
Abstract
BACKGROUND:
Osteoporosis usually develops gradually and progresses without significant signs and symptoms. It is one of the most common musculoskeletal conditions associated with aging.
OBJECTIVES:
To evaluate the effects of whole body vibration (WBV) or magnetic therapy in addition to standard pharmacological treatment on bone mineral density (BMD) in elderly individuals being treated for osteoporosis.
METHODS:
Eighty-five participants, 60–75 years of age, were randomly divided into three groups. All three groups received the same standard pharmacological treatment comprised of vitamin D, calcium, and alendronate sodium. In Group I, thirty participants were also exposed to WBV for 25 minutes in each session with two sessions per week for 4 months. In Group II, thirty participants were exposed to magnetic therapy for 50 minutes in each session with two sessions per week for 4 months. In Group III, twenty-five participants received only pharmacological treatment. Dual-energy X-ray absorptiometry was used to measure BMD of the lumbar spine and femoral heads before and after interventions. Venus blood sample was drawn for analysis of calcium and vitamin D.
RESULTS:
An ANOVA test detected significant (
CONCLUSIONS:
Addition of either WBV or magnetic therapy to standard pharmacological treatment for osteoporosis significantly increased BMD in elderly subjects. No significant difference in effectiveness was detected between these two alternative therapy modalities. Consequently, either WBV or magnetic therapy could be effectively applied in conjunction with pharmacological treatment to increase BMD in elderly osteoporotic patients.
Introduction
Osteoporosis is a chronic systemic skeletal disease which is usually characterized by gradual reduction of bone mineral density (BMD) [1, 2]. Osteoporosis is one of the common causes of morbidity in elderly individuals [3, 4] and dramatically increases with advancing age [5, 6] especially when combined with other risk factors such as menopause, prolonged cortisone therapy, low calcium intake, smoking, alcohol consumption and physical inactivity [5]. Osteoporosis increases risk of repeated fractures and co-morbid complications that may result from otherwise trivial trauma and mild stresses [2, 3, 4] and it places a huge financial burden on health services [5]. Although pharmacological treatments including hormonal therapy, vitamin D and calcium are commonly prescribed as main line treatment [4], non-pharmacological management is a tangible part of the long-term prevention and treatment for osteoporosis [7]. Adequate intake of vital nutrients and minerals in addition to lifestyle changes and an increase in active exercise are emphasized as effective interventions [1, 4, 7, 8, 9, 10, 11, 12, 13]. Another non-pharmacological treatment, magnetic therapy, is a physical therapy modality that is both feasible and safe [14, 15]. Magnetic therapy is recommended as an alternative regimen for treatment of osteoporosis in both animals [16, 17, 18, 19] and humans [4, 20, 21, 22]. Pulsed electromagnetic fields (PEMFs) applied in magnetic therapy can stimulate osteogenesis by increasing osteoblastic activity and decreasing osteoclast formation [23]. Thus, magnetic therapy has the potential to enhance bone cell formation and increase BMD of osteoporotic bones [15]. Magnetic therapy [4, 14, 19] could therefore be an alternative therapy to traditional physical therapy modalities such as increased physical activity or strength building exercises for increasing BMD in older individuals [8, 24, 25, 26].
Flow diagram of patients’ recruitment.
Whole body vibration (WBV) is a novel mechanical stimulus, low-impact alternative therapeutic exercise to combat bone loss, increase bone mass and optimize peak bone in older subjects without the associated risks and effort of strenuous exercise [1, 27]. WBV training is a relatively new and promising non-pharmacological method for prevention of BMD decline [1]. WBV is generated in oscillating platforms and transmitted through the feet to the bones and muscles of the whole body [28]. However, the results of clinical trials investigating the impact of WBV on BMD are conflicting [29, 30, 31]. Recently some authors found that 12 months of WBV therapy did not alter BMD [29], but others found that treatment can strengthen weak muscles [30]. Beck and Norling [31] found that WBV for two sessions per week over 8 months increased hip BMD and balance performance more than walking exercise [31].
WBV and magnetic therapy are appealing alternatives to weight bearing exercises such as walking, which can be difficult for elderly individuals due to aging complications such as muscle weakness and a loss of balance [4, 32, 33, 34]. As the aging population grows, so does the need for alternative interventions for the prevention and treatment of osteoporosis. The aim of the study presented here is to evaluate the impact of WBV or magnetic therapy when combined with pharmacological treatment on osteoporosis. The null hypothesis tested here is that no difference in effectiveness in the management of osteoporosis will be observed with WBV or magnetic therapy when combined with pharmacological treatment, compared to pharmacological treatment alone.
Study design: Experimental study was conducted as a blind, randomized clinical trial.
Subjects
One hundred older participants, both males and females, were recruited by a consultant in orthopedic surgery and screened based on patient history and physical examination (Fig. 1) in accordance with the following criteria.
Inclusion criteria
Osteoporotic patients included in the study ranged in age from 60–75 years old with a T-score of (
Exclusion criteria
Participants with cognitive impairment, dizziness, arrhythmias, pacemaker, bone fragility, fractures within the past six months, other metabolic bone diseases, cancer, joint replacements, internal fixations, hormonal therapy in the past 12 months, bisphosphonates or bone altering medications in the past 3 months, long-term glucocorticoid or any other conditions known to interfere with usage of either WBV or magnetic therapy were excluded [1, 27, 29, 32].
Randomization
Every participant signed a consent form and was informed that collected data would be submitted for publication. Out of the 100 patients screened, only 85 osteoporotic participants were randomly assigned to three groups based on a computer-generated randomized number opened from a sealed envelope and communicated by an independent blinded research assistant (Fig. 1).
Study approval
Ethical approval was given by the Institutional Review Board (IRB-2013-04-037) of Imam Abdulrahman Bin Faisal University prior to starting participant assessment and therapeutic intervention.
Instrumentation
Quantitative instrumentation
BMD quantification: Dual-energy X-ray absorptiometry (DEXA; GE Medical Systems, USA), a bone densitometer, was used to measure BMD at the lumbar spine (L3–L5) and at both right and left femoral heads before and after each therapeutic intervention in all three groups [38, 39].
Calcium and Vitamin D quantification: Plastic syringes were used to draw venous blood samples from the anti-cubital vein for analysis of serum concentrations of both calcium and vitamin D. Plastic tubes were covered with foil during phlebotomy and transport to protect vitamin D from ultraviolet degradation.
Demographic data of patients’ sample
Demographic data of patients’ sample
BMI: body mass index *: Significant (
WBV Therapy was administered with the DKN Technology XG5 Pro, a whole body vibration (WBV) therapy machine. The XG5 Pro has a high tense carbon reinforced steel platform, an electronic personal trainer with 4 preset programs with durations up to 10 minutes in 30 second intervals, and visuals for independent body parts or the whole body. The machine dimensions are 33.5
Magnetic therapy was administered with the ASA magnetic field (Automatic PMT Quattro PRO). The instrument consists of an appliance, an adjustable electronic bed and solenoids as well as a couch with an 80-cm diameter sliding solenoid and two applicators The appliance generates PEMFs with a pulse repetition frequency up to 100 Hz and an intensity of 85 gausses [4].
Treatment procedure
Participants in all three groups were asked to maintain their daily life habits and to use the prescribed drugs for osteoporosis throughout the study.
Group-I
In addition to the prescribed medications for osteoporosis, participants of Group I received WBV therapy from a well-trained physical therapist responsible for supervising WBV therapy to ensure correct and safe use. Each participant was instructed to stand upright on the WBV platform with feet side-by-side, shoulder width apart, with hands fixed on the rail for increased stability and knees slightly flexed at a 20
Group-II
In addition to the prescribed medications for osteoporosis, participants of Group II received magnetic therapy. Each participant was exposed to low frequency, low intensity pulsed electromagnetic therapy. The magnetic device was applied to each participant from a comfortable supine position. After connecting the appliance to a power supply, the solenoid was adjusted over the affected parts of the body (lumbar spine and hip regions). Magnetic therapy was applied with a frequency of 33 Hz and an intensity of 50 gausses for 50 minutes in each session 2 times per week for 4 months [4].
Group-III
Each participant received only the prescribed medications for the treatment of osteoporosis with no additional therapy.
Statistical analysis
Data was statistically analyzed using SPSS (Version 22.0). Data from only 68 participants were included in the final analysis. A paired t-test was used to evaluate results within each group before and after intervention. Results included the mean T-score of BMD measured at the lumbar spine and right and left femoral heads in addition to serum levels of both calcium and vitamin D. A one-way ANOVA test was used to compare results among the three treatment groups before and after treatment. The ANOVA evaluation was followed with post hoc tests (LSD) to determine significances among the three groups. For all tests, statistical significance was determined at
Results
Demographical data of participants
There were no significant differences in the demographics including age, gender, weight, height, body mass index, and duration of osteoporosis incidence among the three treatment groups (
T-Score of bone mineral density of the lumbar spine pre-and post-therapeutic programs among three groups
T-Score of bone mineral density of the lumbar spine pre-and post-therapeutic programs among three groups
*: Significant (
T-Score of bone mineral density of the right femoral head pre-and post-therapeutic programs three groups
*: Significant (
T-Score of bone mineral density of the left femoral head pre-and post-therapeutic programs of three groups
*: Significant (
Significant increases in BMD based on the T-score of the lumbar spine, right, and left femoral heads were detected after treatment in Groups I and II, but not in Group III (
No statistically significant differences in BMD T-scores for the lumbar spine, right, and left femoral heads were detected among the three treatment groups prior to the described interventions (
Vitamin D and calcium levels
Significant increases in serum levels of both vitamin D and calcium after treatment were detected for all three groups (
Mean values of vitamin-D pre- and post-therapeutic programs in three groups.
Mean values of calcium level pre- and post-therapeutic programs in three groups.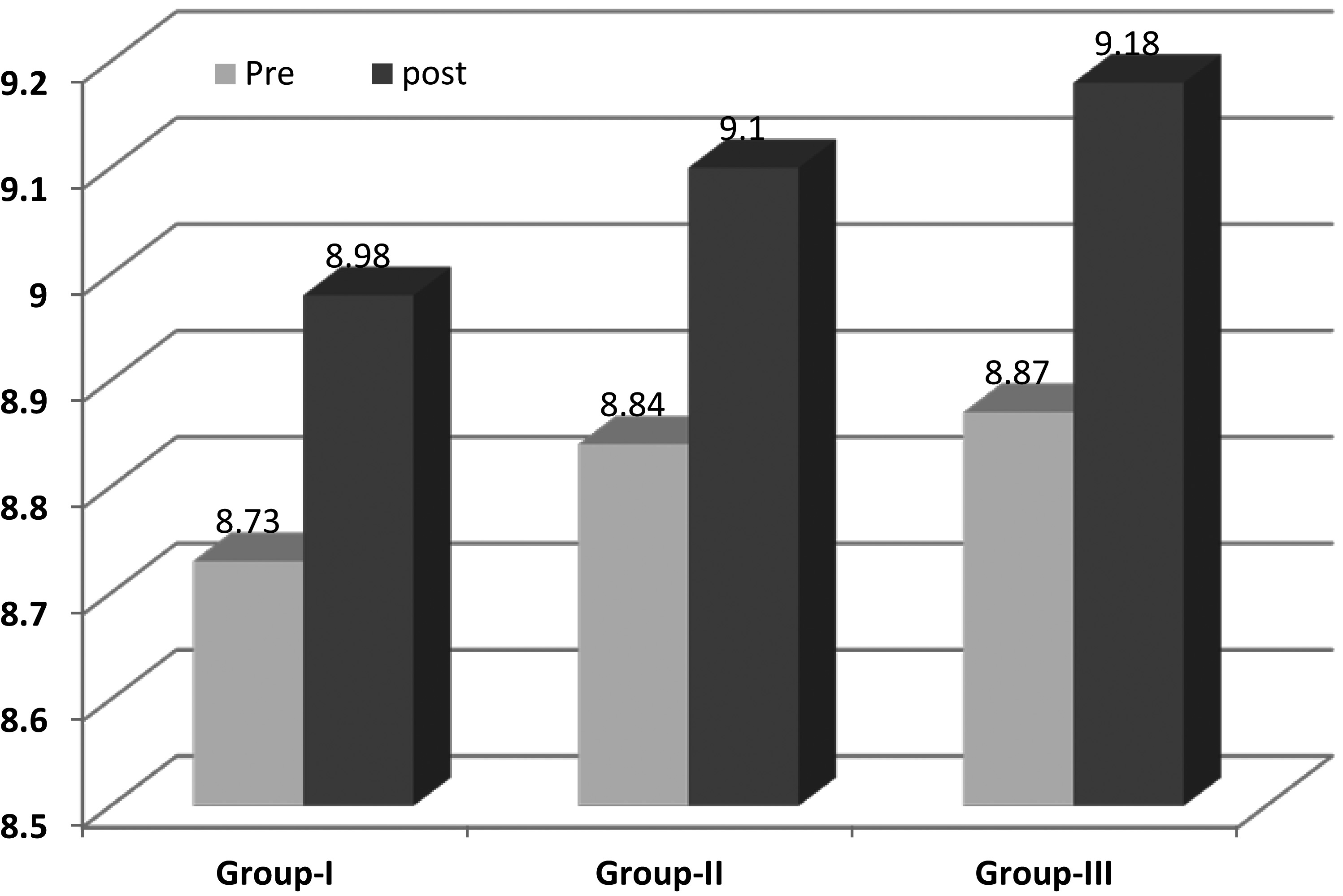
Osteoporosis is considered one of the most common and important health problems facing older individuals. It has been demonstrated that multi-component exercise programs based on strength, aerobic and/or weight-bearing training are beneficial to treating and preventing osteoporosis [8, 40]. However, some patients are limited in their ability to practice these exercises due to common complications related to aging such as muscle weakness, advanced osteoarthritis, neurological diseases and balance disturbance. Therefore, the availability of alternative physical therapy modalities with demonstrated effectiveness in treating osteoporosis when used in combination with pharmacological treatment would be tremendously beneficial, particularly for elderly patients [4].
The primary purpose of the study presented here was to evaluate and compare the effect of WBV therapy or magnetic therapy, in combination with pharmacological treatment, on BMD in elderly subjects with osteoporosis. BMD was evaluated in three regions, the lumbar spine, right, and left femoral heads and quantified using a “T-score”. The “T-score” was measured using DEXA, a commonly used radiological method to detect bone mineral density [18] that has been shown to reliably detect changes in BMD in osteoporotic bone [13]. Study results demonstrated a statistically significant improvement of BMD in all three areas after treatment with either WBV or magnetic therapy combined with pharmacological treatment. This improvement is in contrast to pharmacological treatment alone which resulted in no significant improvement in BMD.
Participants in all three treatment groups in this study received the same pharmacological treatment 1000–12000 mg/day of oral calcium supplementation, 10 mg/day or 70 mg/week of alendronate sodium, and 600 IU/day of vitamin D as recommended in literature [36, 37]. The recommendation of supplemental calcium and vitamin D for treatment of osteoporosis is based upon reports of a high prevalence of inadequate intake of these critical vitamins and minerals in elderly osteoporotic patients [41]. Furthermore, the supplementation of vitamin D3 and calcium was proven to have beneficial effects on increasing and maintaining BMD by enhancing the process of osteogenesis [42]. Consequently, the prevention and treatment of osteoporosis requires special attention to both calcium intake, which is a primary factor for bone health, and vitamin D, which improves calcium absorption [36, 37]. Thus, some researchers have proposed that adequate intake of calcium and vitamin D in addition to physical interventions or active exercise can synergistically improve the treatment of osteoporosis [36, 37]. The current study supports this approach, showing an enhanced increase in BMD when physical interventions such as WBV or magnetic therapy are combined with calcium and vitamin D supplementation. Other studies support these findings, reporting that vitamin D supplementation has no extra short-term skeletal benefit over calcium citrate supplementation in women with vitamin D insufficiencies [43]. In another study, investigators showed a reduction in bone loss at the femoral neck with calcium and vitamin D treatment, but results were not statistically significant [44]. While these studies do not conclusively demonstrate an effective increase in BMD based on vitamin D and calcium supplementation alone, a one year intervention study with calcium and vitamin D supplementation did show reduced bone turnover and significantly increased BMD in patients younger than 70 years of age. However, the effect of intervention in this study was positively correlated to physical activity, which emphasizes the importance of physical activity on positive results [45]. This further supports the conclusion of the study presented here, that for a significant positive impact on BMD in osteoporotic patients, calcium and vitamin D supplementation should be combined with physical therapy.
In addition to further supporting the importance of combining pharmacological treatment with physical therapy in combating osteoporosis, the study presented here demonstrates the effectiveness of two alternative modalities of physical therapy other than traditional physical activity and strength-building exercises. In support of the results presented here, previous studies have also reported increases in BMD with magnetic therapy, with one study specifically demonstrating an increase in BMD in older osteoporotic women after treatment [4, 14, 17]. Effects of magnetic therapy on BMD in osteoporotic participants can be explained by many mechanisms [14, 46, 47]. It was shown that magnetic therapy significantly suppressed trabecular bone loss and restored trabecular bone structure in bilateral ovariectomized rats [23]. Magnetic therapy may also stimulate calcification of the fibro-cartilage in the space between bony segments. Magnetic therapy can increase blood supply, which has been considered as a main source of improvement for bone healing, and may also stimulate osteogenesis, increasing osteoblastic activity [20]. In addition to the improvements in effectiveness of treatment, magnetic therapy also provides a non-invasive, easy, and safe method of direct treatment that can be targeted to specific sites in the body. It has even been suggested that magnetic therapy may prevent many older subjects from undergoing surgery [14].
As another alternative to traditional physical therapy, WBV has also been shown to significantly increase bone mineral density in this study as well as others [48, 49]. There is some agreement among researches that WBV therapy may be a suitable therapeutic modality for the prevention and treatment of osteoporosis [38, 50, 51]. It can be considered as a common exercise where individuals stand on an oscillating platform and the motor transmits vertical acceleration to muscle and bone [49]. One direct mechanism by which WBV is hypothesized to produce osteogenic effects is by changing the flow of bone fluid through bone stimulation and mechano-transduction. In addition, WBV may indirectly stimulate bone through activation of skeletal muscle by means of stretch reflex stimulation [52, 53]. WBV training can also produce an endocrine system response, increasing growth hormone and testosterone levels, indirectly affecting bone remodeling [54]. The positive effect of testosterone on BMD was detected in the forearm, the lumbar spine, and the hip in healthy men and women [1]. The WBV training has shown osteogenic effect in both college age individuals [3] and on the femoral neck in post-menopausal women [32]. The high-frequency and high-magnitude WBV has been applied on post-menopausal non-osteoporotic women, and it was found that vibration training improved isometric and dynamic muscle strength and significantly increased BMD of the hip [38].
While many studies support the results presented here, some clinical trials have contradicted these results. In several studies, the authors report non-signifi- cant benefit of WBV on post-menopausal bone measurements [29, 55]. Slatkovska et al. [29] applied WBV at 0.3G and either 90 or 30 Hz in addition to calcium and vitamin D supplementation for 12 months, measuring volumetric BMD (trabecular, cortical, and total) and bone structure (cortical thickness and trabecular thickness) at the distal tibia and distal radius as outcomes. Also measurement by the outcomes in Slatkovska et al.’s work did not show significant improvement with WBV therapy, the outcome measures differed from the current study in which is “T-score” of BMD at lumbar spine, right and left femoral heads are measured. Rubin et al. [55] also did not find significant changes in bone density after using either the WBV or placebo treatment, but the protocol for WBV use differed from the current study. Rubin et al. used a quiet standing posture to receive high-frequency, 30-Hz vibration, low-magnitude, 2.0 m/s
To the best of our knowledge, there is no direct clinical trial comparing WBV with magnetic therapy. The results of the current study revealed WBV produces greater increases in BMD in the lumbar spine and right femoral head (
Conclusions
Application of either WBV or magnetic therapy in combination with standard pharmacological treatment for osteoporosis increases BMD of the lumbar spine, right, and left femoral heads in elderly osteoporotic individuals. Usage of pharmacological intervention alone is not sufficient to achieve significant increases in BMD over a 4 month period. Thus, it can be concluded that application of either whole body vibration or magnetic therapy in combination with pharmacological treatment is a promising and effective method to treat osteoporosis in older individuals.
Recommendations
Further studies are needed to compare effects of WBV with that of magnetic therapy on BMD in older individuals using a larger sample size for a longer time and with long-term follow up.
Limitations
Limitations of the current study include a relatively short duration of treatment and evaluation (4 months) with measurements taken only before and after treatment with no long-term follow-up.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
The authors are grateful to all participants for their cooperation and to Mrs: Ibtihal Abdul-aziz and Mr. Adel Othman for their valuable efforts in data collection.