
Abstract
BACKGROUND:
The prevalence of chronic back pain poses major challenges for all health care systems and patients worldwide. Myofascial trigger therapy (MT), although a very popular standard non-pharmaceutical form of treatment, only shows small to medium effectiveness.
OBJECTIVE:
To test a new vibrotreatment (Cellconnect Impulse) transmitting low-frequency, vertical shock waves in a routine clinical practice.
METHODS:
Eligible patients were adults seeking physiotherapeutic treatment. They were randomly allocated to either six treatments of MT or to six treatments of combined MT and vibrotreatment. Outcome parameters were pain intensity, pain days, pain duration, and quality of life.
RESULTS:
The pain relieving effects of the combined treatment were very large (
CONCLUSIONS:
Combining MT with Cellconnect Impulse enhances the physiotherapeutic effectiveness of treating chronic back pain.
Keywords
Introduction
Although the prevalence of both non-specific and specific chronic back pain is high, robust epidemiological estimates are difficult to obtain. Consequently, may practitioners struggle with applying (cost) effective treatment. Part of the problem is the fact that chronic back pain comprises different classes of causes, symptoms and locations. For instance, chronic neuropathic pain (CNP), a sub-class of chronic pain affecting the somatosensory system, has recently been rated to impair 7–10 percent of the general population [1]. According to another recent meta-analysis of chronic widespread pain (CWP), the random effects pooled estimate was close to 12 percent, but the effects showed considerable heterogeneity [2]. In a recent systematic review of low back pain (LBP), the highest rate (20 percent) was found in the population of 30 to 59 year olds [3]. The prevalence of chronic back pain (CBP) in Germany, for example, is among the highest in the world. In several regional and national surveys, rates of up to 50 percent were reported with only about 20 percent of the population never having experienced any back pain at all [4]. Clearly, chronic back pain poses a major challenge for the health care system. When treated unsuccessfully, it causes continuous substantial socioeconomic burden and significantly reduces the health related quality of life of the individuals affected.
There are three ways to treat back pain: non-pharmaceutical, pharmaceutical, and surgical (invasive) therapies. From the various forms of non-phar- maceutical therapies (e.g., kinesiotherapy, massage therapy, or thermo therapy), manual therapies are among the more effective ones, both short term and long term, but the effects are only small to moderate in size [5]. Among the various forms of manual therapy, many health care professionals favor myofascial trigger point therapy [6]. However, although most practitioners agree on the notion that myofascial knots constitute an identifiable source of musculoskeletal pain, there has been a debate regarding the claim that such hyperirritable, taut nodules in the fasciae surrounding the muscle may be used as triggers to mitigate chronic pain. The main argument concerns the ambiguity of the exact diagnosis and the lack of sufficient explanation of the functional mechanisms of trigger points [6, 7]. There is, however, empirical evidence showing that myofascial trigger point therapy does indeed effectively relieve pain in, for instance, patients with spinal pain disorders [8]. Likewise, a RCT involving comprehensive treatment of muscle trigger points for a period of 12 weeks effectively reduced shoulder pain symptoms and joint functions [9]. Moreover, there is a number of imaging studies detecting and quantifying neuronal patterns underlying taut bands in patients with myofascial pain [10, 11, 12].
The assessment of the effectiveness of myofascial trigger point therapy, however, is rendered difficult due to different existing forms. Varying from deep pressure (myotherapy), acupressure, or tapotement, to ultrasound, electrostimulation or dry-needling, to name but a few, trigger point therapy constitutes a rather heterogeneous class of treatment. On the other hand there is less controversy with regard to the principle of causation. It is assumed that trigger points provoke specific biochemical imbalances (e.g. depolarized muscle fibers putting a strain on ligaments, tendons, and joints) which in turn generate sustained compression of local blood supply and depletion of energy and consequently cause nociceptive pain nerves to fire [13]. Everyday practice experience shows that patients undergoing trigger point therapy usually report an immediate release of pain after the first treatment. This immediate effect may, however, fade. In some patients the effects prevail or even increase, other patients don’t experience a significant decrease in pain at all.
In past years, new methods have been developed to treat chronic pain involving physical stimulation with devices applying frequencies, vibrational impulses and waves. For example, in a recent study with LBP patients the effects of extracorporeal shock waves (ESW) were larger than those of conservative physical therapy. The effects, however, were largest when EST was combined with an exercise program [14]. Yet, the body of evidence regarding the effectiveness of such techniques is still inconclusive. For instance, in a meta-analysis comparing various forms of treatment for LBP vibrotreatment was not superior to traditional therapies or placebo [15]. Apart from this empirical inconclusiveness, there is yet another more practical limitation of such techniques. Most devices, which typically use high and low energetic radial impulses, only apply energy locally (a radial impulse is parallel to the radius vector). This is why they are confined to relatively small areas of the body (e.g., elbow, shoulder, or heel). Also, high-energetic radial impulses may be contraindicated in patient suffering from specific back conditions sensitive to strong physical impacts.
To circumvent these problems and to make full use of the potential benefits of impulse waves in physiotherapy, a new therapy table has recently been developed transmitting integrated, vertical, low-frequency impulses through the body (Cellconnect Impulse; Pa- tent No’s: EP 16 000 704.3, EP 12 783 861.3, DE 10 2015 003 854.0, DE 10 2011 117 680.6). The table is software-controlled (via a tablet) and allows different basic settings for various therapy programs in the range of 10 Hz and 55 Hz, as well as individual programming. Due to the novelty of the device there is no empirical body of evidence regarding its exact functional mechanisms and its therapeutic effectiveness. However, one major difference with regard to similar devices is its conceptual design. The application of mild microvibrations is thought to disperse through bodily fluids and cells thereby altering cell function and cell metabolism (e.g., nutrient transport, detoxification, regeneration). Most importantly, this therapy form was primarily designed to complement existing therapy forms (e.g. MT) to render them more effective. Practical therapeutic experience shows that patients treated with Cellconnect Impulse frequently report strong pain relieving effects when being treated in conjunction with e.g., thermo therapy or MT. Also, in patients suffering from chronic pain, practical physiotherapeutic experience shows that trigger points are released faster and less painfully. Obviously, there appear to be synergistic therapeutic effects when Cellconnect Impulse is used as an adjuvant in the clinical practice.
Flow diagram of randomized and analyzed patients.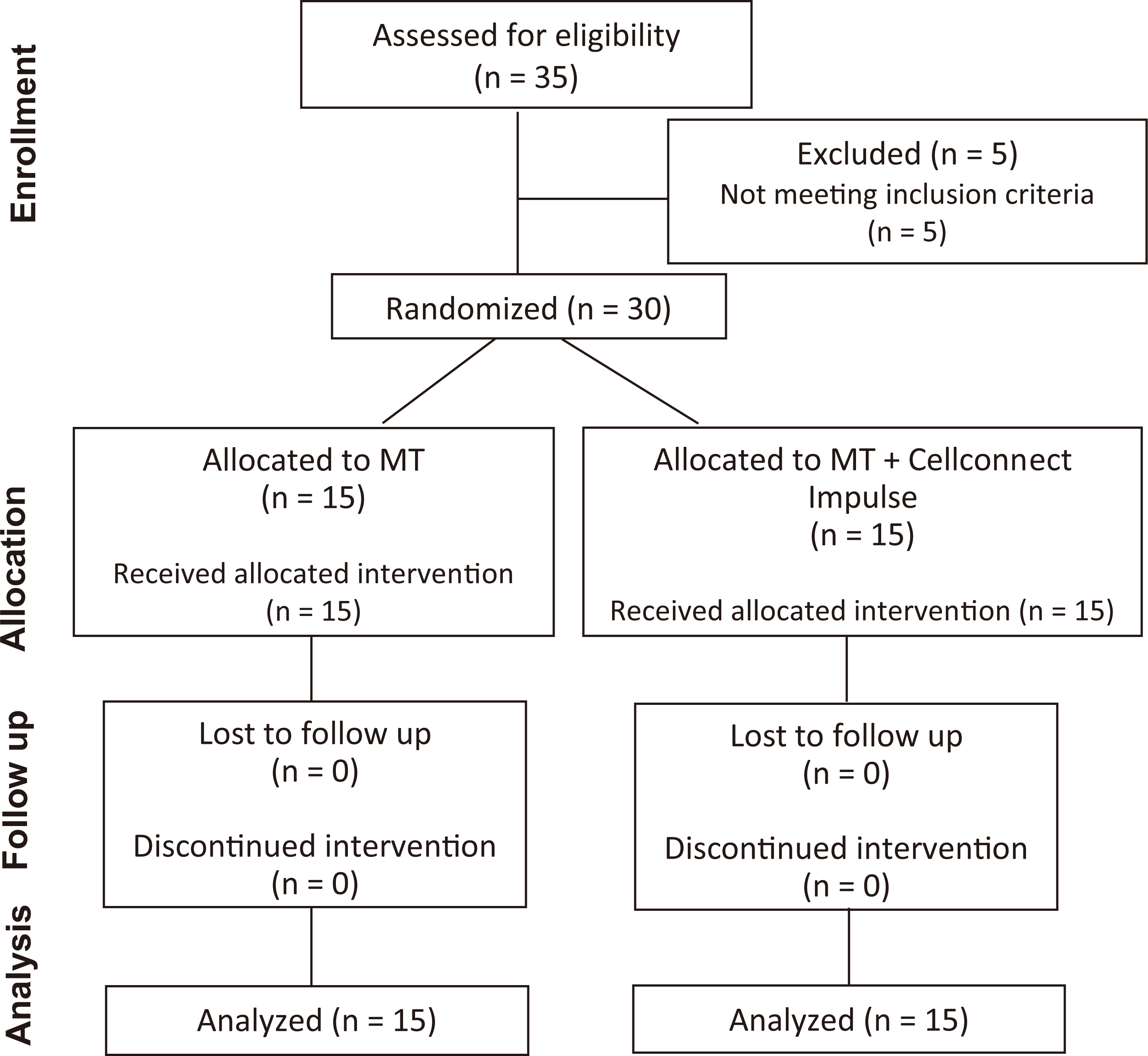
To test this assumption, a pragmatic trial was run with chronic pain patients. Specifically, the effectiveness of this new therapy form was gauged in patients suffering from chronic back pain. The purpose was to determine the clinical relevance of the statistical effects. To do so, Cellconnect Impulse was used in the spectrum of a routine clinical practice. Due to the nature and main purpose of this therapy form, it was compared as an add-on intervention against an established therapy form (i.e. manual myofascial trigger therapy). The main hypothesis was that chronic pain patients would show greater pain relief when treated with the combined intervention.
Sample
Patients were recruited from the pool of RECON and via advertisements addressing chronic back pain. A total of thirty-five patients were enrolled in the study (cf. Fig. 1), thirty of which were eligible for participation (eighteen women). Twenty-five patients had a recorded medical history of chronic back pain and had undergone numerous previous medical and physiotherapeutic treatments (e.g., surgery on spinal discs, malalignment, muscular imbalances). Other than chronic back pain, which had to exist for at least three months, inclusion in the study required legal age and the absence of major diseases (e.g. cardiovascular diseases, diabetes, acute infections or injuries), drug addiction, mental illness or pregnancy. The mean age of the sample was 43.2 years (range: 23–65 yrs). On average, patients suffered from chronic back pain for 56.4 months. Table 1 provides an overview of pain symptoms for the patients of either treatment condition. All participants provided written informed consent, and the study was run according to the Ethical Principles for Medical Research Involving Human Subjects (World Medical Association, 2013) and the CONSORT for Pragmatic Trials [16]. All 30 patients completed the trial and none complained about adverse effects.
Dependent variables
Questionnaires
Chronic pain. All pain indices were adopted from similar studies investigating pain symptoms [17, 18]. The item format and content was chosen in accordance with commonly used response formats and recommendations in pain research [19, 20].
Pain intensity. Pain intensity was measured with a 7-point-Likert-Scale with the anchors no pain, very low, low, moderate, strong, very strong, and unbearable. Pain intensity was the primary outcome variable.
Pain duration. An open item assessed the hours pain typically lasted on pain days.
Number of pain days. An open item assessed the number of days pain typically occurred per week.
Health related quality of life. The questionnaire “Quality of Life with Chronic Disease” (German: “Pr- ofil der Lebensqualität chronisch Kranker” [PLC]) [21] measures the quality of life experienced by patients with chronic diseases on the physical, emotional and social levels, making allowance for subjective state of health and action abilities. The PLC offers valid and reliable indicators of the degree of restriction or disability experienced by patients. Its administration renders practical results in the clinical and therapeutic realm, especially when symptoms are assessed over the course of time. The main module differentiates between six basic dimensions from which the first four were considered in the present study: physical performance, the ability to enjoy and relax, positive mood, negative mood, the ability to communicate, and the sense of belonging. Each item consists of a 5-point-Likert-Scale with the anchors very bad, bad, moderate, good, and very good.
Pain characteristics of study sample
Pain characteristics of study sample
Manual myofascial trigger therapy (MT). This treatment involved palpation of the target musculature, identification of the trigger points, and provocation of the taut muscle fasciae. For each patient, several trigger points were treated. Taut nodules were manually compressed until the muscle tone was reduced. By continuously increasing pressure pain reactions were produced. The treatment was stopped once the reduction of tension was exhausted. Patients were treated for thirty minutes per session.
Cellconnect Impulse (add-on). Patients undergoing this treatment received the same MT described above. In addition, they were placed on an adjustable, full body table (204
Study design and procedure
The study was a two-armed, measurement repeated, randomized, controlled pragmatic trial. The random allocation sequence was generated by RECON using the software package SPSS 17. The balanced random allocation sequence was implemented by a patient sequence list accessed by the therapists before each session.
Treatment was performed by a female and a male physiotherapist. Both treated 15 patients each, and were randomly assigned to them. Both therapists had a professional experience of at least 25 years. To test the effectiveness of the interventions under routine practice conditions, patients were treated in accordance with German medical health care and prescription regulations. Hence, they received six treatments of 30 minutes each. In the initial session, the physiotherapist introduced the nature and purpose of the study. After patients gave their informed consent, baseline measures were taken. Then, participants were informed about the type of treatment they received according to the randomization protocol. Finally, the first treatment was applied. The therapeutic intervention comprised two treatments per week, totaling three weeks per patient. Upon the last treatment, post-treatment measures were taken to determine the therapeutic effectiveness.
Data analysis
In alignment with meta-analytical practice [22], and to avoid pseudo evidence associated with the use of NHST, effect sizes and confidence intervals were calculated.1
Despite the widespread use of so called null hypothesis significance testing (NHST), methodologists have harshly criticized and protested its use since the 1930s (for a recent and thorough overview, cf. [25, 26]). For instance, many ‘highly significant’ results are only of small practical/clinical importance owing to their small effects [27, 28]. Furthermore, any null hypothesis can easily be rejected with a sufficiently large sample, and statistical tests can arbitrarily be rendered significant regardless of the relationship investigated [29]. Also, many statistical assumptions associated with NHST are misconceived despite their ritualistic use (cf., e.g. [30, 31, 32]). One such fundamental error is the combination of Fisher’s evidential statistic (
Chronic pain indices at baseline and after six treatments
Chronic pain
All pain data were normally distributed (K-S-Z:
For all analyses, the same results were obtained when the differences between the baseline measures of the two groups was accounted for [37].
Mean pain intensity reductions (scale values) and standard errors for myofascial trigger therapy (MT) and the combined therapy (MT and Cellconnect Impulse).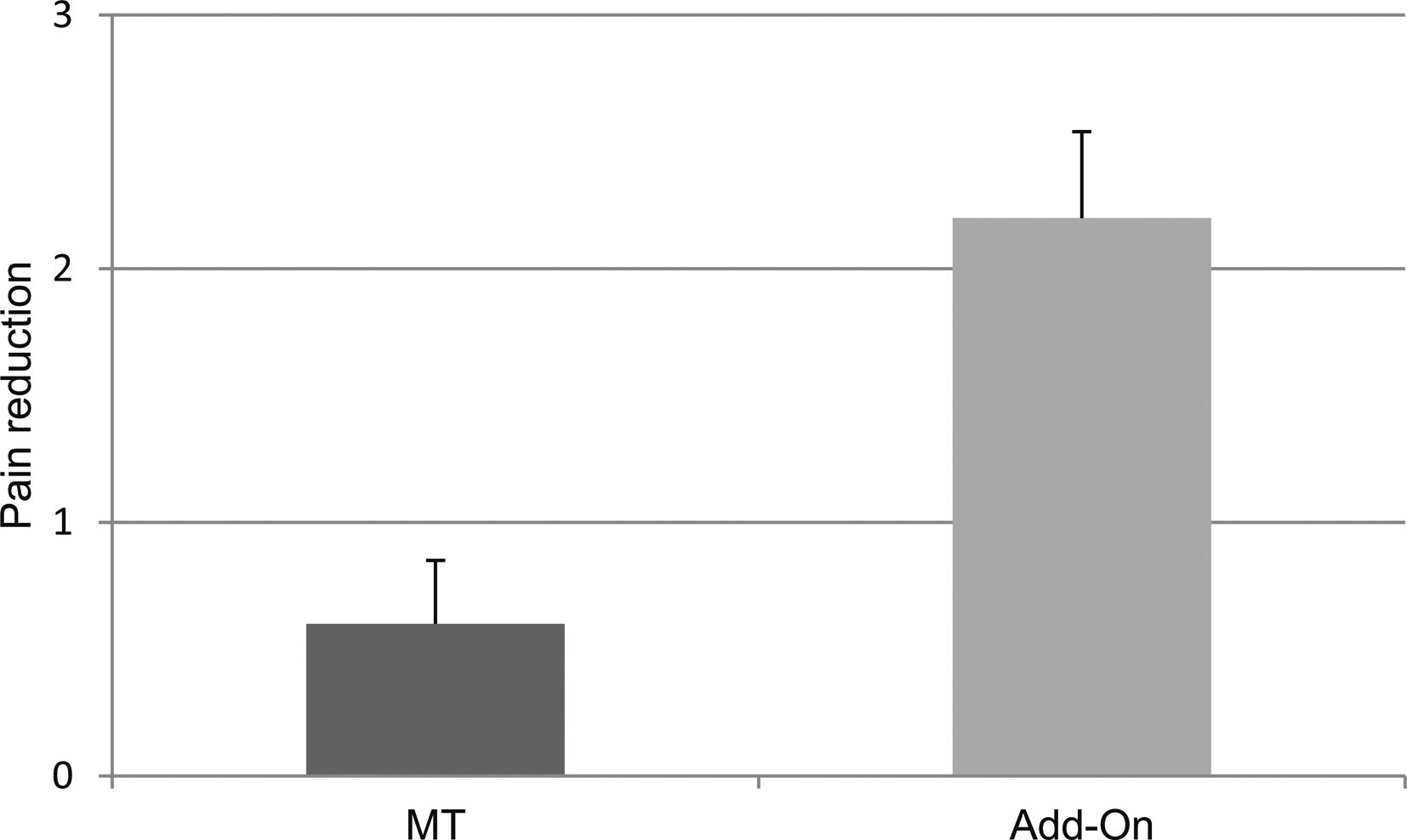
Pain hours and pain days reductions with myofascial trigger therapy (MT) and the combined therapy.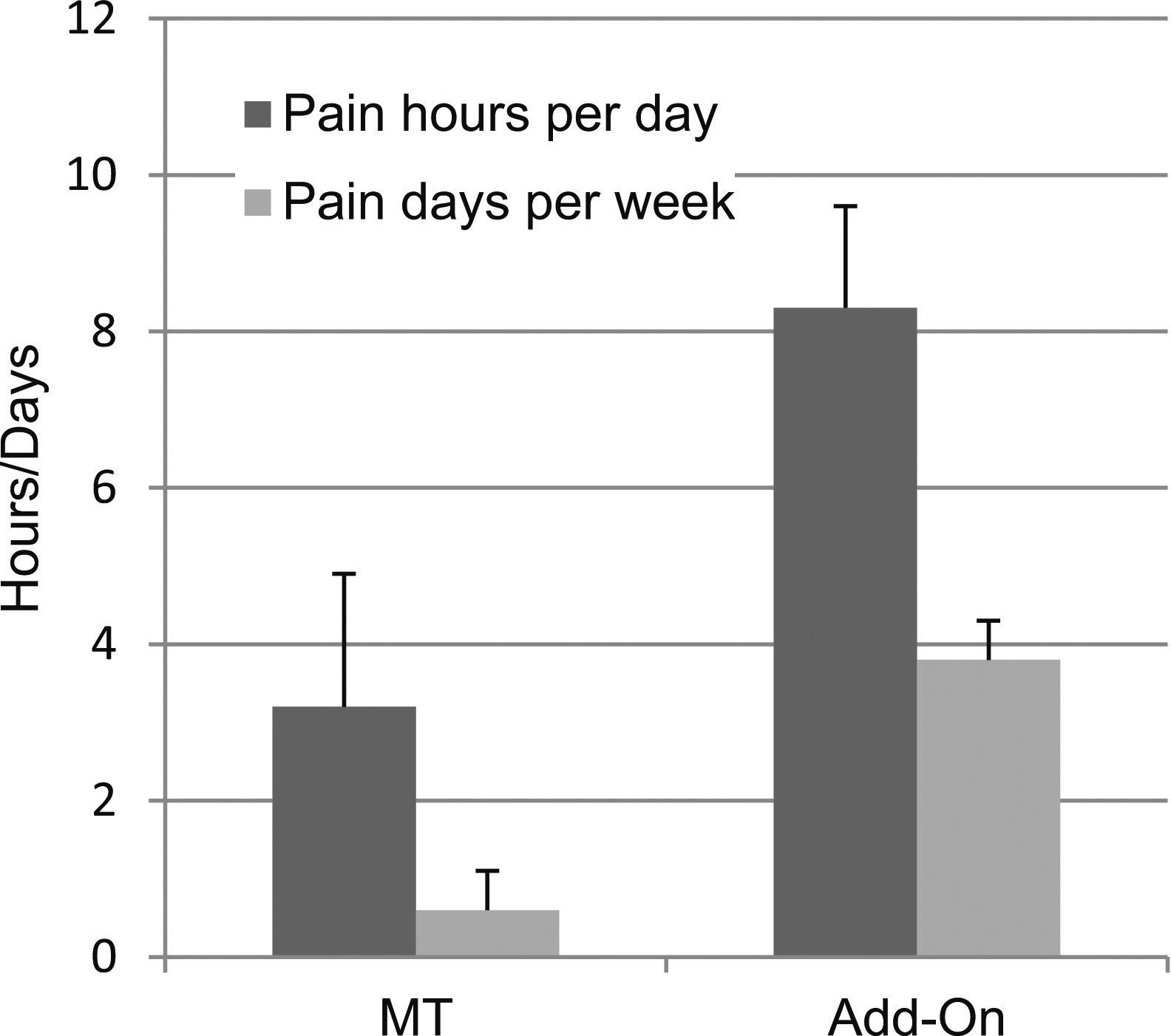
The difference between the two interventions was also visible in the number of pain days. In the MT group, pain days were reduced from 4.6 to 4 days. In the Add-on group, pain days were reduced from 5.9 to 2.1 days. The difference between the two groups was large (
Quality of life at baseline and after six treatments
Changes in quality of life dimensions (scale values) after myofascial trigger therapy (MT) and the combined therapy.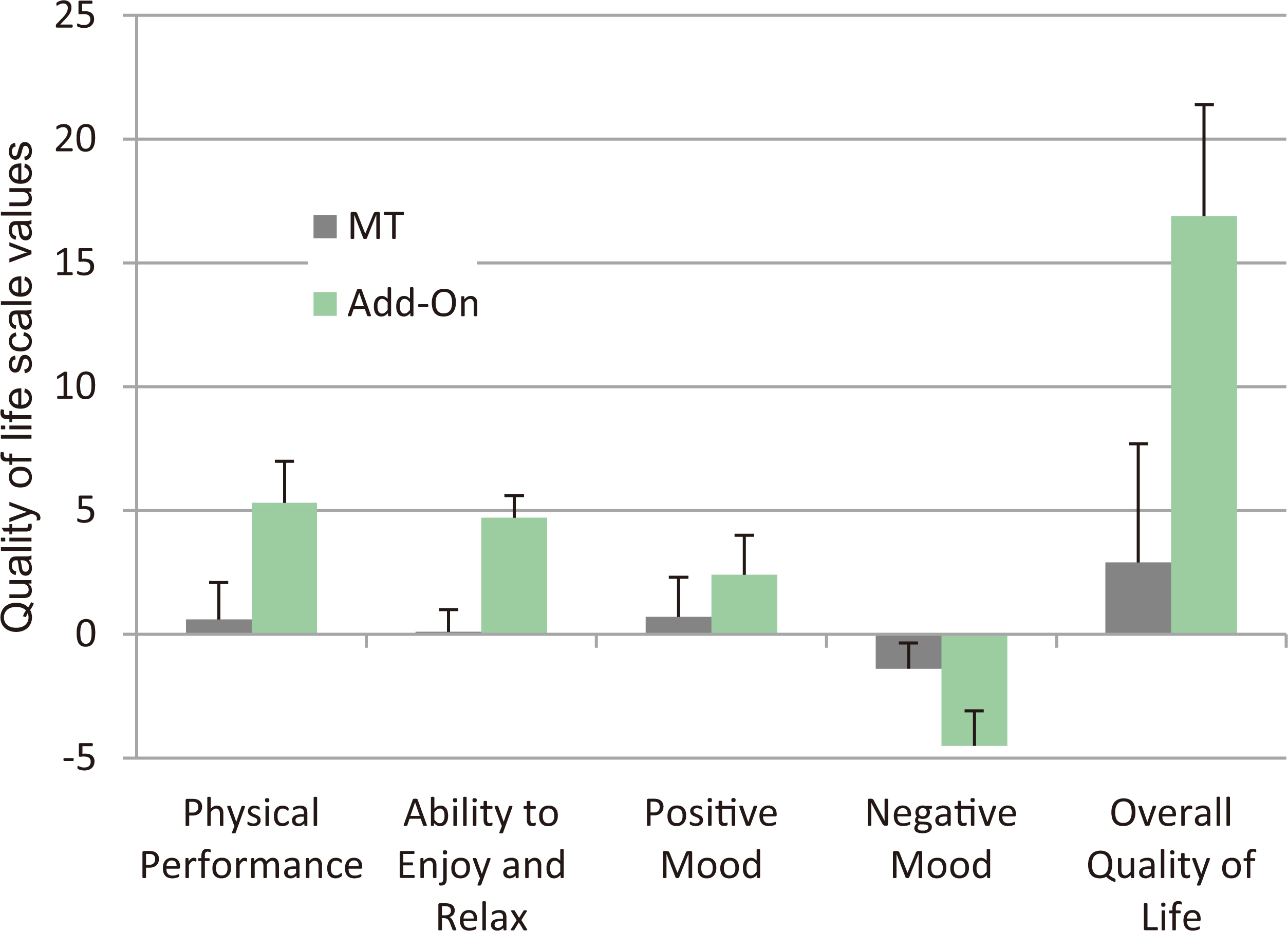
Table 3 depicts the mean ratings for the quality of life dimensions that were assessed before the first and after the last treatment. Patients receiving the Add-on intervention reported a higher quality of life at the end of the treatment. Specifically, their physical ability, as well as their ability to enjoy and relax was clearly larger (
To determine the overall improvement in quality of life, sum scores of all four scales were calculated and compared. Again, there was a large superiority for the Add-on intervention testifying to the notion that health related quality of life impairments were improved to a far greater extent under this treatment (
Discussion
The aim of this study was to investigate the effectiveness of a new vibrotherapy form, Cellconnect Impulse, in a routine clinical practice treating patients with a recorded medical history of chronic back pain. The results show that the effectiveness of a well-established treatment, myofascial trigger therapy, was vastly enhanced when applied in conjunction with Cellconnect Impulse. In fact, the pain relieving effect of MT (pre-treatment versus post-treatment) was small (
To put the practical and clinical relevance of these effects in perspective, it may be useful to illustrate their implications with regard to pain intensity. With a differential effect of
That such large effects were found is surprising given that the sample consisted of patients who on average suffered from chronic back pain for more than almost five years. In fact, some of them suffered from severe impairments to the degree of being resistant to conventional therapy. Most of them had come to terms with the fact they would live in pain. As such, the sample of this study parallels clinical data showing that in general chronic pain is difficult to treat, especially when non-pharmaceutical treatments are used [39]. There is evidence showing that in chronic pain patients extensive alterations in the neurologic pain matrix can be found. These comprise permanent changes of both activity and connections of important pain processing brain regions [40]. Such changes may increase anxiety and/or decrease reward learning or dysfunctional coping with pain. Also, in some chronic pain patients, the threshold for pain signals may be lowered which may further enhance physiological and psychological reactions associated with discrepant bodily processes [41, 42, 43].
Whether such decisive neurologic changes were existent in the present study remains open. The results found, however, were notable. With the exception of one patient all individuals treated with Cellconnect Impulse showed a reduction of pain and two out of fifteen patients were pain free after six treatments. On the other hand, no patient was pain free in the MT condition and the rate of non-responding was 40 percent (
There are a number of open questions this study could not address. Since it was designed as a practical trial, the efficacy of Cellconnect Impulse could not be determined. It is therefore unclear if the “pure” treatment effects are smaller or larger. For example, although treatment was standardized regarding treatment duration and software program, therapists were allowed degrees of freedom to meet the requirements of the patients’ individual needs (note, however, that the therapists were randomly assigned to patients). Furthermore, the nature of the study did not allow for examination of underlying effects of the therapy. Given that Cellconnect Impulse was used in conjunction with MT, it is unclear whether it exerted an auxiliary effect, a potentiating effect or a specific effect in the reduction of pain. Hence, it is unclear if the purported effects show in cell metabolic changes and the activation of self-healing processes. Such questions should be addressed in future studies employing several arms, different treatments, and various medical and psychophysiological parameters. Also, patients undergoing therapy with Cellconnect Impulse usually report sensations of prickling and “floating” when exposed to the treatment. It is likely that such sensations have a non-specific psychological effect which may add to the overall effect of the treatment [44]. Ideally, a sham condition could help to separate non-specific from specific treatment effects, but this is difficult to achieve since physical stimulation via the treatment table cannot be simulated. Additionally, part of a non-specific effect could also be due to the therapist’s expectations and experience with this form of treatment. To test for such effects patients would have to be treated with Cellconnect Impulse only. Lastly, although the effects found were large, it is unclear if and how long they lasted. In the present study, participants treated with Cellconnect Impulse discontinued treatment after six sessions. This was due to the nature of the study. In part, however, this was also due to the fact that the vast majority experienced strong improvement of their medical condition. Still, it is conceivable that the treatment effects abate over time or that the treatment needs to be repeated to warrant long-term effects. Future investigations should address this issue.
In sum, the present study is the first to show that combining MT with the new vibrotreatment Cellconnect Impulse provides a verifiable therapeutic advantage in the treatment of chronic back pain. The effects are large, fast-acting compared to conventional therapies, and show both in pain symptoms and in health related quality of life.
Clinical messages
Effectiveness of trigger point therapy for chronic back pain is significantly enhanced when combined with a new vibrotherapy (Cellconnect Im- pulse). Pain relieving effects are large ( Responsiveness in patients to this therapy is very high (
Footnotes
Acknowledgments
This work was supported by Cellconnect, Inc., Germany. I thank Nick Singer for helpful comments on the paper’s intelligibility.
Conflict of interest
This work was funded by Cellconnect Inc., Germany.