
Abstract
OBJECTIVE:
This study compared the dietary habits of patients with ankylosing spondylitis (AS) and rheumatoid arthritis (RA).
METHODS:
The nutritional status of 56 patients, seen at the Rheumatology Outpatient Clinic and diagnosed with RA based on the ACR-2010 criteria, was compared with that of 28 patients diagnosed with AS using the modified New York criteria. Nutritional status was determined using a form that was filled out during face-to-face interviews with all patients. Patient demographics, disease activity, smoking and alcohol use, concomitant diseases, disease duration and nutritional status were determined using a questionnaire.
RESULTS:
RA patients consumed butter on 2 days a week, and AS patients on 1 day per month. Yoghurt was consumed by RA patients daily and by AS patients 3 days a week.
CONCLUSIONS:
Compared to the diet of AS patients, the diet of RA patients was richer in protein and lipids. The impact of diet on these two diseases remains to be determined in large-scale studies.
Introduction
Study flowchart.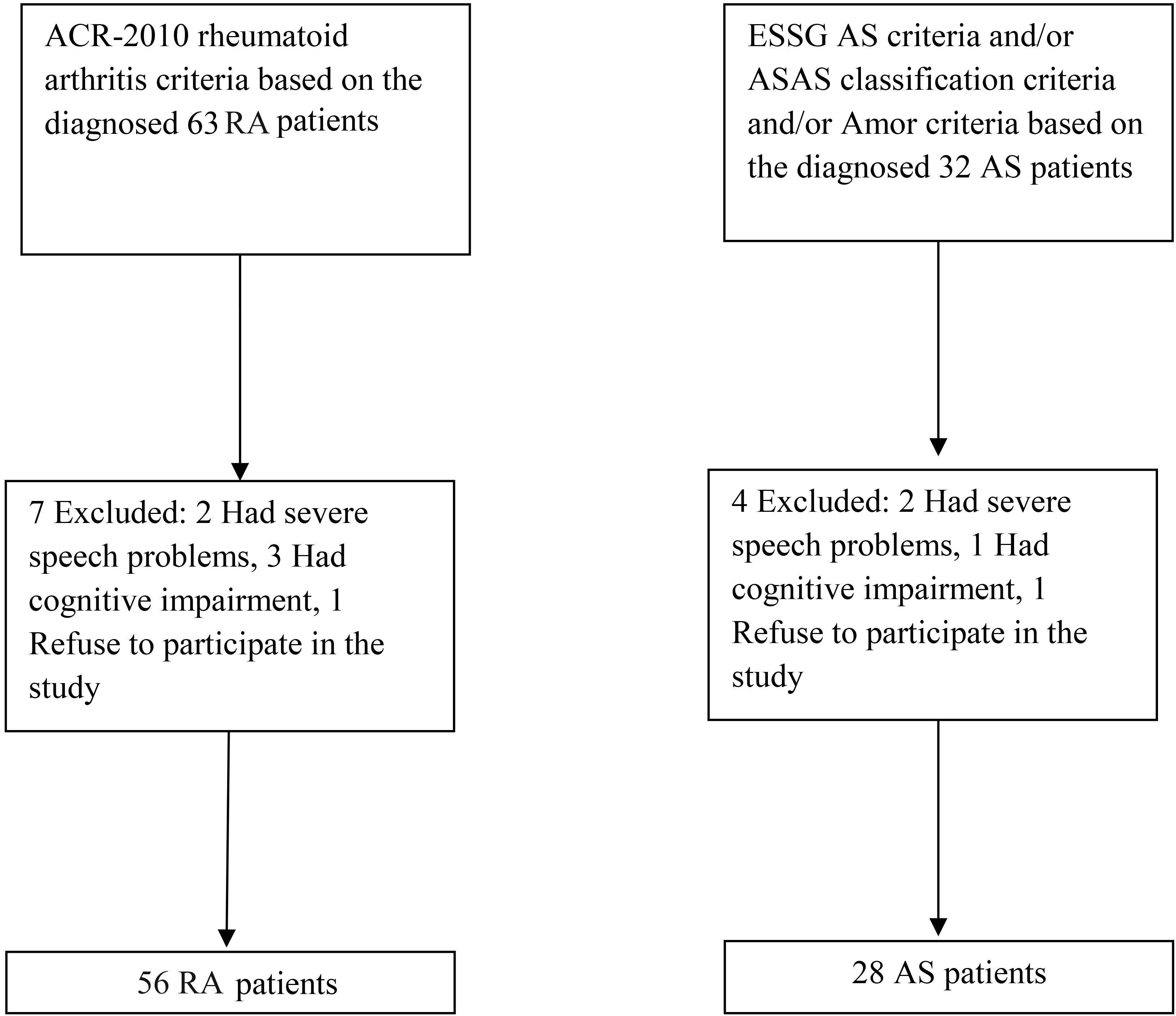
Rheumatoid arthritis (RA) is a chronic joint disease characterised by synovial inflammation and erosion of the cartilage, leading to destruction of the involved joint over time. The aetiology of RA is unknown, but both genetic and environmental factors have been implicated in disease susceptibility and development [1, 2].
Ankylosing spondylitis (AS) is a chronic systemic inflammatory disease that affects mainly the axial skeleton and causes significant pain and disability [3]. It may lead to structural impairment and the loss of important dynamic functions, thus compromising the performance of daily activities. Extra-articular manifestations are common, with restrictive respiratory dysfunction frequently reported in a significant proportion of patients. Environmental, genetic, hormonal, and (probably multiple) unknown factors have been implicated in the development of AS. Diet is one of the environmental factors thought to be involved in the etiopathogenesis of this disease and should be monitored, during treatment and follow-up, in AS patients [3, 4].
Several studies have shown that a Mediterranean diet, rich in fish, olive oil, cooked vegetables and fruit, has a protective effect against RA, perhaps due to its high omega-3 content [5, 6]. However, another study showed that the consumption of red meat had no effect on the risk of developing RA [7].
The possible benefits of specific diets for patients with RA have been tested in previous trials, but the conclusions drawn from those studies were conflicting, and those reporting positive results of dietary therapy were not published in peer-reviewed journals [8]. Therefore, the aim of this study was to compare the dietary habits of AS and RA patients.
This randomised, prospective, controlled, single-blind study was conducted at the Physical Medicine and Rehabilitation department of Bezm-i Alem Vakıf University, Faculty of Medicine, Istanbul, Turkey. The nutritional status of 56 patients, who were seen at the Rheumatology Outpatient Clinic and diagnosed with RA based on the ACR-2010 criteria, was compared with that of 28 patients diagnosed with AS using the modified New York criteria. Nutritional status was determined using a form that was filled out during face-to-face interviews with all patients (Fig. 1). Patient demographics, disease activity, smoking and alcohol use, concomitant diseases, disease duration and nutritional status were determined using a questionnaire.
Nutritional status was indexed by alcohol and smoking habits, breakfast frequency, daily water consumption, salt intake, and the frequency of fast food, egg, milk, yoghurt, cheese, wheat, cereal, whole-wheat bread, white bread, butter and margarine consumption. For each question, the answer options were as follows: every meal, every day, 3 times a week, 2 times a week, once every 15 days, once a month and “I don’t know”.
In addition to the demographic characteristics (age, sex, weight, height, body mass index), the patients were asked about their occupation, main symptoms, time of diagnosis and drug usage (non-steroidal anti- inflammatory drugs and disease-modifying antirheu- matic drugs, including biologics).
Inclusion criteria
Patients aged 20–65 years who were able to understand the content of the questionnaires were included in the study. For the RA patients, additional inclusion criteria were a disease duration
Exclusion criteria
Patients practicing regular exercise during the previous 6 months, those with concomitant systemic disease, and those administered an anti-tumour necrosis factor drug were excluded from the study.
AS disease activity was evaluated using the Bath AS Disease Activity Index (BASDAI) [9]. The reliability and validity of the Turkish versions of the BASDAI and Bath Ankylosing Spondylitis Functional Index (BASFI) have been demonstrated [10].
For the RA patients, Disease Activity Score-28 (DAS28) parameters, including high-sensitivity C-re- active protein (hsCRP), tender joint count (maximum, 28 joints), swollen joint count (maximum, 28 joints) and the patient’s self-assessed global well-being (100-mm visual analogue scale) were calculated [8, 11].
The erythrocyte sedimentation rate (ESR) was measured using the Westergren method (mm/h), and the CRP level using nephelometry (mg/dl).
Measurements of patient body weight and fat mass were used to calculate the body fat percentage.
All patients finally included in the study signed an informed consent form before participating. The study was approved by the local Ethics Committee.
Statistical analyses were performed using SPSS for Windows software (ver. 16.0; SPSS Inc., Chicago, IL, USA). The Kolmogorov-Smirnov test was used to confirm a normal distribution of the data of both groups. A non-parametric test was employed to analyse variables with a non-normal distribution. Data from the two groups were compared using the independent-samples t-test. Statistical significance was based on a p value
All procedures used in the study were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2008.
Demographics and habits of the patients
Demographics and habits of the patients
The demographic information of the 56 RA and 28 AS patients is shown in Fig. 1. Data on alcohol and smoking habits and breakfast regularity are presented in Table 1. Average food and drink consumption are reported in Tables 2 and 3. RA patients had a mean body fat percentage of 35.82
The food average consumption frequency
The food average consumption frequency
The drink mean consumption frequency
There were no significant correlations between either the BASDAI or the DAS28 score and food consumption or other lifestyle habits (
A PubMed search using “diet” and “RA DAS28” as the keywords yielded only five hits, with an additional one result that was deemed invalid. A similar search for AS yielded 41 results but, overall, studies on AS disease activity are scarce. Our results showed that butter was consumed on average by the RA patients on 2 days a week, and by the AS patients on 1 day a month. Yoghurt was consumed by RA patients daily, and by AS patients on 3 days a week. Our results showed that, compared to the diet of the AS patients, the diet of the RA patients was richer in protein and lipids. In both groups, most of the study participants were men, consistent with reports in the literature (Table 1).
In the study of Hayashi et al., serum leptin and albumin levels were significantly lower, and inflammatory markers were increased, in their high disease activity group. An assessment of the dietary intake of those patients showed a lower intake of fish oil, and a lower intake of monounsaturated fatty acid versus other fatty acids. The DAS28 score correlated negatively with the proportion of monounsaturated fatty acid consumed relative to total fatty acid consumption, but positively with serum oxidative stress markers (reactive oxygen metabolites). The salivary levels of reactive oxygen metabolites correlated with CRP and serum reactive oxygen metabolite levels [12].
Shinebaum et al. examined whether disease activity could be lowered by elimination of possible sources of Klebsiella from the diet, such as cold meat and salads [13], but there were no significant differences between the control and experimental groups. Ebringer and Wilson discussed the efficacy of a diet also aimed at reducing Klebsiella substrates in the colon through reducing the dietary intake of starch [14]. However, to date, no controlled study has examined the effect of a low-starch diet in patients with AS. Appelboom et al. reported a small study in which milk products were excluded from the diets of patients with AS, spondyloarthropathies (SpA) and RA [15]. Positive effects were reported for patients with AS or SpA, but not for RA patients. In our study, wheat bread consumption was higher in the AS than in the RA patients. Cheese, white bread and cereal consumption did not differ between the two groups.
Altered serum adipokine levels and decreased albumin levels may reflect the joint deterioration induced by RA. Increased levels of oxidative stress markers in the serum and saliva of RA patients have also been reported (reference). A previous study showed that omega-3 polyunsaturated fatty acids, fish oil and monounsaturated fatty acid ameliorate disease activity and may confer beneficial effects by decreasing inflammation [12].
A recent study was unable to show a correlation between diet and AS disease activity, as assessed using the BASDAI, but did demonstrate a negative correlation between the dietary intake of long-chain omega-3 fatty acids and the ESR. Also in that study, the plasma phospholipid content of arachidonic acid correlated significantly with the BASDAI score. There were also correlations between the intake of long-chain omega-3 fatty acids and high-density lipoproteins and serum triglycerides. The arachidonic acid content of plasma phospholipids and disease activity, assessed using the BASDAI, were also positively correlated in patients with AS. In a group of Swedish AS patients, there was no correlation between diet and disease activity [16, 17]. Similarly, in our study, there was no obvious relationship between the dietary habits of the AS patients and the BASDAI score.
Sköldstam et al. studied the relationship between a Mediterranean diet and DAS28 scores using the Health Assessment Questionnaire, a health survey on quality of life (short form-36). The results indicated that patients with RA, after adjusting to a Mediterranean diet, showed reduced inflammatory disease activity, an increase in physical function and improved vitality [18]. In our study, there was no correlation between the DAS28 score and milk, yoghurt, cheese, wheat bread, white bread, butter, margarine, or cereal consumption.
The beneficial roles of omega-3 polyunsaturated fatty acids, found in high amounts in fish oil, in RA include a decrease in the inflammatory response, better immune function and a reduction in symptom severity [19]. Another study showed that fish oil supplementation decreases the need for medication in RA patients [20]. Dietary supplementation with olive oil has been suggested to improve clinical and laboratory parameters of disease activity in patients with RA [21], and to lower the risk of developing this disease [22]. In our study, milk, yoghurt, butter and margarine consumption was higher in the RA than in the AS patients.
Treatment of AS patients with high- and low-dose omega-3 supplements for 21 weeks produced a greater (although not statistically significant) improvement in the BASDAI score of the high-dose group [23]. In our AS patients, there was no correlation between milk, yoghurt, cheese, wheat bread, white bread, butter, margarine or cereal consumption and disease activity.
Given that there have been few previous studies on the role of diet in RA and AS, a cross-sectional study design without a control group was chosen as an effective starting point for this research, and to inform further studies. Thus, a major strength of this study was the relatively large and comprehensive cohort of patients included who had a verified diagnosis of RA or AS. The study used a validated and robust instruments, and the dietary habits of all of the included RA and AS patients attending our rheumatology clinic, in Istanbul were recorded. The impact of diet on these two diseases remains to be confirmed in large-scale studies.
The English in this document has been checked by at least two professional editors, both native speakers of English. For a certificate, please see:
Footnotes
Conflict of interest
The authors report no conflict of interest.