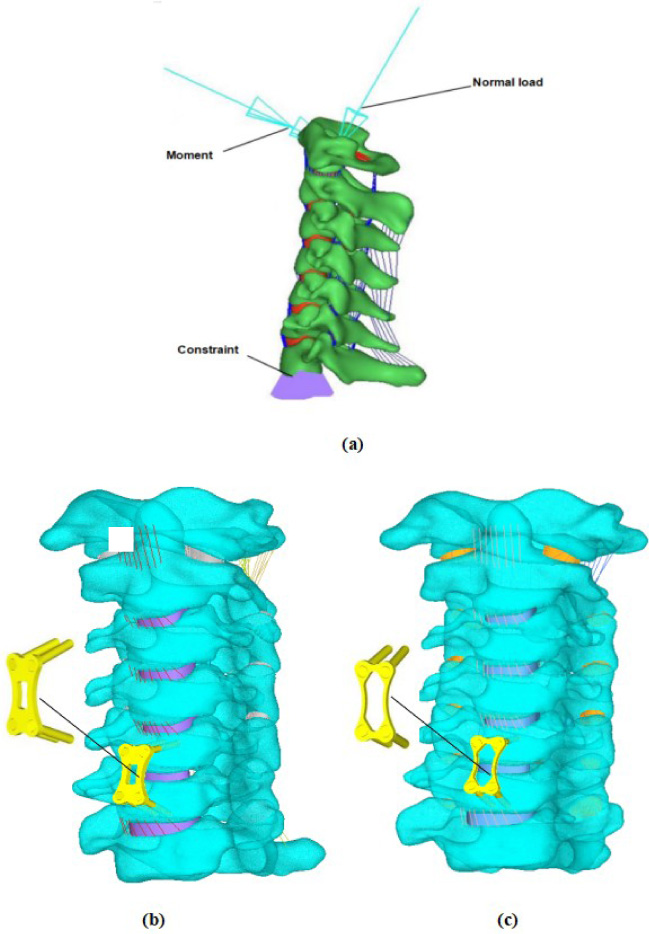
(a) Complete cervical vertebrae model; (b) cervical vertebrae model with implanted QACP cage system; (c) cervical vertebrae model with implanted TOACP cage system.
Unit selection and material parameters of each part of the cervical spine model
To avoid stress concentration caused from artificially applied loads, the center of mass of vertebral body C1 was extracted and coupled to C1. The weight of human head is typically 7% of body weight, and the weight of the volunteer was 67 kg, thus assuming – for this investigation - a concentrated force of 46.9 N was applied at the center of mass with a vertical downward load direction. The range of motion (ROM) of the cervical spine was reduced by 46% ∼ 89.5% in patients following single-segment ACDF [19]. To simulate normal postoperative locomotion, a 0.3 N⋅m moment was used as the load, to simulate normal post-operative motion [20], while a 1.0 N⋅m pre-operative moment was used as the load for excessive exercise. During finite element analysis calculations, the lower surface of the C7 vertebral body was fully constrained for all three abovementioned finite element models. Additionally, the proposed model was validated by analyzing ROM of differing cervical segments under differing exercise modes, in the completed finite element model.
Results
Model validation
Finite element analysis using the completed cervical vertebrae model was conducted, and results were compared with those of human post-mortem cervical vertebrae studies [22], together with ROM investigations of differing cervical vertebrae model segments, involving the skull under differing working conditions and exercise modes [23]. Depicted in Fig. 4, the proposed model shared similar motion responses with previous referenced experiments, despite several simultaneous variations. Based on comparative analyses between references and this study, possible reasons could be varying parameter configurations in differing finite element analyses and following variations in results/variations in individual cervical vertebrae outlines. In light of these differences, the cervical finite element model was in good agreement with the overall cervical motion trend for ROM obtained from the previous solid experiments and simulations. Therefore, the finite element model used in this study was successfully validated.
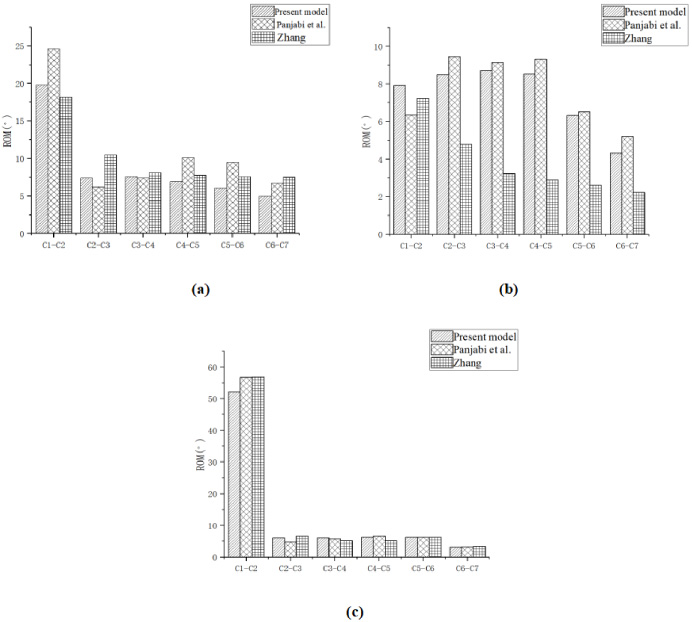
Comparison of each segment ROM of C1–C7. (a) ROM in Flexion and extension; (b) ROM in Lateral bending; (c) ROM in Axial rotation.
According to stress clouds depicted in Fig. 5, in both QACP and TOACP, stress on screw intensified at the root of the device, which was also the outer edge between the screw and cancellous bone contacting surface, indicating the site where screw could easily slip off and fracture. Meanwhile, the stress level in the observation window (middle hole) of the TOACP varied slightly from that of QACP plate, reducing the risk of fatigue failure.
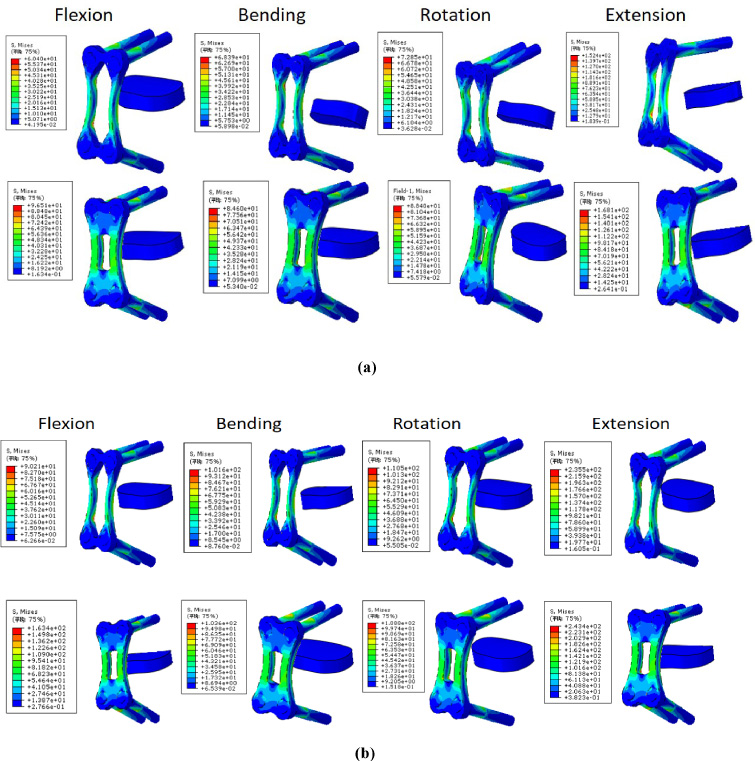
Von Mises equivalent stresses in the QACP and TOACP systems cloud under differing exercise modes. (a) normal exercise after surgery; (b) excessive exercise after surgery.
Depicted in Fig. 6a and b, maximum stresses on both screw and plate increased for cases of excessive exercise post-surgery. Herein, stress upon QACP screw was maximized in the case of over extension exercise (243.3 MPa, which was 3.35% > TOACP screw). Stress upon the TOACP plate was maximized for over extension exercise (118.2 MPa, which was 7.26% > QACP screw). Additionally, maximum stress on QACP screw was higher than that of TOACP under most working conditions, while maximum stress on TOACP plate was higher than that upon QACP plate under conditions of lateral flexion, rotation, and back extension.
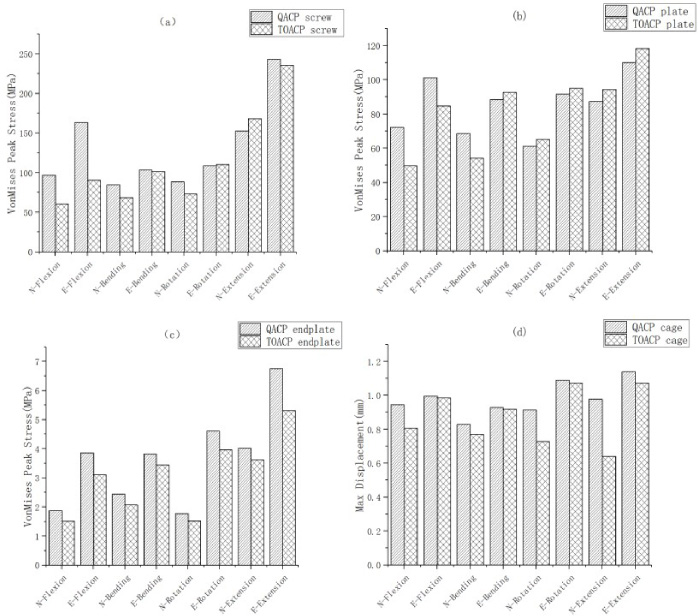
Peak stresses and maximum cage displacements of screw, plate and endplate of the two ACPs under differing cervical exercise modes. N = post-operative normal exercise; E = post-operative excessive exercise. (a) Maximum screw stress for both ACPs; (b) maximum plate stress for both ACPs; (c) maximum endplate stress for both ACPs; (d) maximum cage displacement for both ACPs.
The tensile strength of titanium alloy for medical use at ASTM or ISO for Grade 1 is ≧240 MPa, except for the screw of QACP which has a stress of 243.3 MPa at over extension exercise. All other working conditions are within the safe range, so over-extension exercise must be avoided. In this perspective, the topologically optimized ACP improves the safety of the cage system in terms of tensile strength.
Depicted in Fig. 6c, and compared to normal post-operative exercise, endplate stress under the condition of excessive exercise was significantly higher. Meanwhile, endplate stress for the QACP cage system was higher than that of TOACP cage system under all conditions, with stresses on the endplates in both models being maximized during over-extension exercise (6.752 and 5.312 MPa, respectively). In this case, maximum stress on the QACP cage system endplate was higher than for TOACP cage system endplate by up to 27.1%.
Cage displacement
Depicted in Fig. 6d, the maximum cage displacement was increased in the condition of excessive exercises for both cases. The maximum cage displacement for QACP cage system was larger than for TOACP cage system, regardless of the working conditions, and cage displacements of both systems were maximized in the case of over-extension exercise (1.14 and 1.072 mm, respectively). In this case, the maximum cage displacement for QACP cage system was 6.3% higher than that for the TOACP cage system.
Discussion
This study conducted topological optimization on ACP, simulated post-operative normal and excessive exercises, and assessed biomechanical variations following the implantation of two types of ACPs into cervical vertebrae. According to the results analysis, it is known that the topologically optimized ACP has an impact on the biomechanical effects of the device in the postoperative cervical spine.
The stress level upon the screw from two types of ACP both lied within root-area, as found in previous clinical and mechanical analyses [24]. Post-optimization of plate implanting, stress level was present within differing areas under varying exercise modes, bringing reduced risk of fatigue failure by plate. The maximum stress upon QACP screw was higher than for TOACP under most working conditions, rendering TOACP with reduced risk of screw breakage and thus being beneficial to successful fusion surgery. However, after optimization, the narrowing of the plate’s viewing window profile results in greater stress during rotation, lateral flexion, and extension, and patients should minimize such neck motions after surgery with this plate.
It has been demonstrated that the endplate plays a key role in the proper functioning of cervical vertebrae. Indeed, stresses on upper and lower endplates are directly related to cage sinking. Hence, endplate stresses can function as a marker of biomechanical performance post-ACP implanting [20]. This study indicated that the maximum endplate stress post-ACDF, using TOACP, was significantly less than for QACP under almost all working conditions, rendering TOACP effective in preventing cage sinking.
Selected patients experiencing ACDF could have symptoms such as cage slipping and shedding, which signal the failure of fusion surgery [5]. Therefore, the maximum displacement of cage is a reference in comparing biomechanical performance of the two ACPs. Based upon abovementioned results, TOCAP demonstrated less cage slipping than QACP, suggesting that TOACP can bring additional cage stability and effectively avoid cage slipping and shedding.
This study exhibits several limitations. First, the model for cervical vertebrae was based upon computerized tomography (CT) data from one single volunteer, with limited universality. However, the finite element analysis of biomechanics provided a comparison of pattern, instead of comparison analyses on large statistical datasets. Consequently, the proposed cervical vertebrae model did not include the effect of muscle in this structure, which could exert a degree of effect on finite element results. Additionally, despite validation of the completed model, these two ACP models were not validated post-implementation, due to limitations of conditions. The finite element and in vitro test did not directly and precisely represent results post-implementation. Meanwhile, the method of screwing (angle and depth of implantation) and the level of surgical skill could also affect biomechanical effect for both ACP implantations into cervical vertebrae. Despite such limitations, this study integrated finite element analysis [21], combined with in vitro analyses [22] and, considering the challenge of post-operative patients wearing neck brace, to build the model based upon CT data where the volunteer was in supine position (see Fig. 3a). This work validated the model and proved feasibility of the proposed model, representing its clinical value.
Conclusions
Topological optimization of the ACP showed its biomechanics effect for each component of the cervical spine and cage system. Firstly, from a materials perspective, the titanium alloy consumed in the plate building was less post-topological optimization, saving costs. Secondly, the observation window of the plate was larger post-topological optimization, which facilitates the surgeon’s operation and observation during surgery. Adopting a biomechanics perspective, the stresses on the screw were reduced to different degrees under various operating conditions in TOACP, and the plate assumed a greater stress distribution, while stresses upon upper and lower endplates and maximum cage displacement were improved. Consequently, TOACP was beneficial to the success of fusion surgery. However, this was an exploratory study and not a formal guide for practical surgical protocols. The purpose of this study was to provide novel ideas and a mechanical/theoretical basis for the design of ACP, so that other investigators can design future studies. Further evaluations and studies are still demanded for future clinical implantation results.
Footnotes
Acknowledgements
PY would like to thank his tutor, Rongchang Fu, whose expertise was invaluable in formulating the research questions and methodology. The insightful feedback pushed him to sharpen his thinking and brought the work to a higher level. PY would also like to thank Zhaoyao Wang for his wonderful collaboration and patient support, as well as his parents for the wise counselling and sympathetic ear, they are always there for him.
Funding
The study was financially supported by the National Natural Science Foundation of China (No. 32260235).