
Abstract
BACKGROUND:
Many practitioners recommend step-up and step-down exercises to increase muscle strength in the lower extremities. However, decreased stability of the hip joint and imbalanced muscle activities can alter limb biomechanics during these movements.
OBJECTIVE:
This study investigated muscle imbalance between the medial and lateral muscle components and between the proximal and distal muscle components by expressing the proportions of muscle activation in the step-up and step-down positions.
METHODS:
Nineteen subjects participated in the study. Activity of the vastus medialis oblique, vastus lateralis, semitendinosus, biceps femoris, adductor, gluteus medius, and gluteus maximus was assessed.
RESULTS:
The semitendinosus-biceps femoris ratio was higher in the step-down position than in the step-up position. The adductor-gluteus medius, adductor-vastus lateralis, and adductor-biceps ratios were higher in the step-up position than in the step-down position. The gluteus maximus-biceps ratio was greater in the step-down position than in the step-up position. In the hip joint, internal rotation was significantly greater in the step-up position.
CONCLUSIONS:
The transverse angle of the hip joint has a greater effect on the medial-lateral balance of the muscles surrounding the hip joint. Muscle activation in the medial hamstring is greater in the step-down position; in the adductor, muscle activation is greater in the step-up position. The step-down position is more appropriate for those with proximal weakness, as it can promote muscle activation in the gluteus maximus while maintaining biceps femoris activation.
Introduction
Muscle imbalance is a major factor involved in musculoskeletal disorders [3]. The ability to perform various lower extremities tasks without overstressing is associated with well-organised proximal stability and motor control in the hip joint; this involves a good balance of muscle activation between the medial and lateral muscle components and between the proximal and distal muscle components [4, 5, 6].
Decreased stability of the hip joint and imbalanced muscle activities in the hip and thigh can alter the joint’s biomechanical force on one side, which can also change the muscle function and aggravate muscle imbalance [7]. Moreover, the repetition of overloading in this situation can cause degenerative diseases because the joint stress associated with altered biomechanics is not dispersed adequately [7]. Thus, it is necessary to investigate the balance of muscle activation during common activities of daily life.
Many practitioners recommend step-up and step-down exercises because the hip abductors and hip adductors (AD) may provide additional pelvic stability and supplementary thigh acceleration during walking on ramps and stairs [8]. However, patients with diseases of the lower extremity have altered biomechanics while climbing/descending stairs. A previous study has suggested that knee osteoarthritis (OA) patients demonstrated greater hip abduction during foot strike and smaller peak knee flexion during support and swing [9] and that patients with hip OA demonstrated increased gluteus medius (Gm) muscle activation levels during stepping tasks when compared to controls [10]. For patients with chronic AD-related groin pain, the AD muscle strength was also significantly decreased on the affected side. Restoring the correct relationship between these two agonist and antagonist hip muscles may be an important preventative measure; therefore, it should be a primary concern of training and rehabilitation programs [1]. Therefore, the muscle ratios of the agonist and antagonist muscles of the hip and knee during activities of daily life need investigation.
However, to our knowledge, there has been no study of the medial-lateral and proximal-distal muscle ratios and the differences in these values between step-up and step-down activities. Therefore, we analysed muscle imbalance between the medial and lateral muscles and between the proximal and distal muscles by examining the proportions of muscle activation in the step-up and step-down positions and investigated the differences between both positions.
Subjects and methods
Twenty healthy women were recruited from a university community. One participant had hallux valgus and was excluded; therefore, nineteen subjects finally participated in this study. Volunteers were included if they had no prior lower back or extremity problems and were right-foot dominant. Exclusion criteria were as follows: significant neurologic disease, musculoskeletal disease, or other major systemic problems. The study was approved by the university ethics committee and the purpose and procedures of this study were explained to all subjects. Written informed consent was obtained prior to participation. This study adhered to the Declaration of Helsinki.
Step-up and step-down positions.
The ratios of the medial and lateral muscle activities and the ratios of the proximal and distal muscle activities.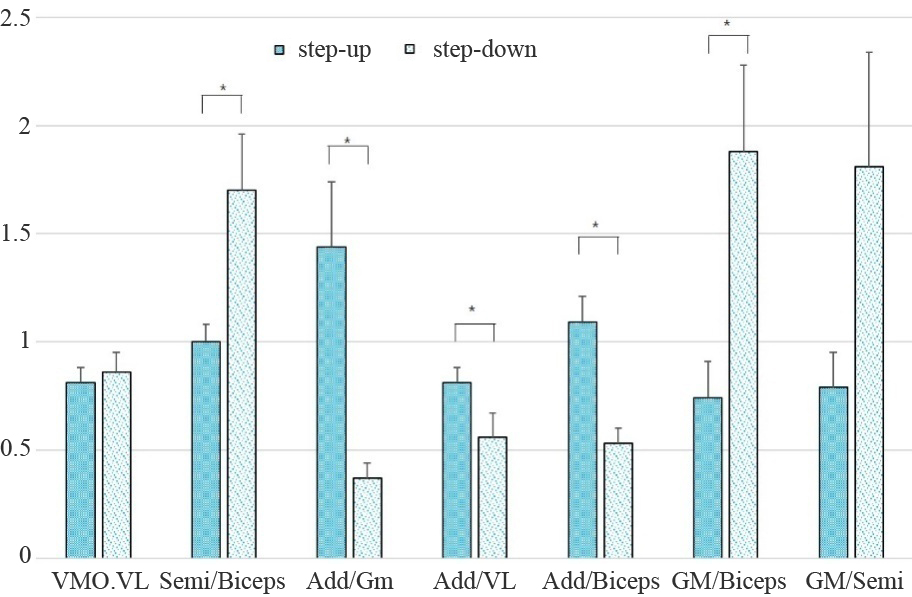
Each of the subjects performed the step-up and step-down positions with bare feet on a step box that had a standard height and depth (height, 16 cm; depth, 27 cm). We asked the subjects to step up and down on the box as naturally as possible and to pause movement when their foot landed on the step box. In the step-up position, the right foot, which was the forward limb, was placed on the step box and the left foot was placed on the floor. In the step-down position, the right foot was placed on the floor and the left foot was placed on the step box, with the participant in a comfortable position (Fig. 1). The step width and length were not controlled. We analysed the right leg because the right side was the movement side. Muscle activity was measured in the step-up and step-down positions. The electrodes were attached over the vastus medialis oblique (VMO) and vastus lateralis (VL), semitendinosus and membranosus (Semi), biceps femoris (BF), AD, Gm, and upper fibre of the gluteus maximus (GM). All electrodes (except for those for the GM and VMO) were applied according to the European recommendations for surface electromyography [11]. For the upper fibres of the GM, the electrodes were placed at a point midway on the line between the posterior superior iliac spine and the greater trochanter; this is a slightly modified version of the European recommendations for surface electromyography [11]. We selected the upper fibres of the GM due to avoid interference caused by pants. For the VMO, the electrodes were placed 4 cm proximal to the superior-medial angle of the patella at a 55-degree angle from the line of the femur [12]. For the surface electrode, an Ag/AgCl electrode (3 M, St. Paul, MN, USA) with a sampling rate of 1024 Hz was used. Signals were processed through a 20- to 500-Hz band-pass filter. During the step-up and step-down static positions, the surface EMG signal was collected in ten-second segments and measurements were performed three times for each position. The sEMG data obtained during the first and last second were removed, and only the data for the six seconds was used. The recorded total muscle activity was normalized to the maximal voluntary isometric contractions (MVC); the MVC were recorded prior to the tasks in the manual muscle testing position. The data were expressed as %MVC.
A Falcon System (Motion analysis, Santa Rosa, CA, USA) with six cameras was used to capture the joint angle in the step-up and step-down positions. Each camera was set to acquire 60 frames per second, with the sampling rate set at 60 Hz. Data analysis was performed using EvaRT 4.0 and Orthotrak 5.0 with the Helen Hayes market set (Motion analysis, Santa Rosa, CA, USA). Motion data were captured for ten seconds each in the step-up and step-down positions. The average value was expressed.
We analysed the %MVC and ratios of the medial and lateral muscle activities (VMO and VL; Semi and BF; AD and Gm; AD and VL; and AD and BF) and the ratios of the proximal and distal muscle activities (GM and BF; GM and Semi) because it was easy to recognize muscle imbalance and stability in these areas.
The results were expressed as mean
The muscle activities in the step-up and step-down positions
*Significant difference between the step-up and step-down positions.
Nineteen women participated in this study. The average age of the participants was 21.4
Joint angles in the step-up and step-down positions
Joint angles in the step-up and step-down positions
*Significant difference between the step-up and step-down positions. Hip extension, adduction, internal rotation and knee flexion are in the positive direction.
This study investigated muscle imbalance between the medial and lateral muscles and the stability between the proximal and distal muscles by examining the proportions of muscle activation in the step-up and step-down positions. We found that muscle activation in the medial hamstring is greater in the step-down position; in the AD, muscle activation is greater in the step-up position; in the hip joint, internal rotation is greater in the step-up position. We also found that the GM is more activated in the step-down position than in the step-up position.
The first finding of this study was that the Semi-BF ratio was lower in the ascending position than in the descending position, which indicates that the BF was dominantly activated in the ascending position. In our study, the angle of hip internal rotation was greater in the step-up position. This means that the BF controls the hip angle eccentrically in the step-up position. A previous study suggested that the long head of the BF muscle, but not of the Semi, contributed support during the loading response when ascending stairs. The study also suggested that the Semi is activated more during the swing phase when descending stairs, which is the same trend that we observed [13].
The second finding was that the AD muscle was more activated in the ascending position than in the descending position. A previous study reported that AD longus activities during the mid-swing phase while ascending stairs were greater than during descending stairs [8]. Additionally, when the hip is flexed, the AD muscle plays a role in assisting the hip extensor according to the moment arm vector concept. The extension role of the hip AD may assist in leaping and lifting when the hip is flexed [14]. Therefore, it seems that greater AD muscle activation was observed when ascending stairs.
The transverse plane angle of the hip joint showed significant differences between two positions but not of the frontal plane angle. Based on the first and second findings, it can be seen that the transverse angle of the hip joint has a greater effect on the muscle medial-lateral balance surrounding the hip joint. A previous study reported that subjects demonstrated more adducted and internally rotated hip positions while ascending stairs than while descending stairs, which is more aggravating for patients with patellar femoral pain syndrome [2]. Therefore, control of the transverse plane angle of the hip joint is considered clinically important for hip joint muscle balance.
In addition, we found that the GM-BF ratio is greater in the descending position. GM activation was greater in the descending position and the GM was the principal hip extensor that was active during the loading response [13]. Therefore, it is suggested that the step-down position is more appropriate for training those with proximal weakness, as it can promote muscle activation in the GM while maintaining BF activation.
This study had several limitations, including the small sample size and the fact that all the participants were healthy women. Another limitation was that we measured muscle activities only in the static position. We were unable to determine muscle activities during the step-up and step-down movements. Therefore, follow-up studies are needed to study the movements, which will provide further in-depth knowledge regarding muscle activities and ratios. This will enable clinicians to recommend the most suitable exercises to patients.
Footnotes
Acknowledgments
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT and Future Planning (grant No. 2015R1D1A3A01019272).
Conflict of interest
None to report.