
Abstract
PURPOSE:
There are limited studies related to the rehabilitation of neglected Monteggia fracture-dislocations. This study reports the results of the rehabilitation of neglected Monteggia fractures and dislocations and the best treatment options available.
MATERIAL AND METHODS:
Thirteen children were rehabilitated between 2009 and 2012. A retrospective chart review was conducted to record the following: age, gender, anatomic region of fractures, time delay from symptom onset to fracture, Bado classification, Mayo Elbow Performance Index (MEPI) which includes pain, range of motion and daily life comfort, surgeries, length of hospitalization, location and pattern of fracture, length of follow-up and complications.
RESULTS:
The study group included thirteen children and adolescents; eleven males and two females with a mean age of 8.5 (range 2–15) years. According to the Bado classification, 11 patients had type 1, one had type 3 and one had type 4 fracture-dislocations. For Mayo Elbow Performance Index (MEPI) scales, patients that were less than ten years old had greater mean scores. Two patients had superficial infection, one had subluxation, one had osteoarthritis, one had delayed bone union and two had rigidity at the elbow.
CONCLUSION:
The goals of elbow rehabilitation following Neglected Monteggia cases include restoring function by restoring motion and muscle performance; influencing scar remodeling and preventing joint contracture; and restoring or maintaining joint stability. Patients aged younger than 10 years and intervals of less than one-year, between trauma and diagnosis, as well as early and effective rehabilitation were found as important parameters regarding favorable outcomes.
Introduction
Monteggia fracture is defined as fracture of the proximal third of the ulna and the anterior dislocation of the head of the radius together with disconnection from both radiocapitellar and radioulnar joints [1]. Most patients respond to conservative treatment performed at the early stage. However, neglected cases with Monteggia fractures that could not be diagnosed in the first examination have a quite high possibility of recurring within a couple of months or later with complaints of pain, weakness, limited range of motion, deformity and nerve injury at elbow (involvement of ulnar and posterior interosseus nerves) [2, 3, 4]. The most common and current approach for surgical treatment is open reduction of the radial head, open wedge osteotomy to ulna and/or ligamentoplasty [5]. There is no common consensus on the type of osteotomy or ligamentoplasty to be performed in Monteggia fracture-dislocations. In addition, there are very few studies related to the rehabilitation of neglected Monteggia fracture-dislocations. In this paper, we report medium and long-term results of rehabilitation in our cases with Monteggia fracture-dislocation which is a rare entity.
Preop and postop images of Bado type 1 case.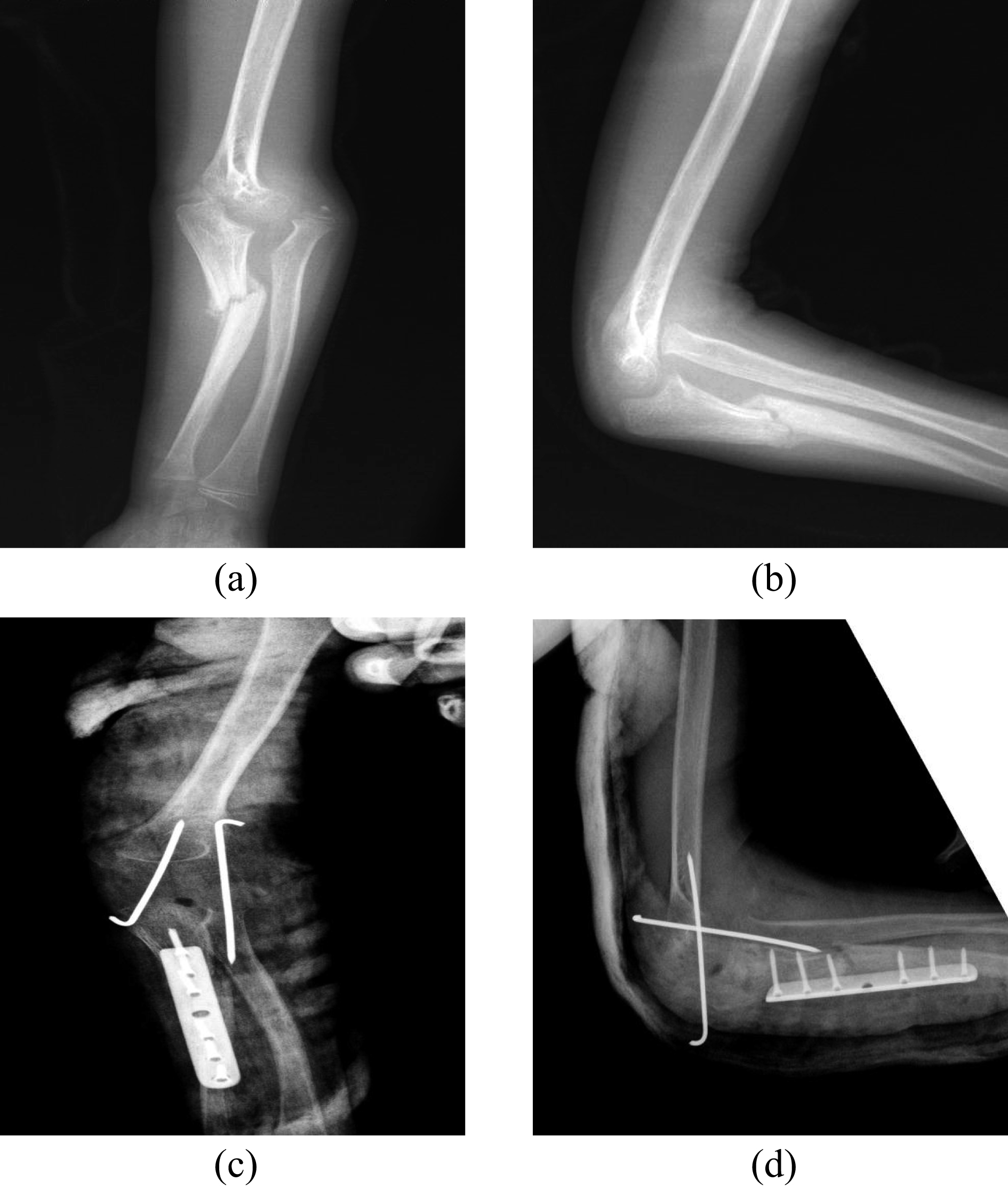
The study included 13 cases with Monteggia frac- ture-dislocation that underwent operation and foll-owed-up from 2009 to 2012 after obtaining informed consent. The ages of the patients varied between 2 to 15 years with a mean age of 8.5 years. There were 11 male and 2 female patients. The reason for the complaints at the elbow and forearm of the patients was due to fall from height in 4 patients, a simple fall in 4 patients, a fall off from an animal in 3 patients and birth trauma in 2 patients. None of the patients were taken to a health center at the initial injury. They were taken to bonesetters and their arms were bandaged with traditional methods. The mean interval between trauma and diagnosis was 8.84 months (range: 3–24 months). The affected elbow was on the right side in 5 patients and on the left side in 8 patients. Diagnosis was made by taking anteroposterior and lateral radiograms of the elbow and patients were categorized according to the Bado classification. According to the classification introduced by Bado [1]: there is an anterior dislocation in type 1 and 4 (accompanied by radial diaphysis fracture) injury; there is a posterior dislocation in type 2 injury and there is an anterolateral dislocation in type 3 injury depending on the orientation of dislocation of the radial head. No advanced examinations such as computer tomography or Magnetic rezonans were performed in any patient. Eleven patients had type 1, one patient had a type 3, one patient had type 4 fracture-dislocations and none of our patients had type 2 injuries. All patients were operated under general anesthesia by minimizing the anesthesia risks. The Boyd posterolateral approach was preferred for surgery [6]. In all patients, ulnar osteotomy was performed first to provide length (Figs 1–4). Ligamentoplasty was performed in all patients and when applicable, annular ligament was repaired. The ulna was stabilized with plaques screws in 9 patients, intramedullary K-wires (TEN) in 4 patients and transcapitellar K wire applied in six patients. No case required radial osteotomy and a long arm splint was applied to all patients postoperatively while keeping the forearm in the neutral position.
Preop and postop images of the Bado type 1 case where proximal metaphyseal osteotomy was performed.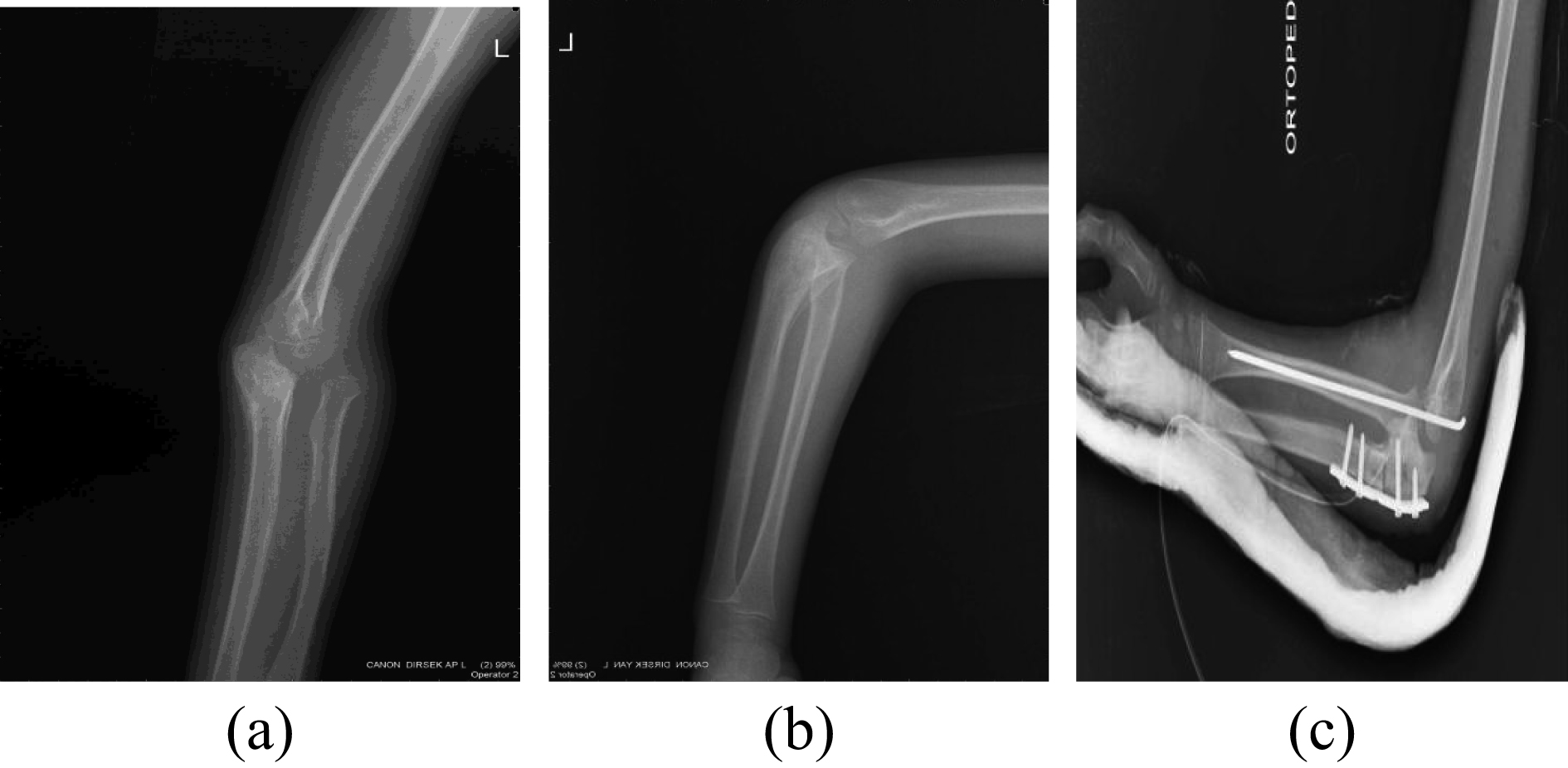
Pre- and post-operative images of proximal ulnar diaphysis fracture and radial head anterior dislocation.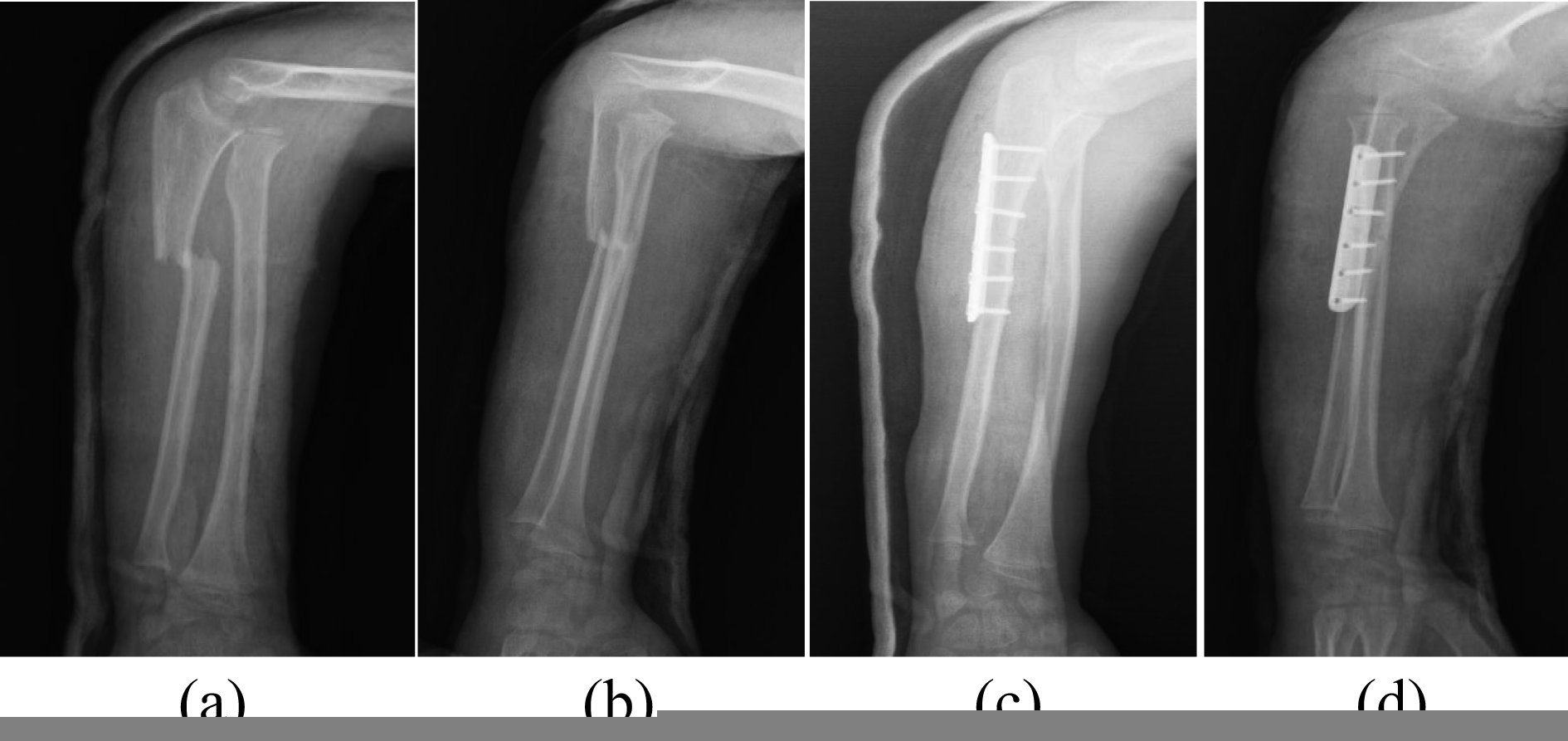
Preop and postop images of the Bado type 1 case where proximal metaphyseal osteotomy was performed.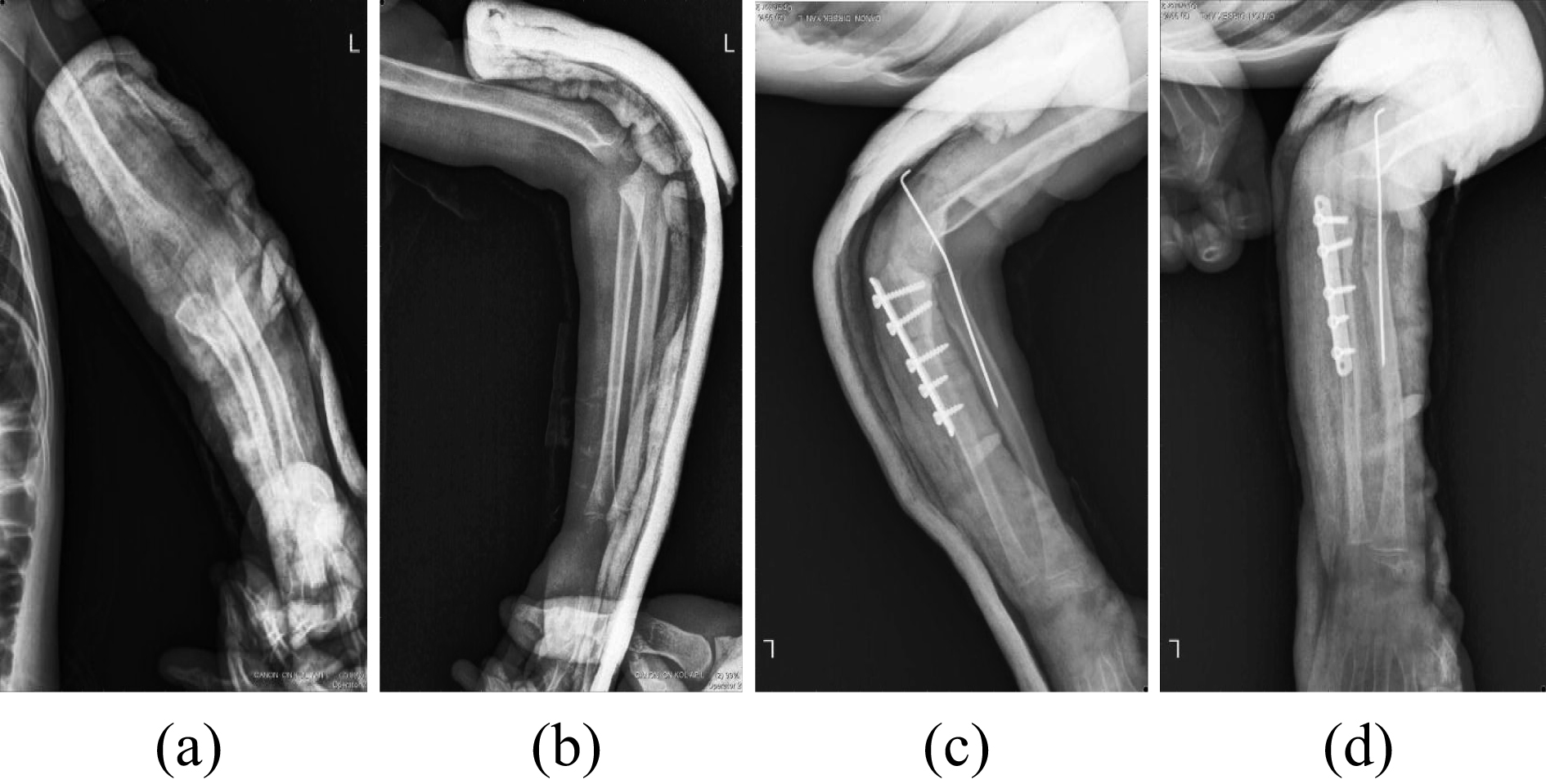
Due to being neglected, our patients experienced minor muscle atrophy around the elbow and developed a limitation in the range of motion of the joint. Therefore, early and effective rehabilitation was mandatory. Early rehabilitation was initiated soon after surgical operation and the rehabilitation program was as described below.
Week 1–3
Controlled active and passive exercises were performed along the range of motion (ROM) while a long-arm splint was put in place. Active assisted ROM exercises were performed on the shoulder, deltoids, biceps, and triceps muscles covered with the splint were trained with isometric exercises.
Week 4–6
A long-arm splint was replaced with a functional arm brace. Controlled active-passive ROM exercises and shoulder active assisted ROM exercises were continued. In addition, active ROM exercises were started gently on the elbow (with supination and pronation of elbow) while removing the brace three times a day. Ball-squeezing exercises were started for the hand.
Week 8–12
Immobilization of the elbow joint was terminated. Fully active partially resistant exercises were applied for all movements of the elbow with particular emphasis on the supination and pronation. Squeezing force was increased using ball-squeezing exercises. Body weight was gradually transferred to the elbow joint [7]. Patients were followed-up based on Mayo Elbow Performance Index (MEPI) which includes pain, range of motion and daily life comfort [8]. The radial head, osteoarthritic changes, radial frontal neck angle and radial head hypertrophy were monitored according to the criteria described by Kim et al. [9]. Routine lateral and AP radiograms of the elbow were used to evaluate radial head deformity, osteoarthritic changes and subluxation and/or luxation of radial head during follow-up. Radiological findings were noted as good (complete reduction of elbow without osteoarthritis), moderate (osteoarthritis of the elbow and resistant subluxation) and poor (complete dislocation of the radial head).
Details of preoperative and postoperative findings
Details of preoperative and postoperative findings
Univariate and multivariate analysis of variance at each ROM and MEPI scales
Data were analyzed using R version 3.1.1. and multiple statistical analyses were conducted. First, two-way multivariate analysis of variance (Manova) between patients designed with the independent variables of 2 (treatment group)
Results
Patients age, gender, Bado type, fracture type, interval time, osteosyntesis type, mean follow up and complications were summarized in Table 1. Patients were followed up for 1.5–4.5 (2.9) years on average. At the last follow-up, all patients were rated according to the Mayo Elbow Performance Index (MEPI) [8] criterion. One patient had an osteochondral lesion. Radiological signs of bone union began to appear at 6
Pairwise t tests for ROM scales
Pairwise t tests for ROM scales
Pairwise t tests for MEPI scales
If the treatment of this disease is delayed, the natural course becomes worse. It can lead to progressive valgus deformity, instability, and decreased range of motion. Surgery was advised to achieve anatomic reduction of radial head, prevent progressive valgus instability and improve cosmetic appearance and range of motion. Currently, many authors recommend surgical intervention if: 1) the diagnosis is made early; 2) there is limited range of motion, weakness, progressing deformity, normal concave radial head, convex and capitellum 3) the family and the patient are aware of the benefits of reconstruction procedure. Very few case series related to surgical outcomes of neglected Monteggia fractures include more than 10 patients [10, 11, 12, 13, 14]. Currently the most debated topics in delayed cases with Monteggia fractures are the appropriate age to perform surgery, type of ligamentoplasty interval between the time of trauma and surgery and the type of osteotomy to be performed.
According to by Nakamura et al. [15], favorable outcomes can be expected in the long term in delayed cases, if the patient presents before 12 years of age and within 3 years after the trauma. We also observed that outcomes were worse with increasing age and interval. In chronic cases with Monteggia fractures, we were able to achieve less painful and more functional elbows with appropriate surgery and early rehabilitation, if the interval was shorter than 12 months and patients were younger than 10 years old. Nakamura et al. [15], starting in 1997, used forearm fascia followed by remnant annular ligament by augmenting them with free tendon grafts. They reported their outcomes were better. Delpont et al. [16] performed ligamentoplasty to one group of patients, and did not perform it in the other group. They reported that the group that had ligament repair had better outcomes compared to those without repair. If not all, most authors suggest a combined approach of ligament repair together with osteotomy. We performed ligament repair in all our patients and observed a great benefit from this approach. According to the generally accepted view, the major problem is the poor bone union in the ulna that prevents reduction of the head of radius. According to some authors [17], ligament repair is not necessary [15]. If the head of radius does not fit into place after angulation distraction osteotomy, then there must either be a pseudocapsule preventing reduction of the radial head or the remnant annular ligament must be stuck between the joint. For that reason, some authors performed arthrography and made excision under arthrographic guidance when the head of radius did not fit into place with closed reduction. According to the authors, additional surgical procedures would increase rigidity, avascular necrosis, heterotopic ossification and radioulnar synostosis [17]. In one study, the authors detected annular ligaments that were stuck in the joint space and repaired 5 of them [18]. In one study, they repaired an overturned annular ligament in 2 patients [19]. In another study, the authors approved of the late repair of the annular ligament for better functioning and less pain in the long-term [20]. Nevertheless, some authors preferred elongation with the use of an external fixator and correction of the angulation. They did not perform open reduction in any patients and reported their results as satisfactory [21]. Gyr et al. [20] used annular ligament reconstruction (ALR) in 15 patients. Considerable loss of range of motion was observed at follow-up in both flexion-extension and supination-pronation planes. We performed remnant ligament in 6 patients and using triceps in 7 patients for ligamentoplasty and could not find any significant difference between the ROMs of these patients. In our opinion, annular ligament is statically and dynamically the main stabilizer of the radial head and we believe that it is a more reasonable and more biological option for elbow restoration. In our study, ligament reconstruction was made after osteotomy and we performed ligament repair in all of our patients. We did not detect prevention of the rotational movements of the radial head due to ligament repair. Therefore, we approve of ligament repair in terms of elbow biomechanics and think the external fixator applications may be troublesome and frequently lead to failure.
There is no consensus on the best approach to fixation of osteotomy stabilization. Rather than the type of fixation, a good ulnar fixation is the key to maintain the stability of radial head. In our study, we repaired annular ligament using tricipitate graft or remnant ligament in all patients following ulnar osteotomy using Boyd [6] incision. Since eleven of our patients had their fractures at diaphysis region, angulation distraction osteotomy was performed in these patients. Metaphysial osteotomy was performed in the remaining patients. For children aged 10 years or older, rigid osteosynthesis was performed using plaque screw regardless of the type of fracture.
Internal fixation and ligametoplasty are a safe me- thod for missed monteggia fracture- dislocations in children and adolescents, which allows postoperative rehabilitation with the advantage of early elbow and forearm mobilization. Postoperative rehabilitation has the advantage of early mobilization in children [22]. The most common complication of elbow fractures and dislocations is the elbow flexion contracture. The exact pathology of elbow contracture is unclear. Reported reasons for loss of motion include prolonged immobilization, soft tissue trauma, intra-articular trauma and heterotopic bone formation [23]. Treatment should be coordinated for the involved tissues through the progressive stages of healing without damaging the healing soft tissues. The therapist must focus on minimizing joint stiffness and muscle atrophy to maximize functional outcome without losing fracture reduction or joint stability, and must be attentive to potential complications and, when possible, minimize or prevent them. These complications include ankylosis, instability, nerve injury and ectopic ossification [24, 25, 26, 27]. Early protected motion of the elbow minimizes joint stiffness and facilitates healing. According to Goyal et al., another area that needs further study is radial head morphometry in neglected dislocations. Future computed tomographic or magnetic resonance imaging-based evaluation of radial head shape with measurements of size may be useful [28]. As previously stated, joint stiffness is common with elbow fractures, and immobilization longer than 3 weeks may result in significant loss of motion. We think that it might be useful to work with radial head morphology that may require further investigation; however, we have not studied this issue in our study and have not used advanced imaging systems. In our study, rehabilitation results of patients younger than 10 years old were more satisfactory than those of patients older than 10 years old. While we observed four complications among patients older than 10 years old, we only saw one complication among patients younger than 10 years old. Similar to previous reports, two patients had rigidity at their elbow. We think the reason for fewer complication rates in our hands was related to the higher proportion of patients in our study group that were younger than 10 years old with intervals less than 1-year. Physiatrists and surgeons need to work together to provide evidence to support the rehabilitation needed and to determine the most effective plan of care to enhance patient outcomes. Communication among the patient, therapist, physiatrists and surgeon is essential for the rehabilitation program to develop the appropriate plan of care throughout each phase of healing. Rehabilitation after elbow fracture and dislocation is challenging for the therapist, since the elbow is prone to joint stiffness and contracture. The therapist must consider the timing and progression of therapy during the physiologic phases of tissue healing.
This study has a few limitations. It is retrospective and comprises a relatively small number of patients. Therefore, more studies are necessary to validate our findings.
Conclusion
We believe that ulnar restoration and annular ligament reconstruction is a more reasonable and biological option that leads to increased performance by enhancing and restoring elbow biomechanics. Early diagnosis, an interval of less than 1-year between the time of trauma and diagnosis and patient age younger than 10 years are considered as the most important factors in terms of the rehabilitation outcome. Initiating rehabilitation as soon as possible in the presence of sufficiently stable fixation may yield quite satisfactory results.
Conflict of interest
The authors declare that there is no conflict of interest.
Footnotes
Acknowledgments
Thanks to Hospital committee for their contribution in sharing data.