
Abstract
BACKGROUND:
Dynamic tasks over unstable surfaces are commonly done in daily activities.
OBJECTIVE:
A number of studies indicated positive effect of doing postural tasks over unstable surface on trunk muscle activities in patients with low back pain (LBP), while the others reported opposite effects. Due to lack of consensus in the findings in this area of research, we aimed to systematically review studies, which investigated the effect of surface instability on trunk muscle activity in patients with LBP as compared to healthy individuals.
METHIDS:
A literature search was performed using the PubMed, Science Direct, OVID, CINAHL, PEDro, Cochrane, Scopus and MEDLINE databases. Low back pain, unstable surface, posture or stability and trunk muscle activity were applied as keywords. The methodological quality was examined using valid assessment tools.
RESULTS:
The activity of superficial trunk muscles is impaired in patients with LBP during dynamic tasks over unstable surfaces. Differences in the methodology of included studies could be considered as reasons behind the inconsistencies in the findings in included studies. These studies included investigation of superficial or deep muscles, the timing of recorded muscle activity, the level of surface instability and the length of time over unstable surfaces.
CONCLUSION:
Dynamic tasks over unstable surfaces could decrease pre-program reaction (PPR) and increase voluntary reaction (VR) of superficial trunk muscles in patients with LBP, which may reduce the ratio of deep versus superficial muscles, compared to healthy individuals.
Introduction
Low back pain (LBP) is one of the most common musculoskeletal complaints and costly health problems in both western and eastern societies [1, 2]. About 70–80% of adults, in the general population, experience LBP at least once in their lifetime [3]. High prevalence of this problem may be caused by a large number of factors that may lead to LBP or an inadequacy of available assessment or treatment techniques [4, 5]. LBP is a compound and multi-factorial bio-psychosocial disorder with unclear definitive anatomical causes [2, 6]. Thus, any improvement in the assessment of LBP symptoms may lead to the development of novel treatment strategies to improve the functional outcomes in the patients with LBP.
New management approaches such as functional therapy have placed emphasis on performing the adaptive strategies of movement in the final stage of management to treat LBP [7]. The literature indicates that this approach is more effective than exercise therapy alone in the reduction of disability and enhancement of functional capacity [7, 8]. Dynamic postural control, required during unstable standing condition, is a common conditioning approach in daily activities such as walking, running and climbing stairs. Patients with LBP may experience pain when they are subjected to these unstable conditions during daily activities [9]. Therefore, according to the functional therapy approach, one of the final goals of rehabilitation in patients with LBP, after motor control training and correction of maladaptive strategies, is controlling their dynamic posture and pain during daily standing activities in order to progressively increase their functional capacity [7].
Inclusion and exclusion criteria for identified studies
Inclusion and exclusion criteria for identified studies
Instead of using unstable surface, articles used unstable position such as one leg standing for assessing of activation pattern.
The literature indicates that doing dynamic tasks such as an activity on an unstable surface, may improve the whole body’s balance, dynamic postural control, lumbar joint position sense, deep muscle activity, and lumbar movement [10, 11]. According to the literature, unstable surfaces may produce a therapeutic effect in the patients with LBP during rehabilitation programs with increasing the ratio of deep versus superficial muscles activity [12, 13, 14, 15, 16]. Some investigators have advocated using unstable surfaces to activate the deep trunk muscle [12, 13, 14, 15, 16] and even the global abdominal muscles such as rectus abdominis (RA) [12]. On the other hand, the findings of some studies have shown that the ratio of trunk deep versus superficial muscles activity deteriorate with decreasing deep muscles activity during trunk internal and external perturbation in patients with LBP as compared to healthy participants [17, 18, 19, 20, 21, 22, 23, 24]. The literature indicates that any increase in the activation of superficial trunk muscles during perturbation on an unstable surface causes the enhancement of trunk stiffness and spinal stability in patients with LBP as compared to healthy participants [25, 26], while other studies reported opposite effects [27, 28, 29]. Boudreau et al. and Newcomer et al. indicated decreasing superficial trunk muscles activation during perturbation on unstable surfaces in patients with LBP as compared to healthy participants [27, 28]. In line with the findings in these studies, Rasouli et al. also reported decrease in the deep abdominal muscle activity during perturbation on unstable surfaces in patients with LBP as compared to healthy participants [29]. In contrast, some other studies have indicated progressive improvement in the deep trunk muscle activity in patients who have been trained on an unstable surface [29]. Therefore, there is controversy on the effects of surface instability on superficial and deep trunk muscle activity in LBP patients. According to the controversy, comparison of the effects of standing on unstable surfaces on recruitment of superficial and deep muscles in LBP patients compared to healthy individuals could provide valuable clinical information. Thus, the primary aim in the current systematic review is to determine the effects of standing on unstable surfaces on activity of superficial and deep trunk muscles pattern in patients with LBP as compared to healthy individuals. The secondary aim is to investigate if training approaches using unstable surfaces can induce functional therapeutic effects in patients with LBP. The variables investigated in this review are the type of LBP (i.e. stage, intensity and disability), methodological quality, study of superficial or deep muscles, the level of surface instability which includes the degree of perturbations, the type of surface instability (with tilting or sliding movements of movable platform), the timing of recorded muscle activity, i.e. pre-program reaction (PPR) or VR and the length of using unstable surface, i.e. short- or long-term use. We hypothesized that:
Unstable surfaces decrease superficial trunk muscle activity during VR and increase their activity during PPR in patients with LBP as compared to healthy individuals. Unstable surfaces increase deep trunk muscle activity in patients with LBP as compared to healthy individuals. The high instability levels of unstable surfaces increase trunk muscle activity more than low instability levels in LBP patients.
Inclusion and exclusion criteria
Articles were included if they clearly stated their inclusion/exclusion criteria (Table 1).
Quality assessment of the included studies with case-control design
Quality assessment of the included studies with case-control design
Quality assessment of included articles with clinical trial design
Articles were included if they adhered to these points:
They utilized unstable surfaces as an intervention with or without training. They assessed the effect of unstable surfaces as an external perturbation on trunk muscle activity in the patients with specific or nonspecific LBP as compared to healthy participants.
Accordingly, studies were excluded if their assessment included the following:
They only assessed the effect of an unstable surface on trunk muscle activity pattern in healthy participants. They applied external loads for making external perturbation while assessing trunk muscles activation pattern. Instead of using unstable surfaces, they used unstable positions, such as standing on one leg, to assess the activation pattern.
The search strategy was restricted for relevant articles published in English. An electronic literature search was performed using PubMed, Science Direct, OVID, CINAHL, PEDro, Cochrane, Scopus, and MEDLINE databases between the period 1995–2015. For the search, five keywords were used: low back pain, unstable surface, posture, stability, and trunk muscle activity. In addition, all reference lists of included articles as a hand search were also reviewed to discover additional relevant articles unknown through the initial electronic search strategy.
Study selection
After detecting articles through database searching, some of the duplicated articles were removed. Then, two reviewers (F.E and AM.A) independently screened remaining articles based on the inclusion/exclusion criteria of the study. Two reviewers read all the abstracts, and the third reviewer (S.J.) separately read a random sample of the abstracts. If based on the title and abstract, it was not clear whether an article should be included, the whole article was then checked. Also, if the reviewers had conflicting opinions about including a study, resolution was achieved by the third reviewer (S.J.).
Methodological quality
According to the study design, we used the PEDro scale for methodological quality assessment of the included articles with randomized control trial (RCT) design [30, 31]. The Critical Appraisal Skills Program (CASP) scale was used for the methodological quality assessment of the other included articles that weren’t RCTs [32]. Both CASP and PEDro scales included eleven criteria for internal validity; studies were given a point for each criterion met (Tables 2 and 3). The two reviewers independently investigated the quality of the studies. If there wasn’t a consensus in detail of some articles’ quality assessment, the third reviewer (S.J) resolved these disparities to reach an agreement on any differences between all reviewers. The scale cut points are 9–10, excellent; 6–8, good; 4–5, fair, and below 4, poor [33]. The scores for the CASP scale in the included articles ranged from 7 to 9 (Table 2), and for the PEDro scale, they ranged from 5 to 9 (Table 3).
Data extracted from all included studies
Data extracted from all included studies
CLBP: chronic low back pain, EMG: electromyography, ES: erector spine, RA: rectus abdominis, GC: gastrocnemius, TA: tibialis anterior, EO: external oblique, RMS: root mean square, COP: center of pressure, IO: internal oblique, TrA: transverse abdominis, Long: longissimus, Ilioc: iliocostalis, G Med: gluteus medius, BF: biceps femoris: right, L: left, ROM: range of motion, ADIM: abdominal drawing-in maneuver, MF: multifidus.
The primary outcome measures of this study were the activity of deep and superficial trunk muscles in the participants with and without LBP on unstable surfaces. Muscle activity is measured by surface electromyography (EMG) or ultrasound imaging (US) [18, 19, 21, 34]. The EMG detects the electrical activity of muscles, and the US measures the thickness of muscles during the test [19, 21, 34]. In using an US, the thickness change of muscles during contraction compared to rest conditions can indirectly indicate the level of muscle activity at each position [19, 21].
Details of studies according to finding
Details of studies according to finding
VAS: Visual Analog Scale, CLBP: chronic low back pain, ES: erector spine, RA: rectus abdominis, NSMR LBP: non specific mechanical recurrent low back pain, RMS: root mean square, PPR: preprogram reaction, VRPPR: voluntary response preprogram reaction, IO: internal oblique, TrA: transverse abdominis, EMG: electromyography, GC: gastrocnemius, TA: tibialis anterior, Long: longissimus, Ilioc: iliocostalis, FRP: flexion-relaxation phenomenon, McGill Pain Questionnaire (MPQ), EO: external oblique, ADIM: abdominal drawing-in maneuver, MVIC: maximal voluntary isometric contraction, MF: multifidus, ES: erector spine, BSE: bridging sling exercise, BBE: bridging ball exercise, NBE: normal bridging exercise.
ES muscle activity in the participants with and without LBP over an unstable surface.
EO muscle activity in the participants with and without LBP over an unstable surface.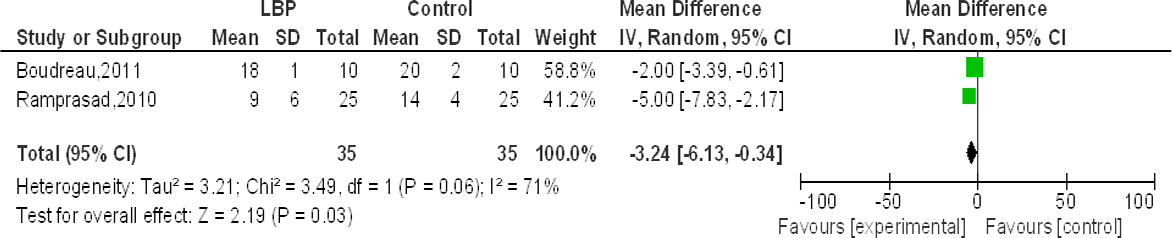
The required information was obtained from full-text articles of the included studies. The following relevant data were extracted: study design; the name of authors and the year of study publishing, the characteristics of the participants; the number of participants in each group; the measurement tools; the assessed muscles; the test position and the outcome measures (Table 4). We categorized the results of all studies according to the methodological differences between the included studies, the length of using unstable surface, i.e. short- or long-term use, the level of the unstable surface, which includes different degrees of perturbation, the study of superficial or deep muscles, the timing of recorded muscle activity, i.e. PPR or VR and the stage of LBP (acute or chronic) in the evaluation of the muscle activity pattern on unstable surfaces (Table 5). According to the location of muscles related to the spine, the trunk muscles are classified into deep and superficial groups. The erector spine (ES), RA, gastrocnemius, tibialis anterior, external oblique abdominal (EO), gluteus medius, biceps femoris and Iliocostalis muscles are considered as superficial trunk muscles. The transverse abdominis (TrA), posterior fiber of internal oblique abdominal (IO), multifidus, and longissimus muscles are deep muscles which directly control the movements of vertebral column.
Due to the methodological inconsistencies between the included studies, we only included the extracted data of only five included studies into the meta-analysis [25, 26, 27, 35, 36]. We calculated the required data, such as standard deviation (SD), which were not reported in the studies using the SD formula [25, 26, 35]. When the data were not accessible from figures and graphs of the studies, and when it was not clear according to the information, we contacted the corresponding author (s) to obtain the requested “mean
If the data were accessible from figures and graphs, the required data were extracted using a Java-based Plot Digitizer program [37]. Then, we entered the data into the effect size calculator of REVMAN 5.1 software (Cochrane Collaboration, 2008) [38]. The statistical significance of the difference between means with 95% confidence intervals (CIs) was calculated by REVMAN [39]. A random effects model was used to carry out separate meta-analyses for different forms of perturbation conditions (different directions).
The heterogeneity of these studies was evaluated using the Chi
Result
Identification and selection of studies
The literature search identified 267 articles using the keywords, including 192 duplicates. Screening by title and abstract identified 38 studies as potentially relevant for the review. Twenty-five studies that did not meet the inclusion criteria were excluded. The most important reasons for exclusion were articles assessing postural control without muscle activity assessment on unstable surfaces; articles with the evaluation of muscle activity during internal perturbation; articles with the evaluation of muscle activity during trunk perturbation, not surface perturbation. Two studies were also identified from hand-searching of the reference lists in the included studies, of which one was not retrievable in the abstract or full manuscript form. After the evaluation of exclusion criteria of studies, the final number of articles that met the inclusion criteria was fifteen (see Fig. 3).
QUORUM flowchart of studies included in the review.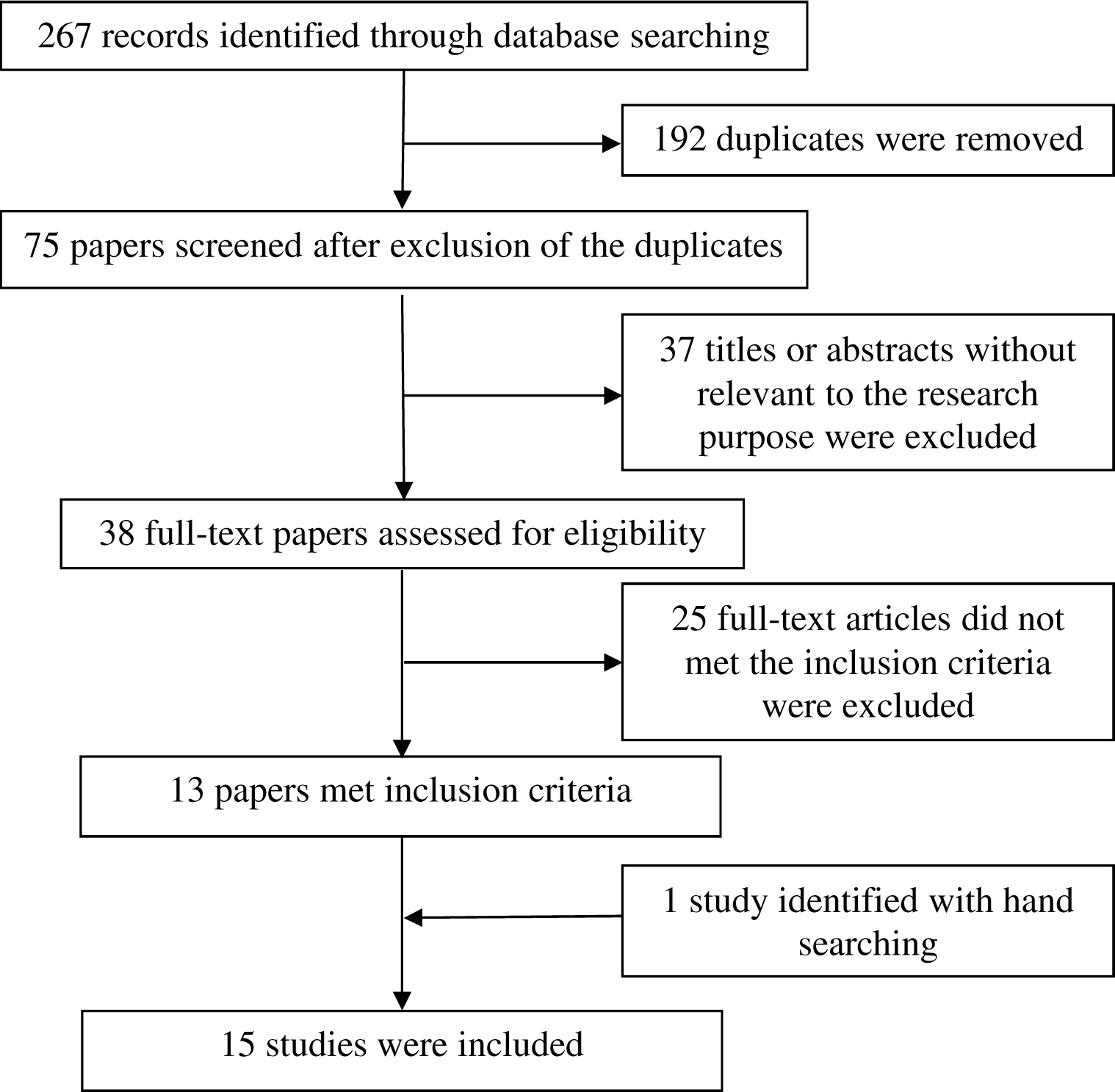
According to the study design in the included studies, PEDro or CASP scales were used for methodological quality assessment. For RCTs, the PEDro scores of the included studies with the mean score of 7/11 indicate good quality in clinical trial studies. Likely, the CASP checklist showed a good quality with the mean score of 7.5/11 in comparative studies. Tables 2 and 3 indicate the CASP and PEDro scores of the included studies, respectively [10, 12, 25, 26, 27, 28, 29, 35, 36, 40, 41, 42, 43, 44, 45].
Description of the included studies
In many included studies, chronic or recurrent LBP was examined [10, 12, 26, 28, 29, 35, 36, 40, 41, 42, 43, 44, 45], and only two studies evaluated patients with active or experimentally included LBP [25, 27]. To assess the severity of their pain, a Visual Analog Scale (VAS) was used in seven studies [10, 25, 26, 35, 36, 42, 45]. In the studies that noted pain intensity, the average of VAS was less than 5. Similarly, the Ostwestry Disability Index was used in seven included studies [10, 35, 40, 42, 43, 44, 45] and the Roland-Morris Disability Questionnaire was applied in three included studies [25, 26, 36] to assess the level of disability. The average of the disability index was less than 50% in all included studies [10, 25, 26, 35, 40, 42, 43, 44, 45] except one study [36]. According to the type of unstable surfaces, to examine the contribution of surface perturbation, unstable surfaces were manipulated by sliding movements in three studies [25, 26, 35] and tilting or sliding movements in the other studies [10, 12, 27, 28, 29, 36, 40, 41, 42, 43, 44, 45].
We investigated the effect of unstable surfaces on trunk muscle activity according to the findings of all included studies [10, 12, 25, 26, 27, 28, 29, 35, 36, 40, 41, 42, 43, 44, 45]. Because of different methodologies in the included studies, to quantify trunk muscle activity over unstable surfaces, various parameters were extracted, including mean latency, root mean square (RMS) amplitude, rectified amplitude in the early, and late-phase of muscle response, thickness change, muscle response percentage, muscles fatigue, and the flexion relaxation phenomena. The RMS amplitude and rectified amplitude of trunk muscles were most frequently reported as an outcome measure.
Overall, between groups, study findings were analyzed under three categories: category 1 includes studies that compared superficial and deep trunk muscles activities between healthy and LBP participants during perturbation over unstable surfaces [12, 25, 26, 27, 28, 29, 35, 36, 41]; category 2 contains the four studies that investigated the effect of different degrees of perturbations [29, 40, 44, 45]; and the third category includes the studies that evaluated the long-term effects of perturbations [10, 42, 43]. All included studies applied surface EMG for the evaluation of trunk muscle activity [10, 12, 25, 26, 27, 28, 35, 36, 41, 42, 43, 45], except three studies that examined trunk muscle activity using US [29, 40, 44]. Except two studies that assessed only back muscle activity, the other included studies examined abdominal muscles such as TrA, IO, EO, and RA [41, 42]. Also, except three studies that examined only abdominal muscle activity, back muscles activity was evaluated in the others [29, 40, 44].
In the included studies that investigated the immediate effect of perturbation, the data recording was limited to 2 minutes after perturbation [12, 25, 26, 27, 28, 29, 35, 36, 40, 41, 44, 45]. So, data about the PPR or VR amplitude of the muscles were extracted from included studies. The long latency responses between 40–120 millisecond (ms) are named PPR, and those greater than 120 ms were termed VR [34, 46]. As shown in Table 5, while in some studies patients showed higher VR amplitude in some superficial trunk muscles during perturbations [12, 25, 26, 35, 36], there were a number of studies which showed lower PPR amplitude in superficial trunk muscles in patients than healthy individuals [26, 27, 28, 36, 41]. Figures 1 and 2 summarize the pooled data extracted from three studies [26, 27, 36]. Both forest plots identify the effect of unstable surface on the PPR of trunk superficial muscle activity in participants with and without LBP. The meta-analysis results indicated the overall mean effect of perturbations over unstable surfaces on ES muscle activity (Fig. 1) and EO muscle activity in the patients with LBP as compared to healthy participants (Fig. 2).
Although the number of studies in each meta-analysis is limited, the finding of this meta-analysis shows that PPR of some superficial muscles decreased significantly in the patients than healthy participants on unstable surfaces [26, 27, 36]. This finding indicates that the PPR amplitude of some superficial muscles, such as ES and EO, which is important in the control of perturbation over unstable surfaces, shows a greater reduction in the patients than healthy participants [26, 27, 36]. In line with this finding, there are a number of studies, which also found a higher VR of trunk superficial muscles [12, 25, 26, 35, 36]. According to the differences in the methodology of included studies that assessed VR amplitude in trunk muscles, we could not have meta-analysis in this field. These results discriminated a higher VR and lower PPR of superficial trunk muscles in the patients with LBP as compared to the healthy participants during perturbation over unstable surfaces.
Deep trunk muscle activity was assessed in the five included studies during perturbation in the participants with and without LBP [25, 26, 29, 35, 41]. TrA and the posterior part of IO muscles are known as deep abdominal muscles [47, 48]. The test positions were standing in three [25, 26, 35] and sitting in two studies [29, 41]. Because of differences in methodology of the included studies in assessing the activity of trunk muscles, we could not have meta-analysis in this field. Overall, the results of the included studies showed significant reductions in deep muscle activity during perturbation over unstable surfaces in the patients as compared to healthy individuals. However, these studies applied surface EMG for evaluation of trunk muscle activity. Because the surface EMG would not be a reliable tool for measuring deep trunk muscle activity [49], the obtained findings from these studies should be considered cautiously.
As shown in the finding of some included studies, the effect of surface instability on muscle activity may be manipulated based on the rate of surface instability. Although some studies showed lower trunk muscle activity in the patients with LBP than healthy participants [29, 41], these demonstrated that trunk muscle activity was increased in the high degree of instability than stable surfaces in the patients with LBP [29, 40, 44, 45].
As indicated in Table 5, most studies investigated the immediate effect of perturbation on unstable surfaces on trunk muscle activity [12, 25, 26, 27, 28, 29, 35, 36, 40, 41, 44, 45] and the others examined the long-term effect of perturbations in the participants with and without LBP [10, 42, 43]. With reference to the studies that examined long-term effects of perturbations, data were not collected during the test, but during pre- and post-training [10, 42, 43]. However, results of these included studies indicated a significant improvement in trunk muscle activity pattern by using a Swiss ball instead of a stable surface in long-term training [10, 42, 43]. Therefore, the considered length of using an unstable surface (short- or long-term use) may cause diversity in the results [10, 29, 41, 43].
It seems that the results are not consistent among acute and chronic LBP stages. One study showed lower activity of the trunk superficial muscles in the acute LBP stage [27], while other studies detected a higher activity of trunk superficial muscles over unstable surfaces in the chronic or recurrent LBP stage [12, 35].
Discussion
The present systematic review was aimed to detect the evidence for the effectiveness of surface instability on trunk muscle activity in patients with LBP as compared to healthy individuals. The included studies do not indicate similar results, as some studies showed increased trunk muscle activity and a few studies showed decreased trunk muscle activity on unstable surfaces in the patients with LBP than healthy individuals. Some studies demonstrated a positive long-term effect of unstable surfaces on trunk muscle activity pattern in the patients with LBP.
It seems that different methodological differences between studies can affect the results. Study of superficial or deep muscles, the position of postural task on unstable surface (sitting and standing or supine with curl up), the timing of recorded muscle activity, i.e. PPR or VR, the length of using unstable surface, i.e. short- or long-term use and the level of surface instability which includes the degree of perturbations are found the important causes that impact on finding of included studies.
The effect of using unstable surfaces on the PPR and VR of superficial trunk muscles in patients with LBP as compared to healthy individuals
We hypothesized that unstable surfaces decrease the VR of superficial trunk muscles and increase PPR of superficial trunk muscles in patients compared to healthy individuals. This hypothesis was not supported by the finding of the included studies. The result of our meta-analysis shows that the patients comparing healthy participants cannot appropriately recruit the superficial trunk muscle in the PPR phase during perturbation over unstable surfaces (see Figs 1 and 2). These studies discriminated decreased PPR activity in the superficial trunk muscle during perturbation in the patients [26, 27, 36]. However, some of the included studies show a higher activity of the some superficial muscles in the VR phase during perturbation in the patients than healthy participants [12, 25, 26, 35, 36]. It seems that VR of the superficial trunk muscle may increase to compensate decreasing PPR of the superficial muscle in patients with LBP [36] (see Table 5). These changes in PPR and compensatory VR activity of the superficial trunk muscle may increase trunk stiffening and restrict trunk movement to avoid potentially injurious losses of balance in the LBP [50, 51, 52]. Changes in superficial trunk muscle activities in patients with LBP can affect motor control of trunk movements [48, 58]. Therefore, one of the potential explanations for inconsistencies in the findings about superficial trunk muscle activity may relate to the time of data recording (PPR or VR phases of muscle activation) during perturbation over an unstable surface.
The effect of using unstable surfaces on the activation of deep muscle activity in patients with LBP as compared to healthy individuals
The findings of the included studies did not support similar hypothesis based on deep trunk muscle activity during perturbation in patients than in healthy individuals. Overall, without considering methodological differences in the studies, a significant decrease in the activity of deep trunk muscle was shown in the five included studies during perturbation [25, 26, 29, 35, 41]. However, all studies, except that of Rasouli et al., applied surface EMG for the evaluation of deep trunk muscle activity [25, 26, 35, 41]. Accordingly, the reported findings from these studies should be considered cautiously. Rasouli et al. showed decreasing deep trunk muscle activity in the patients with LBP [29]. However, to determine firm conclusions about the effect of using unstable surface on the deep trunk muscle activity, more studies with sound methodologies are required.
The effect of surface instability levels on the activation of trunk muscles in patients with LBP
Another hypothesis of our systematic review study, trunk muscle activity in high instability levels of unstable surface is more than the low instability levels in the patients with LBP. In this line, although a meta-analysis was not administrated due to the methodological differences of the included studies, the results of included studies confirmed this hypothesis [29, 40, 44, 45]. These results were consistent with some studies that showed a greater activation of the superficial and deep trunk muscles on the conditions of higher instability [11, 53]. It seems that under differing degrees of stability, a high degree of surface instability challenge the motor control system and increases the demand on the stabilizing muscles. However, some studies showed a decrease trunk muscle activation over an unstable condition in the healthy individuals [54]. In this study, exercises were done for strengthening upper limbs and perturbation was made on upper limbs and upper trunk. Although this study discriminated the decrease in RA muscle activity, RA muscle was considered as primary mover rather than the stabilizer trunk muscle in this exercise condition. It seems that an unstable surface only may increase the VR of trunk stabilizer muscles to compensate impaired activity of primary muscles [53, 54, 55]. Thus, the type of the test in unstable surface condition can manipulate trunk muscle contribution as primary or stabilizer muscles in the movement.
The effect of unstable surface long-term training on the activation of deep trunk muscles in patients with LBP
We also hypothesized that the deep trunk muscle activity pattern would be increased in the patients during long-term periods using perturbation over the unstable surface. The findings of one the included studies supported this hypothesis [43]. This study showed a significant improvement in deep abdominal muscle activity during long-term training on a Swiss ball in the patients. Although they did not compare the results between participants with and without LBP, significant enhancement in the feed forward response of TrA muscle was observed in training over the unstable surface in the patients [43]. This finding was confirmed in some studies that showed significant differences in the unstable conditions compared to the stable surface training on trunk muscle activity [11, 29, 40, 44, 45, 56]. However, these studies assessed the effectiveness of unstable training on muscle activity only during a short period. One of the probable explanations for these results may be increasing the stabilizer muscular demand to maintain the trunk posture over the unstable surface compared to the stable conditions [15, 16]. To determine a firm conclusion about the effect of long-term training using unstable surface on the superficial and deep trunk muscle activity, more studies with methodological homogeneity are required.
Overall, although there are significant differences in superficial and deep muscle activity in the patients with LBP as compared to healthy participants during perturbation over unstable surfaces, these conditions may increase trunk stabilizer muscle activity in the patients with LBP when compared to baseline value [29, 40, 44, 45]. As a result, it seems that unstable surfaces as intervention have positive effects on deep trunk muscle activity in LBP patients [29, 41].
Other differences between findings of the studies may play a role, but could not be verified due to a lack of sufficient studies. For example, acute or chronic conditions of LBP may influence muscle activity. A few studies included acute LBP patients [25, 27], while the most studies investigated the muscle activity pattern on an unstable surface in chronic or recurrent LBP [10, 12, 26, 28, 29, 35, 36, 40, 41, 42, 43, 44, 45]. Comparing the results reveals that acute LBP may decrease the activity of muscles, such as EO and ES, during perturbation over an unstable surface [27]. However, there is evidence that acute pain may inhibit the muscle activity by activating nociceptor stimulators, which may affect motor neuron excitability and reflex responses [57, 58]. The other studies have shown increased superficial muscle activity during perturbation on surfaces using a trunk stiffening strategy in chronic or recurrent LBP patients than in healthy participants [25, 26, 35, 36]. The heterogeneity in the studies may suggest that more studies with larger sample sizes are required to draw a firm conclusion about the effect of unstable surface on the superficial and deep trunk muscle activity based on the stage of LBP.
Conclusion
The present systematic review indicates a lower PPR and higher VR of superficial trunk muscle and decreased activation of deep trunk muscle in the patients with LBP as compared to the healthy participants. Although unstable surfaces may have positive effect on trunk muscles activity in the patients with LBP as compared to their baseline values, reducing the ratio of deep versus superficial trunk muscles was shown during perturbation over unstable surface in the patients as compared to healthy participants. Accordingly, it seems that training over the unstable surface should not be suggested for the first stage of training. We recommend starting the training by using static motor control training tasks to correct impaired trunk muscle activity patterns, i.e. enhance activity of deep muscles compared to the superficial muscles, in the LBP patients. Then, the static training should be progressed into more dynamic tasks such as training over unstable surfaces.
Limitations and areas for future research
There are some limitations in our study. The current review was limited to English-language articles. Because of the methodological and design differences of the included studies and their small number, we could not perform meta-analysis for all included studies. The most of the studies investigated the effect of unstable surfaces on superficial trunk muscle patterns in patients with LBP [12, 16, 27, 28, 36, 42], but little is known about the activity of deep trunk muscles, such as TrA and Multifidus (MF) [29, 40, 41, 43, 44, 45]. This review suggests performing similar studies by testing the effect of unstable surface on the deep trunk muscle activity with different levels of surface instability in patients with LBP.
Conflict of interest
The authors report no conflict of interest.
Footnotes
Acknowledgments
This project was supported by Neuromuscular Rehabilitation Research Center, Semnan University of Medical Sciences, Semnan, Iran. We are thankful for all supports we given in this work.