
Abstract
BACKGROUND:
Malignant peripheral nerve sheath tumor (MPNST) arising in benign schwannoma with multiple intraosseous spinal metastasis is extremely rare, having a highly aggressive progression and poor prognosis. In such cases, the malignant cells of MPNST usually have an epithelioid morphology. Here, the authors present a very rare case of spindle cell type MPNST arising in benign schwannoma.
CASE:
A 47-year-old woman had a history of wide marginal excision of right buttock spindle cell sarcoma previously. However, metastatic lesions to C7, L1 body, and the right lung were detected during follow-up. Total spondylectomy and stabilization of the C7 and L1 tumors were performed within an interval of 5 months. However, the patient expired 6 months after the last surgery. From analysis and study of three tumor specimens (right buttock, cervical and lumbar spine), the pathological diagnosis based on histomorphologic and immunohistochemical studies was spindle cell sarcoma, high grade, most consistent with MPNST arising in schwannoma.
RESULTS
: It is important that pathologists and surgeons recognize that spindle cell type MPNST may arise in benign schwannoma, as this recognition aids in assessment of patients with schwannoma and contributes to the pathologist making a more precise diagnosis, and the surgeon better determining the appropriate therapeutic options and surgical methods.
Introduction
A 47-year-old female complained of left upper extremity motor weakness and severe radiating pain. 
Malignant peripheral nerve sheath tumors (MPNSTs) are soft tissue malignant tumors that usually arise from major or minor peripheral nerves and show variable differentiation toward one of the cellular components of the nerve sheath [1, 2]. MPNSTs account for approximately 5% to 10% of all soft tissue tumors and the incidence of MPNSTs in the general population is 0.001% [3, 4]. Approximately one-half of MPNSTs develop from a neurofibroma, commonly in patients with neurofibromatosis type 1 (NF-1) [5]. However, the incidence of MPNSTs due to the malignant transformation of schwannoma is very rare; only around 20 cases have been reported in the English literature (PubMed search, with no publishing date limitation) [6, 7]. Furthermore, malignant transformation of MPNST usually presents with epithelioid features in most malignant tumor cells.
Here, we report the case of a patient with an intraosseous spinal metastasis of the spindle cell type MPNST arising in benign schwannoma. To the best of our knowledge, this is the first reporting of such a case.
Clinical summary
A 47-year-old woman with a 1-month history of motor weakness and severe radiating pain to her left upper extremity was transferred from another regional hospital to our hospital. The patient had a history of wide marginal excision with good margin of right buttock spindle cell sarcoma, which had been performed at the other hospital some 30 months previously. During follow-up, she was detected osteolytic destructive lesion of the C7 body and was transferred to our hospital with a diagnosis of spinal metastasis. On physical examination, the pain was situated in the left scapular, posterior arm and medial forearm. It was also associated with decreased sensation in the left medial forearm. No tenderness was noted around the neck. A neurological examination revealed clumsiness and motor weakness of the left upper extremity (Grade 5 motor strength in elbow flexion, Grade 3 in elbow and wrist extension, and Grade 2 in finger abduction and grip power). Also, upper extremity deep tendon reflexes were exaggerated on the left side. The patient had received perioperative chemotherapy during the previous buttock surgery. The patient had no other relevant medical history.
Plain X-ray of the cervical region showed osteolytic destruction of the C7 vertebral body. Computed tomography (CT) and magnetic resonance (MR) imaging of the cervical spine showed the presence of a large, expansile mass, centered in the C7 vertebral body with extension into the left epidural and paraspinal space. Incidentally, a hypermetabolic lesion was also noted at the L1 by whole body PET-CT and a bone scan and a single small nodule was found in the right lung by whole body PET-CT and chest CT. A metastatic lesion was suspected, but she had no corresponding back or lung symptoms. A physical examination revealed 5/5 strength in all lower-extremity muscle groups, with intact sensation and no pain. Other investigations, including abdominal and pelvic CT scans, were normal.
A 47-year-old female who underwent C7 total spondylectomy due to a metastatic spine tumor. The patient complained of low back pain at 5 months postoperatively. 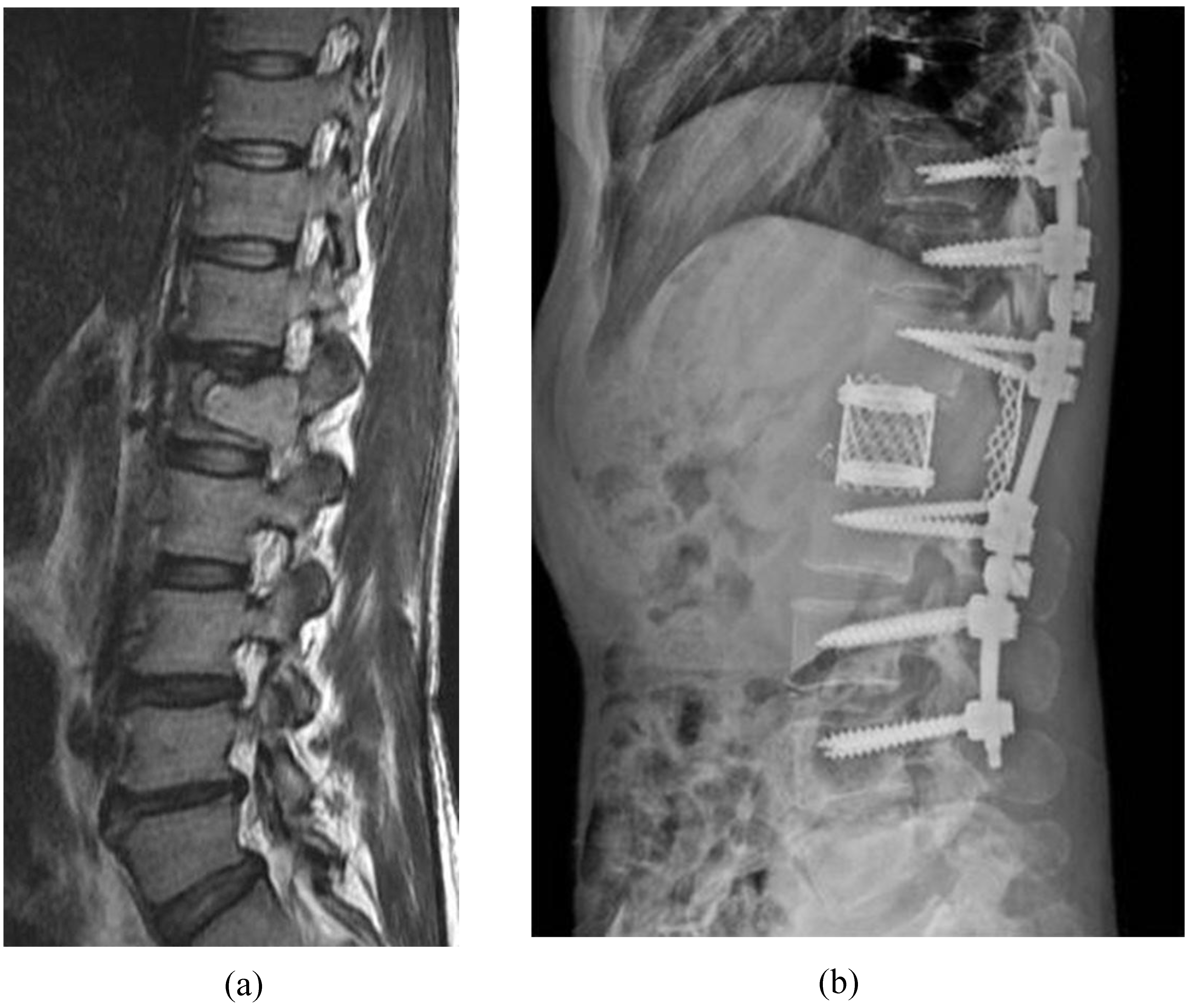
Total spondylectomy of the C7 tumor and stabilization with pedicle screws and cage were performed using an anterior and posterior approach (Fig. 1). At first, the posterior elements of C4-T3 were exposed subperiosteally, with dissection on both sides anterolaterally to expose the C7 nerve roots. The C7 lamina was removed in one piece by osteotomizing the bone at the junction between the lamina and lateral masses. The pedicles of the C7 vertebra were identified and pedicle screw fixation of C5, C6, T1 and T2 was performed. The C7 pedicles were transected, and each lateral mass was removed en bloc. The posterior tubercles were excised to prevent entrapment of the vertebral arteries during removal of the vertebral body during the anterior reconstruction. Posterior titanium mesh for spinal stability, scaffold of bone graft and protection of neural element and rods were applied to the spine, and autologous iliac bone grafts were used for the posterior fusion. For anterior surgery, the position was changed from prone to supine position. The C7 vertebral body was exposed anteriorly. The dissection was carried out to the tips of the anterior tubercles of the vertebra above and below, and the nerve roots were visualized and protected. Discectomies at C6-7 and C7-T1 were performed back to the posterior longitudinal ligament. There was special attention not to enter the subchondral bone of the C7 body. The vertebral arteries were dissected free of the C7 vertebral body and anterior tubercles. The body of the C7 vertebra was removed en bloc, and a titanium cage with autologous iliac bone graft was placed in the vertebrectomy defect between the C6 and T1 vertebrae. An anterior plate was fixed to C6 and T1. Operative time from skin incision to closure was 480 minutes, and the estimated blood loss was about 1200 cc.
After operation, symptoms progressively improved and motor strength below the elbow were increased to Grade 4. We had planned to operate for the L1 lesion after recovery of general condition. However, as there were no related symptoms with the lumbar lesion and the patient did not want to have more postoperative burden, she want to discharge and received adjuvant treatment at a hospital near her home. The patient received a total of 4 chemotherapy sessions and 10 radiotherapy (total 3000cGY) sessions to the C7 and L1 at a hospital near her home. However, 5 months later after the C7 surgery, she was transferred to our hospital with severe back pain and radiating pain of the right leg. CT and MR imaging of the lumbar spine showed the presence of a larger, more expansile mass than had been observed 5 months previously in the L1 vertebral body with extension into the epidural space. Neurological examination of the lower extremity was normal.
Histopathologic findings of the primary buttock lesion 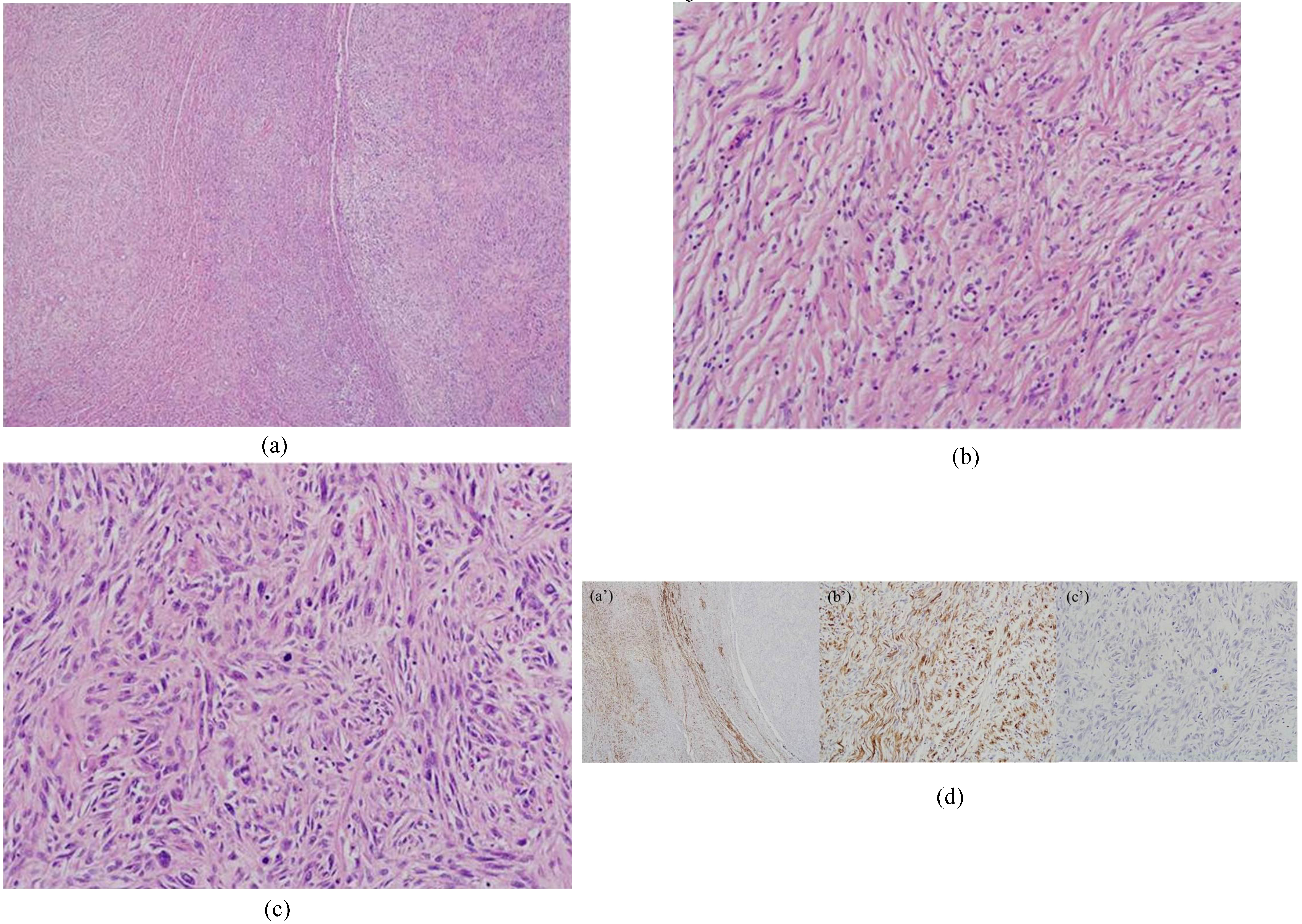
Total en bloc spondylectomy of the L1 tumor was performed using a single posterior approach (Fig. 2). After en bloc laminectomy of L1, segmental fixation 3 levels above and 3 levels below was performed. A temporary rod was applied and the blunt dissection was performed anteriorly on both sides through the plane between the tissue and the vertebral body. Then the segmental artery was dissected from the vertebral body and ligated. We mobilized the spinal cord from the surrounding venous plexus and the ligamentous tissue. Thread-wire saw cut the ventral column of the vertebra and the anterior and posterior longitudinal ligaments. The freed ventral column was rotated around the spinal cord and removed carefully to avoid injury to the spinal cord. After en bloc corpectomy, anterior reconstruction was done with a titanium mesh cage filled with iliac autograft and the two permanent rods were adjusted. Posterior titanium mesh was applied to the spine, and autologous iliac bone grafts were used for the posterior fusion. The operative time was 425 minutes with an estimated blood loss of about 1800 cc.
Histopathologic findings of primary 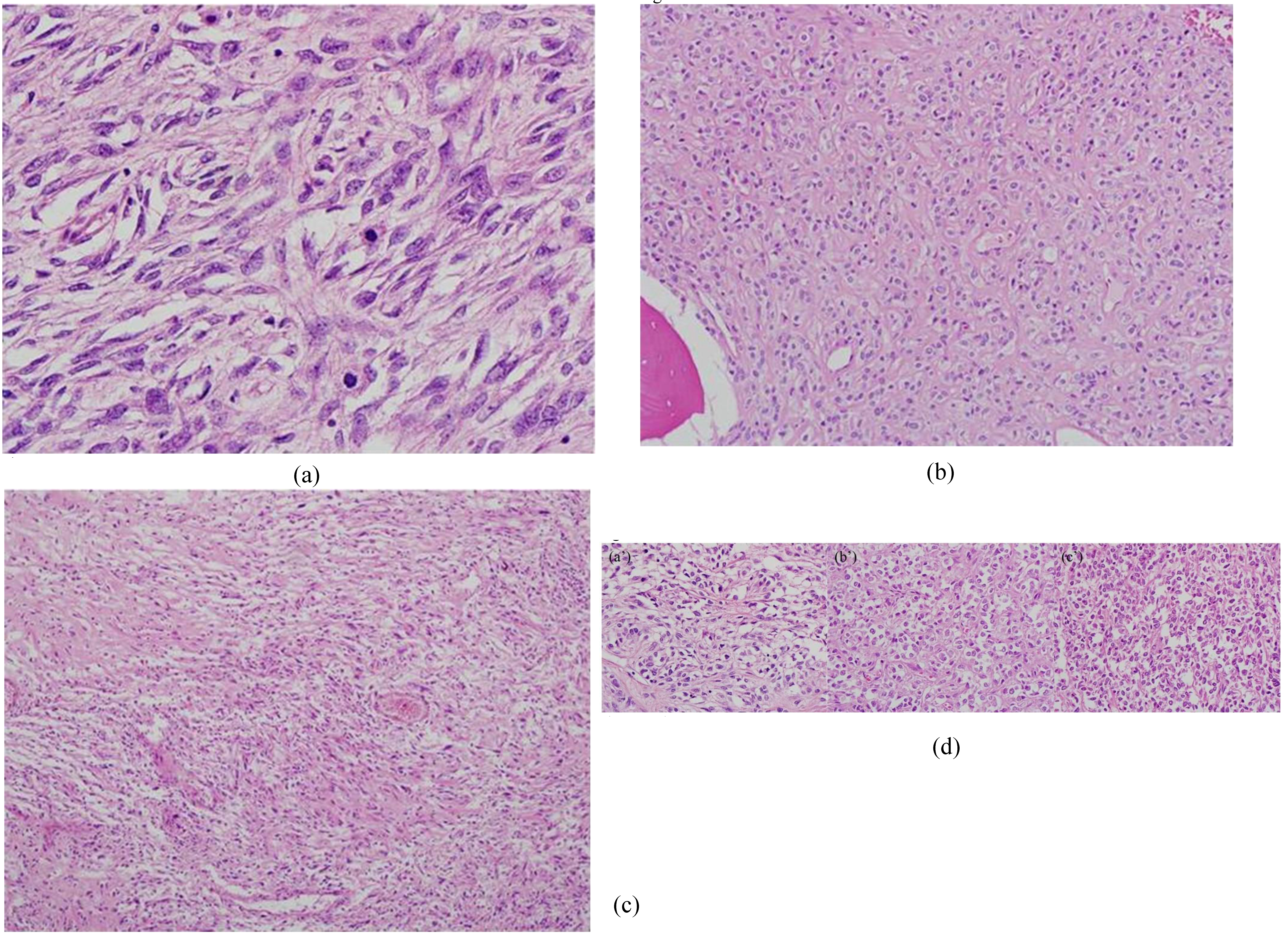
Postoperatively, back pain and right leg radiating pain showed good recovery and her neurology was normal. Ten days later, she was returned to the hospital near her home for adjuvant treatment. She received 2 times chemotherapy session. However, 6 months later (about 41 months after first buttock surgery), she died of septic shock with fever of an unknown origin, dyspnea and unstable vital signs. A retrospective review revealed no cutaneous markers suggesting neurofibromatosis and her family denied a familial history of neurofibromatosis.
Excised tissues were sent to our pathology department for histopathologic examination, and specimens of the right buttock obtained during the first surgery were re-examined at our hospital. Macroscopically, the right buttock mass was a relatively well circumscribed but non-encapsulated deep soft tissue mass. Most of the mass was tan in color and rubbery to firm in consistency, but its central region contained a small flesh-like area. For the secondary cervical and lumbar lesions, fragmented tissues had a ragged appearance and there were tan to gray in color and rubbery in consistency. Hemorrhage and necrosis were observed in the lumbar specimen. No macroscopic associations with a nerve were observed.
Microscopically, the right buttock lesion was a relatively demarcated soft tissue mass exclusively composed of spindle cells. The tumor cells showed low cellularity, had a uniform population with no nuclear atypia and rare mitoses, and contained wavy nuclei with variable collagenous stroma and rare mitotic figures, which was thought to be a benign neurogenic tumor. However, the central, well-demarcated, multinodular portion revealed atypical hyperchromatic spindle cells and somewhat epithelioid cells. Mitotic figures were quite numerous in the central area. No transition area was observed between the peripheral benign spindle cell portion and the central atypical portion. Immunohistochemically, the bland-looking spindle cells were strongly and diffusely positive for S-100 (1:1000; polyclonal antibody, Dako, Glostrup, Denmark) in contrast to the central area. They were not immunoreactive for the epithelial membrane antigen (EMA, 1:100; E29, Dako) and the neurofilament protein (1:2000; 2F11, Dako). A diagnosis of spindle cell sarcoma, high grade, most consistent with a malignant peripheral nerve sheath tumor arising in schwannoma was made based on the histomorphologic and immunohistochemical studies (Fig. 3). The cervical specimen revealed a vaguely alveolar growth pattern and was composed of mainly epithelioid cells with thin eosinophilic amorphous material, which should be differentiated from the osteoid. Neoplastic cells were immunoreactive for vimentin, but not for S-100, smooth muscle actin (1:200; 1A4, Dako), and TFE-3 (1:300; polyclonal antibody, Abcam, Cambridge, UK). Histomorphologic features of the cervical lesion were similar to those of epithelioid cells in the central area of the buttock mass. The lumbar specimen showed extensive coagulative necrosis and hemorrhage, which were considered post-therapeutic effects. The tumor cells were composed of mainly hyperchromatic spindle cells and peripheral epithelioid cells. Prominent vascular ectatic change was also noted. This feature and the hyperchromatic pleomorphic spindle cells observed in the central portion of the buttock specimen looked morphologically similar. Based on the overlapping morphologic features between the primary buttock mass and the cervical or lumbar lesion, we concluded that two spine lesions were secondary metastatic foci (Fig. 4). However, it took about 7 months to make this pathological result and it was the result of discussion between eminent domestic and international pathologists based on analysis and study of the three specimens (right buttock, cervical and lumbar spine).
Discussion
MPNSTs are rare malignant tumors of peripheral nerve sheath origin and occur in 0.001% of the general population, and have one of the poorest prognoses of all soft tissue sarcomas. MPNSTs are usually found on the peripheral nerves located in the trunk and extremities [8]. The diagnosis of MPNST is difficult and due to its rarity, little information is available regarding its prognostic factors or its long-term outcome. The clinical characteristics of intraosseous MPNSTs differ from those of their soft tissue counterparts. In particular, they have a wider age distribution, and are not usually associated with NF-1; they also behave more aggressively [9]. Intraosseous MPNSTs are largely confined to the mandible or maxilla and occasionally occur in the long bones of limbs [10, 11]. The spine is a rare site for intraosseous MPNSTs, and thus, the clinical features and outcomes of spinal MPNSTs remain unclear. The image findings of spinal MPNSTs are non-specific and can mimic metastatic secondaries to the vertebrae. MPNSTs typically produce lytic bony lesions that are enhanced by contrast in CT and MR images [5, 11]. Accordingly, their diagnosis usually require adequate tissue biopsy.
The gold standard treatment for spinal MPNSTs also has not been established due to its rarity and a lack of prospective trials. Complete surgical removal with negative tumor margins remains the most effective treatment and the most significant prognostic factor for MPNSTs. The effectiveness of surgery is dependent on performing radical resection before tumor metastasis [12, 13, 14, 15]. Adjuvant radiation therapy improves the local control of this disease [2, 12], but the benefits of chemotherapy remain unclear
Despite aggressive local excision followed by radiotherapy and chemotherapy, MPNSTs tend to recur at their original site and metastasize to lung, liver, lymph nodes, and bones. Thus, MPNST is highly aggressive and survival from it is poor. Review of the literature confirmed eventual recurrence in 75% of cases and a 5-year survival ranging from 16% to 53% [2, 5, 14, 16]. The poorer outcome for spinal MPNSTs is probably due to the surgical challenges posed by its anatomical location and the high vascular supply to the spinal canal favoring systemic spread. In our case, having a first such patient admitted to our hospital, we were not able to initially make an accurate pathologic diagnosis. It was suspected to be a metastatic lesion as the patient had an operation history of right buttock spindle cell sarcoma at another hospital about 30 months previously and C7, L1 lesions and a solitary lung nodule were found. We performed anterior and posterior surgery for the only C7 lesion due to the patient’s strong will for complete recovery of C7 lesion, her relatively young age of 47 years, follow up period without any problems after first buttock surgery and the small L1 and lung lesion with no related symptoms. The final pathologic diagnosis was made after 7 months because our case was extremely rare and then we found that the prognosis was very poor.
The pathological diagnosis of MPNSTs can be difficult due to the lack of specific morphological, immunohistochemical, and molecular criteria. Grossly, the tumors may be within or attached to a nerve trunk. The lack of a single immunohistochemical marker for nerve sheath tumors complicates the diagnosis when the tumor is not associated with a nerve or arises in a patient not having NF-1. Currently, S-100 protein staining is the most widely accepted means of demonstrating neural differentiation. Most MPNSTs occur in patients with neurofibroma, especially in patients with NF-1, but rarely, they arise due to malignant degeneration of schwannoma. Therefore, MPNST arising in schwannoma is quite rare [6, 17, 18]. Woodruff et al. [19] proposed the following diagnostic criteria for the malignant transformation of schwannoma: (a) having histologic and immunohistochemical features of a classical or cellular schwannoma containing a population of malignant cells; (b) presence of cells that should have metastasized or have the same histologic characteristics as metastatic components of reported malignant peripheral nerve tumor; and (c) there being no evidence of a primary tumor that might had metastasized to the schwannoma. Our case met all three of these criteria.
Unlike MPNSTs arising from neurofibroma, most sarcomas arising in schwannoma, such as epithelioid MPNST and epithelioid angiosarcoma, have an epithelioid morphology [7, 19, 20, 21]. This described case is unique because it presented a mainly spindle cell morphology with some epithelioid features. To the best of our knowledge, spindle cell type MPNST arising in soft tissue schwannoma with multiple intraosseous spinal metastasis has not been previously reported. It is important for pathologists and surgeons to recognize that spindle cell type MPNST may arise in schwannoma, as this condition might be misdiagnosed as cellular schwannoma and the prognosis of spindle cell type MPNST is very poor.
Conclusion
Spindle cell type malignant peripheral nerve sheath tumor arising in benign schwannoma is an extremely rare disease entity that exhibits aggressive progression and poor prognosis. The morphology and immunohistochemical expression profiles of our case were different from those of the reported cases. It is important that pathologists and surgeons recognize spindle cell type MPNST may arise in benign schwannoma, because this recognition aid the assessment of patients with schwannoma and contribute to the pathologist making a more precise diagnosis and the surgeon in determining the proper therapeutic options, including surgical methods.
Conflict of interest
None to report.
Footnotes
Acknowledgments
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2016R1D1A1A02937348).