
Abstract
BACKGROUND:
Pulsed radiofrequency (PRF) used for knee pain originating from osteoarthritis is one of these methods.
OBJECTIVES:
The aim of the study was to evaluate the knee functional status and pain palliation following the application of pulse radiofrequency in patients with cardiac comorbid disease who were diagnosed with advanced stage osteoarthritis.
METHODS:
Thirty-eight patients with high surgical risk having cardiac comorbidities with grade 3–4 gonarthrosis according to the Kellgren-Lawrence classification were retrospectively analyzed. PRF was applied to the saphenous nerve of each patient. Visual Analog Scale for knee pain evaluation both at rest and on movement and the Lysholm Knee Scoring Scale for function evaluation were used. The patient status was evaluated before the procedure and at the first and sixth months after the procedure.
RESULTS:
The mean age was 68.8 years (range, 53–82 years). Both the rest and movement post-procedural Visual Analog Scale scores at first and sixth months were significantly lower than pre-procedural values (
CONCLUSIONS:
PRF is a safe and function sparing minimally invasive pain palliation method for knee osteoarthritis in elders with cardiac comorbidity.
Introduction
Senility disorders, such as gonarthrosis, have become more prevalent as the world population ages. In gonarthrosis, simple activities such as walking or climbing stairs, or even sitting or lying down cause pain that severely reduces the quality of life. Hence, immobility is inevitable, creatings a vicious cycle in which, pain brings immobility while mobility brings pain. Therefore, only pain relief can prevent continuation of this ill-fated cycle.
Osteoarthritis (OA) is a chronic non-inflammatory degenerative disease involving the synovial joints, characterised by cartilage destruction, osteophyte formation and subchondral sclerosis. It develops gradually and occurs most frequently, in weight-bearing joints [1, 2].
Although there are specified diagnostic criteria for knee osteoarthritis, in clinical practice OA is diagnosed based on history and physical examination. Radiological investigation is used to support the diagnosis and rule out any other pathologies.
According to a guideline from the Osteoarthritis Research Society International (OARSI), the aim of treatment is to relieve pain and stiffness, maintain and increase joint mobility, reduce physical deficiencies and disabilities, limit the progression of joint damage, increase quality of life for the patient, and inform the patient about the course of the disease [3]. An American College of Rheumatology (ACR) guideline classifies treatment options as non-pharmacological, pharmacological, surgical and research stage modalities [4].
Myocardial infarction and cardiac-related mortality are the most feared complications in patients undergoing non-cardiac or cardiac surgery [5, 6]. Accordingly, in the treatment of patients with OA together with a comorbid disease, conservative treatment methods may be preferred over surgery to avoid significant complications. Orthopaedic procedures are the second most common reason for non-cardiac surgery, following vascular procedures, in patients that have cardiac comorbidity according to the American College of Cardiology and American Heart Association guidelines [7]. Particularly total knee replacement, in which blood transfusion is often required, may increase morbidity and mortality for this patient group already at risk.
Conservative treatment options, including pulsed radiofrequency (PRF) and continuous radiofrequency thermocoagulation (CRFT), are easy and painless applications without risk, of thermal damage that have become widely used in recent years [8, 9]. PRF is a technique whereby radiofrequency oscillations gated at a rate of pulses per second (cycles per second defined as a Hertz) are delivered to a target nerve. Although PRF is frequently applied, the mechanism of action for pain relief has not yet been fully clarified. However, it is thought that it causes a neuromodulator effect [10].
The aim of this retrospective study was to evaluate functional status of the knee following PRF pain palliation in elderly patients with at least one cardiac comorbid disease who presented to the algology clinic for knee pain due to advanced osteoarthritis.
Material and method
This retrospective study included 38 patients aged
Patients with findings of systemic and/or local infection, reasons other than gonarthrosis for knee pain (e.g. discogenic pathologies, hip pathologies, ankle pathologies, previous history of knee surgery and chronic trauma), malignancy, systemic inflammatory diseases, a previous history of allergic reactions to local anaesthetics or any implanted electrical device such as a cardiac pacemaker were excluded from the study. Bilateral PRF applied patients were also excluded from the study so as not to obscure the statistical analysis of the Visual Analog Scale and Lysholm knee scores.
PRF was applied to the saphenous nerve of all patients and there were no subsequent interventions performed within the six months following the PRF procedure. Management of anticoagulant or antiplatelet therapy before and after this minimally invasive procedure was carried out according to the American Society of Regional Anesthesia and Pain Medicine guideline [12]. Sterile technique was used throughout the procedure. The knee area was stained with povidone iodine and covered with a sterile drape. Infiltration anesthesia was ensured with 2 mL 2% lidocaine before the procedure. A Neurotherm JK4A radiofrequency generator was set for 20 ms bursts at a frequency of 2 pulses per second (2 Hz) for 120 s. The full procedure took eight minutes, composed of four sessions of 120 s in which the temperature was below 42
All the procedures were performed in the supine position with the leg fully extended at the knee and the ankle dorsiflexed so that the long axis of the foot formed a 90
Age, gender, body mass index (BMI), comorbidities, ASA classification, and previously used medications were recorded for each patient. Basal knee pain scores (at rest and on movement) and the functional status of the patients were evaluated before the procedure and at the first and sixth months after the procedure. Knee pain was evaluated with a 100 mm Visual Analog Scale (VAS) whose ends were labeled as extremes (“no pain” and “pain as bad as it could be”). Knee functions were evaluated using the Lysholm knee scoring scale which was validated in Turkish and which questions eight different items limping (5 points), restraining (15 points), need for support (5 points), instability (25 points), swelling (10 points), climbing stairs (10 points), squatting (5 points) and pain (25 points). The total score ranges from 0–100. Higher scores indicate a better outcome [13].
Statistical analysis
Data obtained in the study were statistically analyzed using SPSS v. 20.0 software (Statistical Package for Social Sciences, USA). Data were expressed as the mean
Results
The demographic characteristics of the patients, gonarthrosis stages, and the number of comorbid diseases are presented in Table 1.
Demographic analysis, gonarthrosis grading, laterality of radiofrequency treatment and comorbidity
Demographic analysis, gonarthrosis grading, laterality of radiofrequency treatment and comorbidity
The study group was comprised of 5 (14%) males and 33 (86%) females with a mean age of 68.8 years (range, 53–82 years). PRF was applied to the left knee in 15 (40%) patients and to the right knee in 23 (60%) patients.
Grading of the gonarthrosis of the patients was done according to the Kellgren-Lawrence classification (9). The severity of gonarthrosis was determined to be grade 3 in 13 (34%) patients and grade 4 in 25 (66%) patients. There was no relationship between the demographical characteristics (age, gender, BMI and stage of disease) and Lysholm knee function scores in the sixth month (Table 2).
Correlation of demograhical data with Lysholm scores at sixth month
Basal VAS scores both at rest and on movement were significantly higher than the VAS scores stated by the study participants at the first and sixth months after the procedure (
Pre- and post-procedural pain analysis and knee function analysis at rest and on movement
Graphical demonstration of alterations in VAS and Lysholm scores within six months.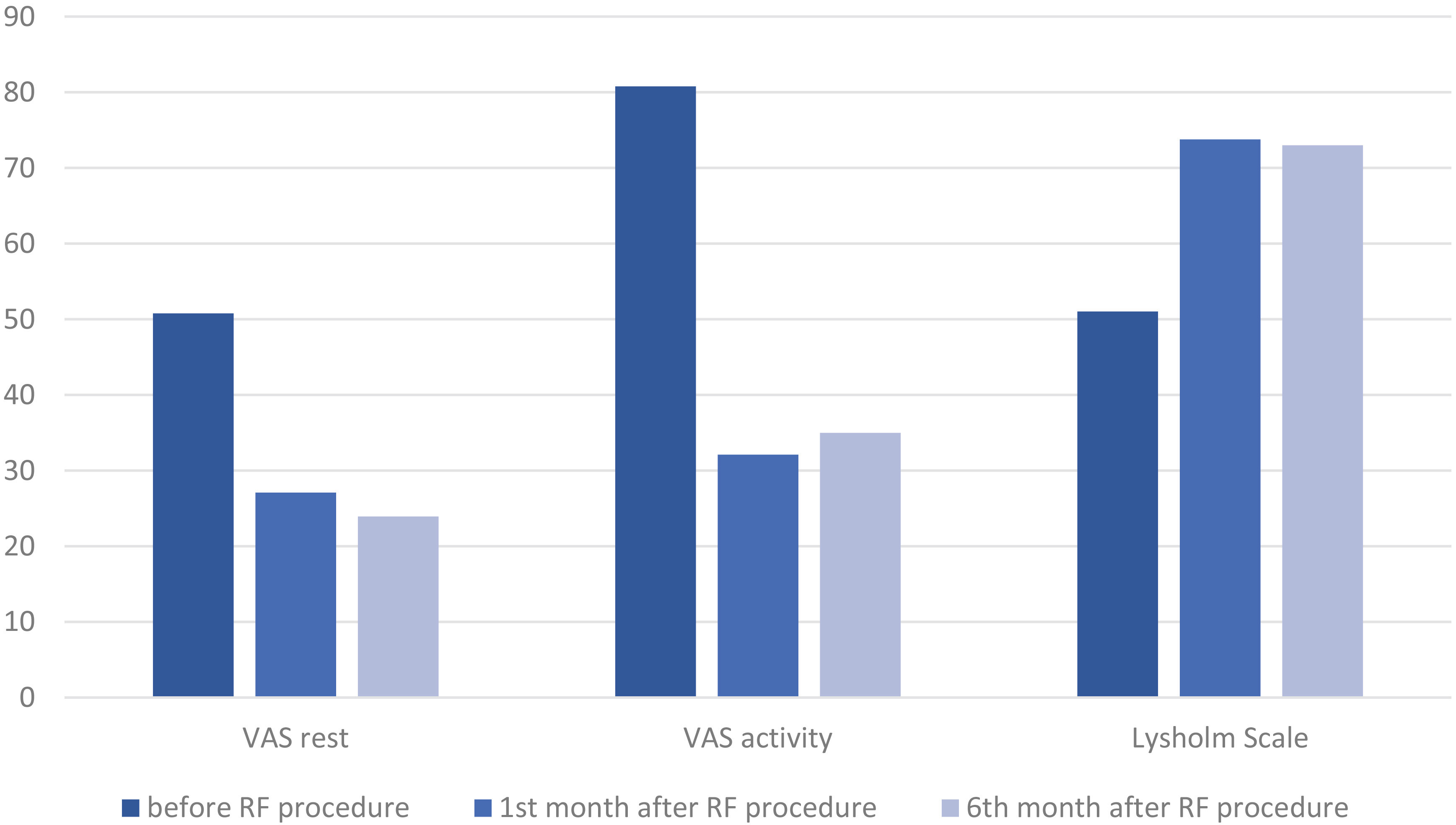
No complications including bleeding or infection were observed in any patient.
Both functional activities and walking speed of geriatric patients with comorbid-disease exhibit a significant decline after a total knee replacement operation. This may increase the hospitalization periods, decrease independence levels, and lead to the development of several complications [14]. PRF, which is thought to have a neuromodulator effect, is a currently used method for pain management in gonarthrosis [8]. This minimally invasive procedure is preferable, especially for surgically high-risk patients. Transfer and mobility activities are improved in the early stages of this treatment due to, quick pain relief. Another advantage of the procedure is that it does not require hospitalization.
PRF block for different nerves has been attempted for pain relief over the last 20 years. The obturator and femoral nerve block for hip pain and an occipital nerve block for occipital neuralgia are among the experimental procedures [15, 16]. Saphenous nerve RF is a relatively under-studied field. The earliest papers in the literature regarding PRF application for knee pain originating from OA were published in 2011 [17, 18, 19]. The results of these studies were similar to those of the present study: PRF was effective for both pain relief and functional improvement. The only randomised prospectively designed study among these was performed by Choi et al. with the others, including the present study, being retrospective reviews [19].
The radiofrequency procedure can be applied directly to the joint or the nerves supplying sensation to the joint [15, 17, 19, 20, 21, 22]. Conventional and ultrasound (US)-guided methods are two different methods of nerve block applications. The success rates of these two methods vary according to the clinician’s experience [23]. None of the studies performed to date have established which nerve block techniques are more successful [23]. Fluoroscopic guidance is also an alternative method for nerve block of knee pain [19]. Actually, the experience of our pain clinic with the conventional technique has not been difficult, especially when the patient is cooperative. It is made, even easier because US usage requires additional experience and equipment. Since the conventional method is used successfully in our clinic, all the study participants were treated using this technique.
Knee radiofrequency is a good choice for patients who have not benefitted from various conservative treatment methods, for those from whom total knee replacement has been postponed for any reason, or for the treatment of neuropathic pain that develops after a total knee replacement [24]. Because radiofrequency is typically preferred for patients with advanced stage gonarthrosis which requires total surgical arthroplasty, it should be considered as a final stage conservative treatment appropriate for surgically high risk patients. In the current study, PRF was performed on gonarthrotic patients who were defined as surgically high-risk patients due to, their cardiac comorbidity.
All of the knee RF studies have excluded patients diagnosed with coagulation disorders or those who are medicated with antithrombotic or anticoagulant drugs because physicians hesitate to perform this procedure on such patients, although it is minimally invasive [17, 18, 19, 21, 22]. In contrast, almost all subjects participating in our study used these kind of medications because of their existing cardiac comorbidity. Hence, we followed the recommendations of the American Society of Regional Anaesthesia and Pain Medicine to avoid drug-related complications [12]. No heamatoma or bleeding complications were observed in any of our patients.
The study design is retrospective and there are limited number of subjects included because of limited number of patients who fulfilled our inclusion criteria and were admitted to our clinic. Another limitation was that very short follow-up duration was common among studies similarly to the present one. The duration of clinical follow-up was six months for most studies which was used to validate follow-up duration of the present study [17, 18, 21]. The follow-up time was only three months unfortunately in the brand new declaration of Shen et al., which had a randomized prospective study design as a positive feature and in which cases gained significantly better pain and function scores similar to the study performed by Choi et al. [19, 22]. Although these are limitations of the present study, the results are promising for PRF to be a part of a treatment protocol in advanced gonarthrosis when surgery is too risky.
In conclusion, PRF is a safe, minimally invasive, alternative treatment modality in advanced gonarthrosis for surgically high-risk patients who did not respond to other conservative treatment modalities. In our series the procedure was safe even for patients treated with anticoagulant or antithrombotic medications when necessary precautions were taken. Its success is probably due to pain relief, which gives the opportunity for greater joint movement, thus improving the joint function. Prospectively designed studies including a large number of subjects are required for more detailed and accurate data on this topic. There is also a need for randomized, comparative studies to determine which of the conservative and US guided methods is superior. Finally, the effective duration has not been established in the literature, and thus follow-up durations should be longer in upcoming studies.
Footnotes
Conflict of interest
None to report.