
Abstract
BACKGROUND:
Exercise of the spinal muscles is recommended for a variety of rehabilitative reasons but it is not always clear whether interventions are effective in improving the performance of the muscles or whether their benefit is elicited via other mechanisms.
OBJECTIVE:
To explore the effects of an exercise intervention on the size and exercise performance of the lumbar spine extensor muscles.
METHODS:
Eleven healthy participants undertook a four week programme of exercise. Magnetic resonance imaging and phosphorus spectroscopy were performed before and after the intervention to determine the time to fatigue and phosphocreatine (PCr) depletion during a muscle endurance test (modified Biering-Sørensen) together with muscle cross-sectional area (CSA).
RESULTS:
The post intervention measures were significantly different to the pre-intervention results for the time to fatigue (post-pre: 20.5
CONCLUSIONS:
Exercise improved the performance of the trunk muscles despite no impact on CSA. This demonstrated the importance of obtaining a wide range of measures when assessing the effectiveness of exercise intervention programmes.
Keywords
Introduction
Exercise interventions targeted at the trunk and spine are recommended in the management of a variety of conditions including non-specific low back pain [1, 2], vertebral fracture [3, 4], and after surgery for spinal stenosis [5]. There is also some evidence that they are effective in reducing pain and improving function in patients with degenerative spondylolisthesis [6, 7] and in preventing falls in the elderly [8].
The aim of such interventions is to increase the stability of the spine and upper body by increasing the strength, endurance and neuromuscular control of the spinal muscles [9]. In the lumbar region of the spine, the extensor muscles (erector spinae and multifidus) in particular are considered to play an important role in controlling movement of the trunk and ensuring spinal stability [10, 11], with the psoas and quadratus lumborum acting primarily as flexors and lateral flexors [10].
Exercises from the intervention programme. (a) Cat, (b) Camel, (c) Superman, (d) Side plank, (e) Bridge, (f) Abdominal curl.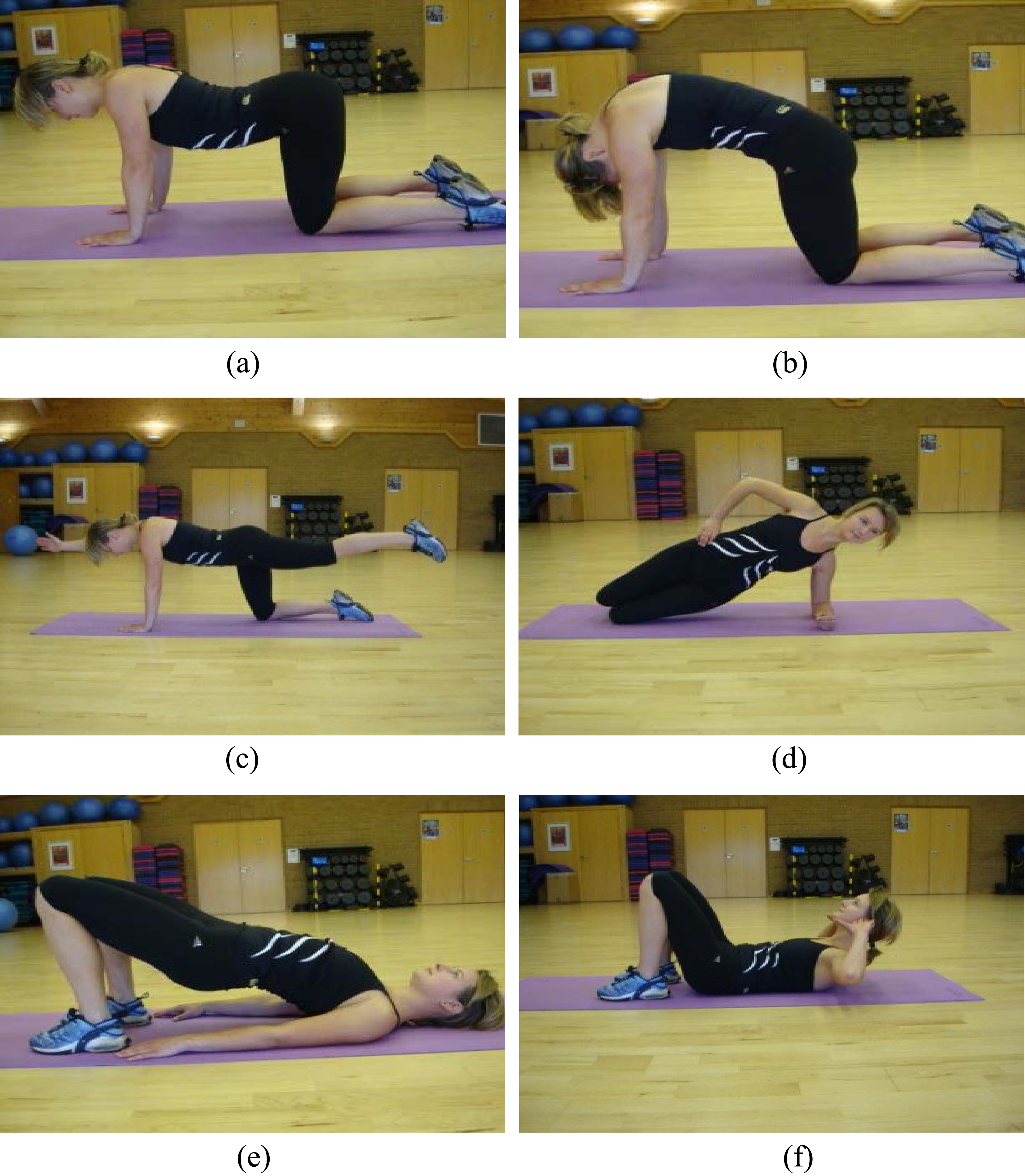
Despite the body of evidence promoting the use of exercise to strengthen the back and spine, there is little consensus over the best type of exercise or the intensity, direction and frequency at which it should be performed [12]. There are also questions as to whether exercise should be tailored to address the specific needs of individual patients or groups of patients [13, 14] and debate, particularly in the literature pertaining to non-specific low back pain, as to whether exercise has an identifiable effect on the spinal muscles or whether improvements in pain and function are mediated by other mechanisms [7, 12, 15].
Measurements of muscle performance, including strength and endurance, are often used to assess the function of the spine [16] and the efficacy of exercise programs [17]. Measures of strength and endurance are generally reliable [16, 18]; however, their appropriateness for assessing patients has been questioned due to their inability to clearly differentiate physical function from pain related behaviour [19] and psychological disturbance [20]. More direct evaluation of whether exercise interventions are affecting muscles is possible using a variety of complementary techniques [21] including electromyography (EMG) to assess muscle activity [22, 23, 24, 25] and imaging to assess muscle size [26, 27] and function [28].
Phosphorous magnetic resonance spectroscopy (31P-MRS) is a further technique that may be used to measure the temporal variation in metabolites such as adenosine triphospate (ATP), phosocreatine (PCr) and inorganic phosphate, as well as monitor pH, thereby providing insight into muscle metabolism [29, 30]. PCr is stored in muscle cells and is used during exercise to maintain levels of ATP during periods when energy demand is not being met by processes such as oxidative metabolism (when muscles obtain and use oxygen to generate ATP) and is thus a useful indicator of muscle oxidative capacity.
There are a limited number of studies that have investigated back muscle function with 31P-MRS [24, 31] and, although it has been shown that PCr depletion can be measured reliably in the spinal extensor muscles [31], it is not known whether a short term exercise intervention produces measureable changes in PCr depletion in these muscles. The aim of this study was therefore to perform a small scale study to assess whether changes in PCr depletion and cross-sectional area of the lumbar extensor muscles were detectable after a four week exercise intervention.
Participants
Eleven participants gave consent to take part in this study, which was approved by the University of Exeter Sport and Health Sciences ethics committee. Exclusion criteria were: a history of LBP, current participation in any exercise programme targeting the lumbar region, and having a medical history that would limit the ability to undertake exercise. Six of the participants were female (age 33
Illustration of the set-up of the modified Biering-Sørensen muscle endurance test within the MRI scanner. (a) Participant supported by foam wedge, (b) Foam wedge removed.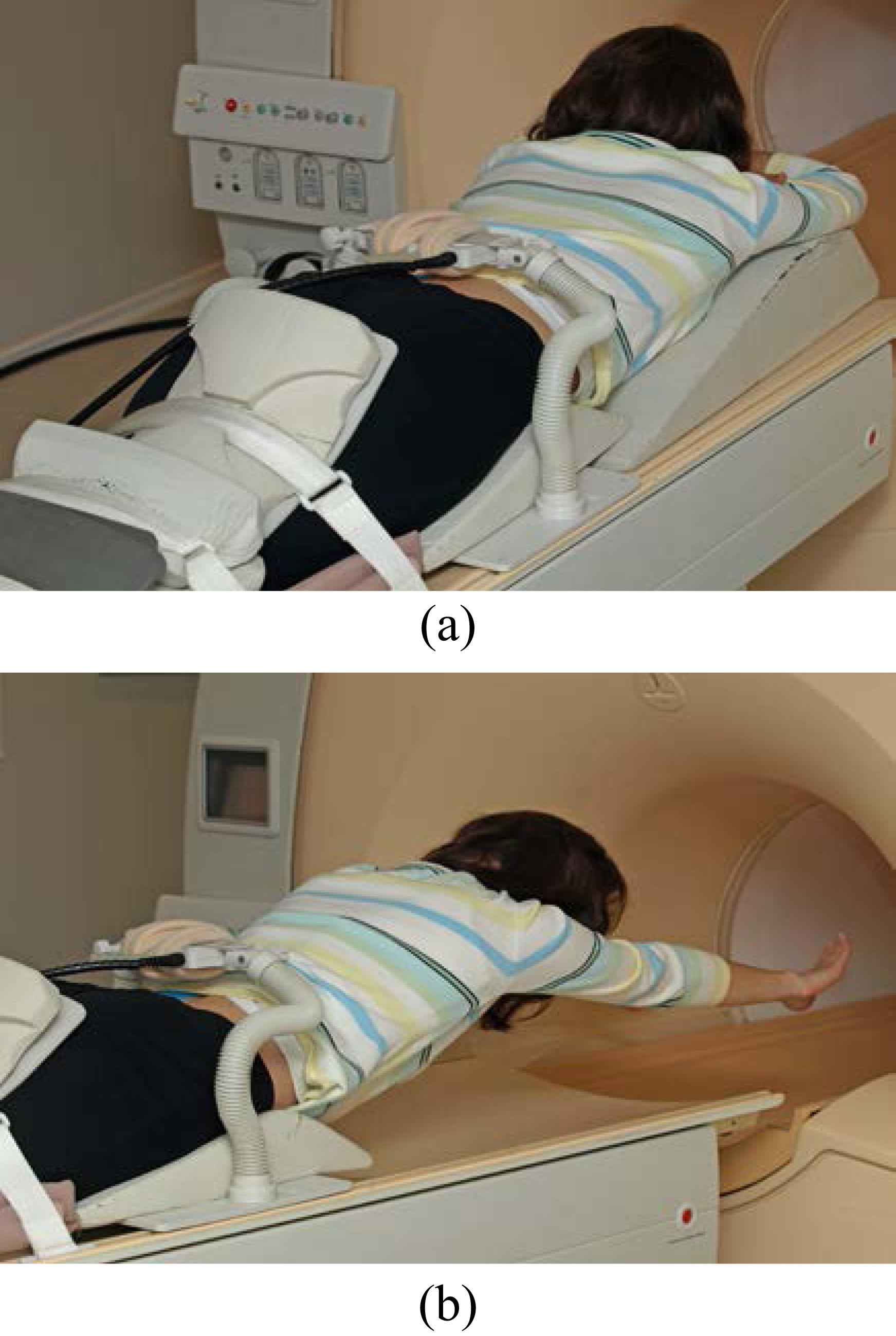
The exercise intervention consisted of cat (Fig. 1(a)) and camel (Fig. 1(b)) exercises as a warm up, followed by the main exercise routine consisting of superman (Fig. 1(c)), side plank (Fig. 1(d)), bridge (Fig. 1(e)) and abdominal curl (Fig. 1(f)) exercises as described by McGill [32]. All the exercises were undertaken in conjunction with abdominal bracing and hollowing techniques to ensure activation of both superficial and deep spinal muscles [33]. Initially, one to one instruction was provided by one of the authors (VJ), a physiotherapist, to ensure participants were competent at all exercises. Subsequently, participants undertook training without supervision five times a week. Eight repetitions of two sets were undertaken for the first two weeks, progressing to ten repetitions of two sets for the following two weeks. A diary was used to monitor adherence to the exercise routine.
Testing protocol
The testing was undertaken at the University of Exeter MR Research Centre using a protocol previously described [31]. Participants were required to attend on two occasions; once before the exercise intervention and once after the exercise intervention had been completed.
Participants were palpated to determine the location of the L4 spinous process and a cod liver oil capsule, visible in MR images, was placed 1 cm cephalically on the right side of the processes corresponding to be the approximate location of the L3/L4 disc. The participants were then positioned in a supine position within the bore of a 1.5 T superconducting magnet (Intera, Philips, The Netherlands) resting on a 5-element spine coil.
T1-weighted MR images were then acquired in the axial and sagittal places to provide spine and muscle anatomical information (turbo spin echo sequence, 1
Participants were subsequently repositioned in a prone position, head first. A small foam wedge was placed directly under the pelvis with an additional larger wedged positioned under the head and upper body (see Fig. 2(a)). Thighs and calves were fastened by straps to secure the lower body. A 6 cm 31P coil, fitted in a custom made holder, was positioned vertically above the location of the L3/L4 disc and the participant moved into the scanner such that the L3/L4 disc was located at the isocentre. Matching and tuning of the coil and an automatic shimming protocol was then performed within a volume that defined the spinal muscle to optimise the signal from the muscle under investigation.
The foam wedge supporting the upper body and head was removed and the participants were instructed to maintain their body position until fatigue at which point the exercise duration was recorded. For 60 s prior to the beginning of exercise and continuously during exercise, 31P data were acquired every 1.5 sec with phase cycling with four phase cycles, resulting to a spectrum being obtained every 6 seconds.
MRI data analysis
The axial slice closest to the L3/L4 disc level was identified from each data set and saved in DICOM format. Images from the two visits were visually compared for each participant to ensure the slices obtained at different visits matched as well as possible. The slices were viewed in ImageJ (open source software), magnified to 300% and contrast enhanced (via histogram equalization and normalization) and the cross-sectional area of the multifidus (MF), erector spinae (ES), quadratus lumborum (QL) and, psoas (PS) were determined. Fat within a region of interest was not excluded and infiltrations of fat going into a muscle were interpolated across. Fat completely outside the muscle was excluded. Measurements were determined by one of the authors, blinded to participant and visit information and with the order of the images randomized. Areas were determined for both left and right muscles separately and the sum calculated. Previous work employing the same methodology examining repeated measurements of spinal muscle CSA found the reliability of this method (within-subject standard deviation) to be 0.8 cm
31P-MRS data analysis
The acquired 31P spectra were quantified via peak fitting, assuming prior knowledge, using the jMRUI (version 3) software package employing the AMARES fitting algorithm [34]. Spectra were fitted assuming the presence of the following peaks: Pi, phosphodiester, PCr,
PCr percentage depletion,
After fitting, values of
All statistical analysis was carried out in PASW statistics 18 (SPSS Inc., Chicago, USA). Paired samples t-tests were used to compare cross-section area, time to fatigue and PCr depletion before and after the four week intervention, with statistical significance defined as
Time to fatigue, PCr depletion, and cross-sectional area (CSA) of the spinal muscles
Time to fatigue, PCr depletion, and cross-sectional area (CSA) of the spinal muscles
MF
Time to fatigue for each individual participant for the two visits when undertaking the modified Biering-Sørensen test.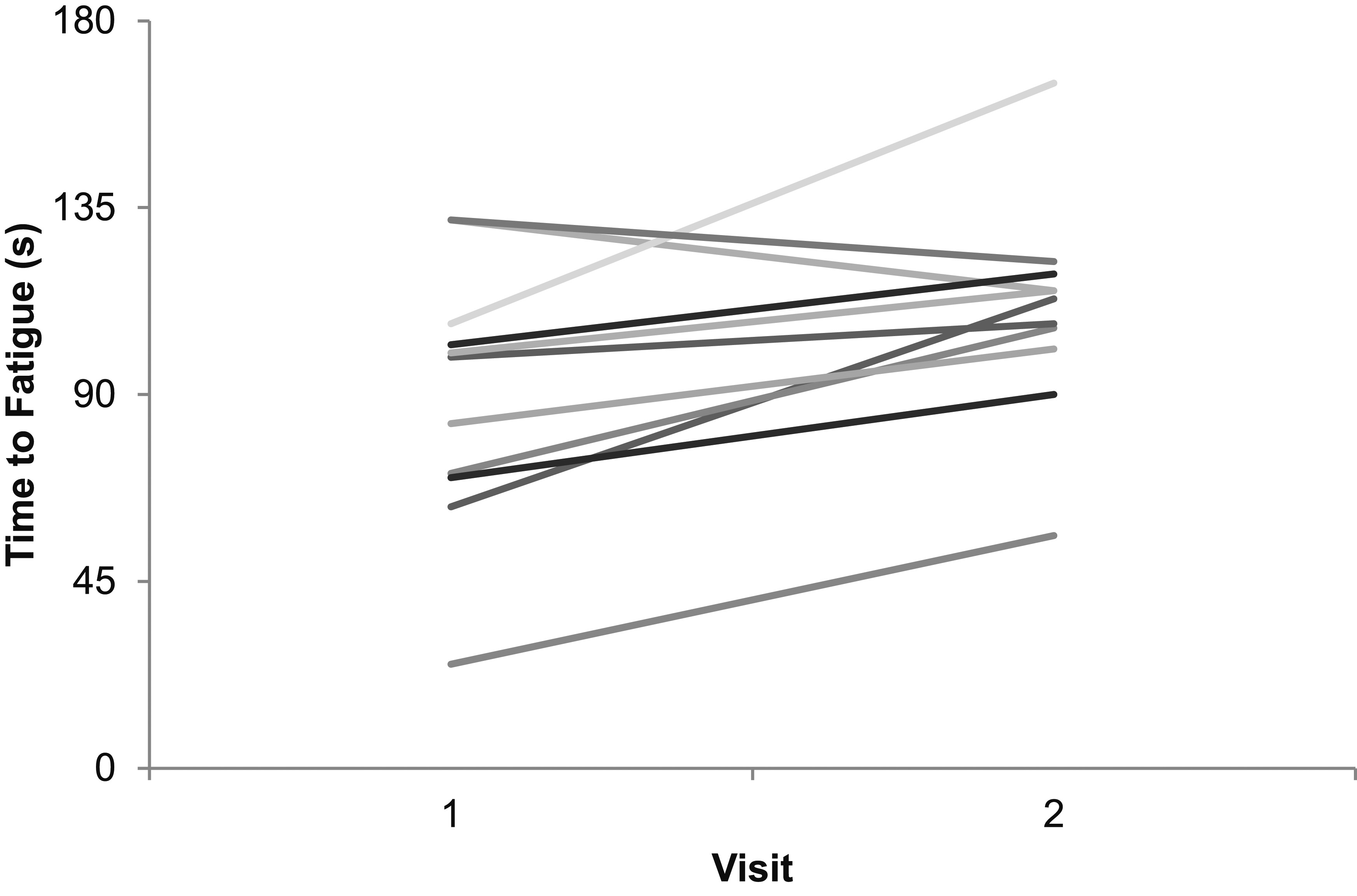
Representative PCr response during the modified Biering-Sørensen test, before and after four weeks intervention together with the fitted with a single exponential of the form given in Eq. (1). Note that exercise was begun after an initial 60 s baseline data collection period.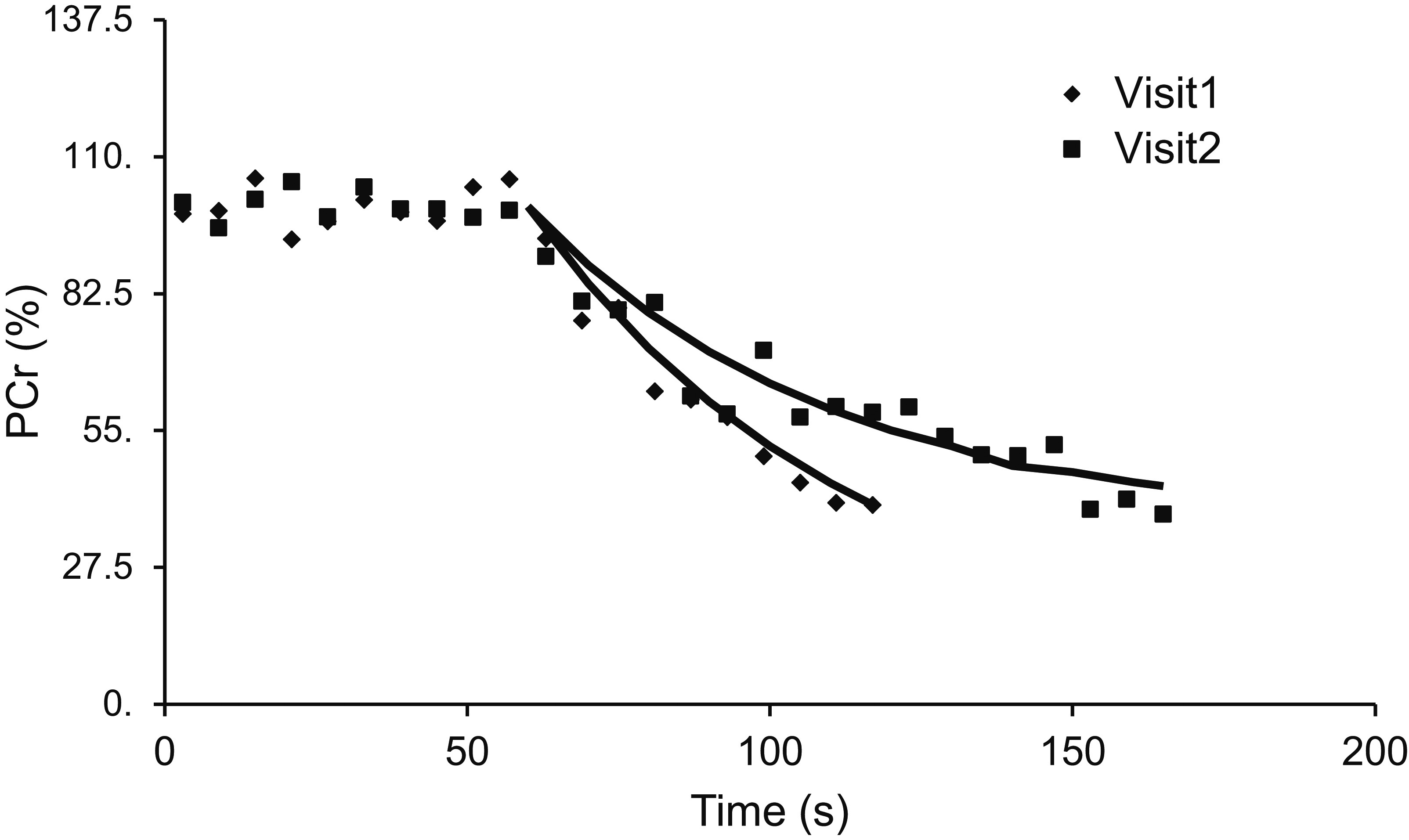
All participants completed the training protocol, with 100% self-reported adherence. The time to fatigue during the endurance test was increased following the exercise intervention (Table 1); individual responses are illustrated in Fig. 3, showing an improvement in nine of the eleven (82%) participants. No significant differences were determined for the cross-sectional area of the four spinal muscles as a result of the exercise intervention (Table 1).
For the exercise induced decrease in PCr levels, fitting a single exponential resulted in good fitting of PCr data with no significant residual arising indicative of slow components (a representative response is shown in Fig. 4). PCr depletion after the training intervention was lower than before training; this difference was significant when comparing pre and post exercise training depletion calculated at the time equal to fatigue occurrence for the pre-intervention test and when comparing the depletion calculated at the time to fatigue recorded for each individual test.
Discussion
The aim of this study was to determine whether changes in muscle size and muscle function could be observed in the spinal muscles as a result of a short term exercise intervention. The main findings of the current study were that, after four weeks of exercise, the time to fatigue when performing a muscle endurance test was significantly increased and the depletion of PCr during the test was significantly reduced. No significant changes in cross-sectional area of the multifidus, erector spinae, quadratus lumborum, or psoas muscles were observed.
The ability of the spinal muscles to sustain contraction is important for maintaining normal posture and balance [36]. Endurance of the spinal muscles can be measured using a variety of different tests such as the Biering-Sørensen test [37], a modifed Biering-Sørensen test (Ito test [38]), or the Timed loaded standing test [39]. Back muscle endurance tests generally have high reliability [16, 18, 39] and in our previous work using an identical experimental set-up to the current study we found that reliability over a period of several weeks was excellent [31]. Endurance has been shown to be lower in patients with low back pain in many studies [16, 18] and is considered to be a risk factor for low back pain [37]. Training that includes exercise for the trunk has also been found to increase endurance in various patient groups [27, 36, 40], similar to the results of the current study.
Questions have been raised, however, over the validity of muscle endurance tests as participants can use different strategies when performing them [41] and performance is also modified by variety of psychological factors [42]. Thus, measures of muscle function that help assess whether improvements are due to physiological changes or not are desirable. Some of these, such as EMG, have been used extensively and provide useful information about muscle activity, indicative of fatigue, although there have been questions concerning them in assessing the effects of training [43]. Muscle size is another useful measure that is related to muscle strength and an increase in muscle size is expected with training [44]. Spinal muscle atrophy has been associated with diseases such as low back pain [45, 46, 47, 48]but few studies have investigated whether muscle size is increased as a result of exercise training. Of those that have investigated this, the findings are equivocal between exercise regimes [26] and between studies [26, 27, 49]. A possible reason for the lack of increase in muscle cross-sectional areas is that the training regime was insufficient in length or intensity to produce significant muscle hypertrophy [26]. It may also be that the participants, similar to those in the study by Teyhen et al. [27] were already physically active in comparison to those in the study by Hides et al. [49] where the participant’s muscles had atrophied due to bed rest. An alternative reason is that the changes in muscle size were less than the measurement error; using data from our previous study [31] we estimate the measurement error to be around 10% of the muscle size.
In the current study, the depletion of PCr following sustained contraction was reduced after the four weeks of training. There was a reduction at the end-point of fatigue (even though the fatigue time was longer) and there was also a reduction at a matched time-point corresponding to the time to fatigue recorded for the pre-intervention test. Studies in the leg muscles have shown that depletion of PCr is lower in endurance trained individuals compared to sedentary individuals [50] and is thought to arise from greater oxidative capacity as a result of training. As the rate of PCr depletion effectively reflects the shortfall between energy (ATP) demands and energy supply from processes such as oxidative metabolism, any training induced reductions in PCr depletion are indicative of improvements in the ability to maintain muscle contraction.
There are various possible mechanisms underlying a reduction in PCr depletion. These include increase in muscle size, increase in capillary density, increase in mitochondrial density [51, 52], and changes in the predominant fibre type from type II to type I (a fibre type more resistant to fatigue) [50, 53]. It is not clear as to which mechanism may have occurred in the current study, however, the timescale expected for changes in fibre type [54] make this unlikely to have occurred in four weeks. Furthermore, the non-localized 31P-MRS method used in the current study means that the PCr signal was sampled for all muscles within the sensitive region of the coil (of extent approximately 6 cm from the coil centre) such that it is not possible to establish where changes may have occurred. Localized 31P-MRS methods are available [24], however, meaning that this limitation could be overcome in future studies.
It should be stated that the study features a relatively small sample size and one with a limited age range of participants. Thus, the results found may not be universally applicable to the population as a whole. In addition, given no control group was included it is possible that improvement in exercise performance could result from learning effects, such that the participant modifies the way they undertake the exercise in order to minimize fatigue in subsequent trials. However, a previous study using the same protocol and with a similar interval between trial repetitions has indicated no significant time effects to indicate learning [31] and resulted in excellent reliability for endurance time and PCr depletion (single-measures intra-class correlation coefficient 0.86 for endurance time and 0.73 for PCr depletion) [31].
Conclusion
Changes in endurance time and PCr depletion in the spinal muscles can be detected after a four-week exercise training intervention despite no changes in cross-sectional area. The use of 31P-MRS as an additional method for assessing baseline muscle function and changes induced by training may be useful for determining whether exercise is having an effect on targeted muscles and for helping to establish whether there are particular groups of patients for who exercise is most suitable for or for tailoring exercise specifically to their needs.
Conflict of interest
The authors have no conflict of interest to report.
Footnotes
Acknowledgments
We thank the participants who volunteered to take part in our study and also thank the NIHR Clinical Research Facility, University of Exeter for funding J Fulford’s salary.