
Abstract
BACKGROUND:
Hippotherapy is a form of therapeutic exercise for conservative treatment of lumbar spine segmental instability and/or hypomobility in subjects with low back pain (LBP).
OBJECTIVE:
The current study evaluates the effects of a hippotherapy simulator on pain, disability, and range of motion (ROM) of the spinal column in subjects with mechanical LBP.
METHODS:
In a randomized clinical trial, 80 subjects were randomly assigned to either the control or intervention groups. All subjects underwent routine physiotherapy. In addition, the intervention group underwent hippotherapy with a hippotherapy simulator for 15 sessions, each lasting 15 minutes. Pain, disability, and ROM of the lumbar spinal column of the subjects were measured in the first and last physiotherapy sessions respectively.
RESULTS:
Improvement in pain intensity was higher in the hippotherapy simulator group over the first eight days of treatment (Hippotherapy vs. Control Point changes: Day 12:
CONCLUSION:
The hippotherapy simulator decreased pain and disability in subjects with LBP; however, no additional improvement in lumbar spine ROM was observed.
Background
Low back pain (LBP) is one of the most common musculoskeletal disorders affecting humans: it has an enormous social and financial impact [1, 2, 3, 4]. While the one-month prevalence of LBP is 35%–37% with a slightly higher prevalence in females, its lifetime prevalence is estimated to be 59% with peak prevalence between 45–59 years. Although about 10% of back pain episodes require consultation with a general practitioner, 90% improve within one month. Of those subjects who stop seeking care, the majority become symptomatic again within one year, only 21% and 25% have complete recovery from pain and disability, respectively [1, 3].
Mechanical LBP (nonspecific low back pain) is the most common type. Multifactorial origin can be traced in a majority of subjects with mechanical LBP: this includes functional or segmental instability, deconditioning, abnormal posture, poor muscle recruitment, emotional stress, senile changes, and injuries such as disk degeneration, arthritis, or ligament hypertrophy [5, 6]. It is believed that segmental instability caused by tissue damage, poor muscular endurance, or control or a combination of all three factors is a common aspect in mechanical LBP [7].
Occasionally, the treatment of subjects with chronic LBP is clinically challenging. Rapid initiation of therapy and encouraging patients to become active and self-efficient are of immense importance. In some subjects disabled with LBP, multidisciplinary management and interdisciplinary rehabilitation may be indicated. For treatment to be successful, the social and psychological concerns of the subjects should be addressed [1, 5, 8, 9].
Riding-of-a-horse has been proposed as a treatment in the handling of neuromuscular disorders [10]. It has been proposed as a method of physical rehabilitation employing a genuine saddle horse to stimulate the somatosensory, proprioceptive, and vestibular systems in tune with the horse’s motions to improve standing, major motor function, alignment, and stability [11].
It is believed that a hippotherapy simulator is a therapeutic exercise option for the treatment of segmental instability and hypomobility [12, 13]. In addition, complications such as fractures caused by falling are greatly reduced using hippotherapy simulators under proper supervision.
Hippotherapy simulates the motion of a horse as part of a continuous therapy package to provide postural or stability training. This rehabilitation develops unified intuitive stimulation plus motor responses [14]. It engages movement hits that are produced by the horse’s spine while the animal walks: this leads to beneficial consequences [15].
Segmental instability and hypermobility are one of the subgroups of mechanical LBP [16, 17]. Hippotherapy produces up and down, forward and backward, and right and left motions, and conveys them from the back of the horse to the subject(s). Eccentric contraction of the muscles of the spine during horse riding strengthens muscles and stabilizes segmental hypermobility to improve the active and passive components of the spine [12, 18, 19].
Horvat et al. [20] have demonstrated that muscle power improved by horseback riding has been discussed as an important part of health and has been related to the enhancement of subjects’ potential to do daily activities. Yoo et al. [21] showed that hippotherapy can be beneficial in LBP and improvement of back surgery by increasing trunk power, and equilibrating muscles with flexor and extensor obligation in subjects with LBP.
Hippotherapy contains actions centered on riding a horse. It provides postural and gestural exercise for subjects: these are carried out throughout rehabilitation sessions. Accordingly, subjects are directed into diverse excitation situations on a horse, including sitting forward, backward, or sideways. Occasionally, they are instructed to take creeping, converting, or standing positions for the purpose of therapy [15]. Hippotherapy is a part of rehabilitation treatment to attain social and emotional recovery through horse riding and is a full-body workout compared to exercise programs that the subjects can do from home. It enhances social interaction, enjoyment, and recovery of self-regard, and is an incentive to be active [22, 23].
The benefits of hippotherapy have persuaded researchers to develop simulators to decrease healthcare costs and provide access to all subjects. These devices mimic the three-dimensional movement of a horse.
Studies have demonstrated the value of actual horseback riding [24, 25]. However, this is restricted by availability, high cost, and safety factors [10]. To overcome these limitations and take into account the scarcity of studies carried out with a simulator, the current study used a horse simulator to study the effects of hippotherapy on mechanical LBP for variables of pain, physical disability, and range of lumbar spine mobility.
Methods and materials
Participants
This was a randomized, single-blind, controlled clinical trial carried out in Tabriz, Iran from March to August 2011. The subjects were patients with mechanical LBP who referred to the outpatient physical therapy center of the Physical Medicine and Rehabilitation Department of the Tabriz University of Medical Sciences in Tabriz. Non-mechanical causes of back pain were ruled out by clinical examination, and imaging as and when necessary. Symptoms of a non-mechanical origin of LBP are: inability experience increase in pain with changing physical position of the lumbar spine, hypomobility in the thoracic spine [26, 27], the subject’s age, gender, morning discomfort and painfulness, deteriorating symptoms contrary to relaxation, and enhancement of symptoms as the day proceeds [27, 28].
After obtaining written informed consent from 80 patients, all subjects were randomly assigned to the control (
Intervention
The intervention and control groups received 15 sessions of standardized conventional physical therapy tailored to LBP and dysfunction: these were supervised by a physiotherapist. The program consisted of application of physical modalities followed by therapeutic exercises. The physical modalities were surface heat (hot pack), deep heat (ultrasound), and transcutaneous electrical nerve stimulation on the pain pathways and lower back. Therapeutic exercises included lumbar and core stabilizing and strengthening, such as pelvic tilt and flexion-extension exercises; and lower back stretching, such as knee to chest exercises. Subjects exercised for 10 cycles (one session) supervised by a physical therapist. The next two sessions were performed at home.
Subjects in the intervention group were also treated with a hippotherapy simulator for 15 sessions, each lasting 15 minutes. The hippotherapy simulator used in this study was ‘the AZ Horsebak Riding Machine (Azimuth fitness)’. Subjects remained in sitting position for 15 minutes on the simulator during these sessions, with extension of the trunk and stabilization of the pelvis. Feet were placed on the footplates as the simulator produced a rhythmic and repetitive movement similar to a walking horse. The simulator can produce several modes of rhythmic and repetitive motions. Treatment sessions were carried out in preparatory mode assuming they would result in better transmission of motions to the user. To prevent sudden muscle tension or stress, subjects were instructed to perform several trunk rotation exercises to the left and right before switching on the device.
Study variables
The outcome variables measured were pain, physical disability, and lumbar spine range of motion. Physical disability was assessed using the Roland-Morris Disability Questionnaire (RMDQ). RMDQ is one of the most considered, most validated, and reliable back pain-specific outcome measure used in trials [27]. It has been suggested for use as an international standard questionnaire in back pain research [30]. This questionnaire is a self-administered disability questionnaire comprising 24 items to be completed by subjects. These questions relate specifically to physical functions likely to be affected by LBP. In this study, RMDQ was completed at the commencement of the trial and after completion of the 15
Sample size
Considering VAS [45, 46, 47] as primary outcome and in keeping with existing literature, the power was set at 90% with
Change score
The change scores (MCID) were outcomes of difference between pre-treatment and post-treatment scores. They were calculated as follows: mean (baseline score – week n score). It must also be noted that baseline score is subtracted from week n score to achieve positive scores, and there is a reprehensible interpretation in calculating the MCID for RMDQ and VAS scores.
Statistical analysis
The collected data was analyzed by SPSS 16.0 software. Frequencies and percentages were applied to present categorical variables, and mean and standard error were utilized for continuous variables. The Kolmogorov-Smirnov test was used to test for normalcy of continuous variable in each level of the independent variable, and homogeneity of variances was assessed using Levene’s test. The categorical characteristics were compared by
Comparison within groups and between groups changes at different times during the study. This was analyzed utilizing mixed design ANOVA procedure. Initially, we checked to make sure that the data can actually be analyzed using mixed design ANOVA. Mauchly’s Test of Sphericity indicated that the assumption of sphericity had been violated. To overcome this problem, corrections were applied to the degrees of freedom (df) by the Greenhouse-Geisser corrections. Pairwise comparisons were corrected using Bonferroni adjustments. P-value less than 0.05 was considered a significant level in this study.
Comparison of demographic variables and the outcome measures at baseline
Comparison of demographic variables and the outcome measures at baseline
BMI, Body Mass Index; VAS, Visual Analogue Scale; RMDQ, Roland Morris Disability Questionnaire.
No subjects were excluded during the study, and no adverse effects were detected after application of the treatment. That is, all eighty patients allocated to the intervention and control groups continued the full course of treatment (see CONSORT flow diagram in Fig. 1).
Functional and physical evaluations of the subjects in each group at baseline and during study period
Functional and physical evaluations of the subjects in each group at baseline and during study period
VAS, Visual Analogue Scale; RMDQ, Roland Morris Disability Questionnaire.
CONSORT 2010 flow diagram for the randomized clinical trial for hippotherapy and mechanical low back pain.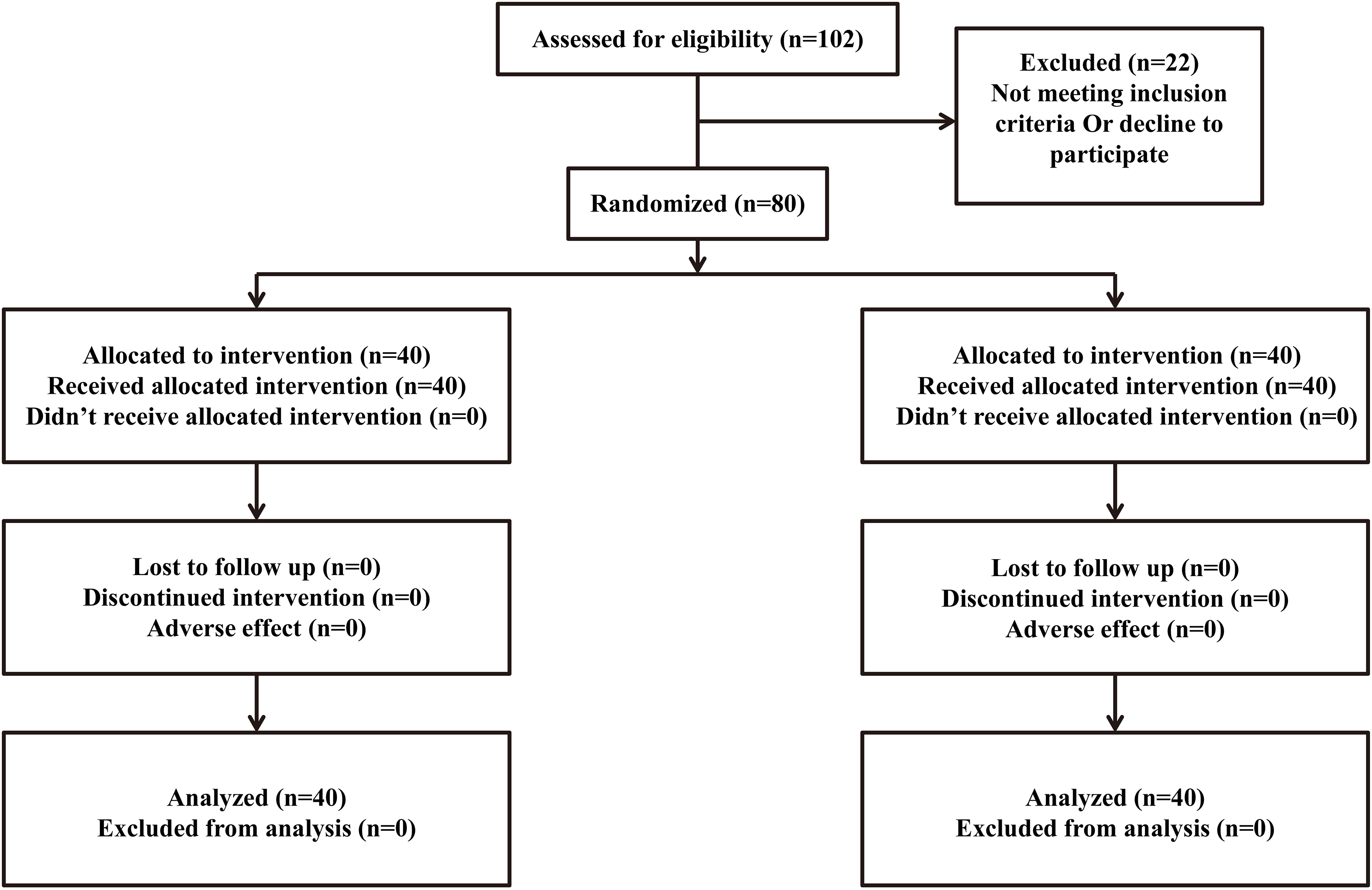
Comparison of changes in VAS, RMDQ and modified Schober test scores during the study period between study groups
VAS, Visual Analogue Scale; RMDQ, Roland Morris Disability Questionnaire.
Changes in pain severity using the visual analog scale score at various periods of the study.
Changes in physical disability score using the Roland Morris Disability Questionnaire at various periods of the study.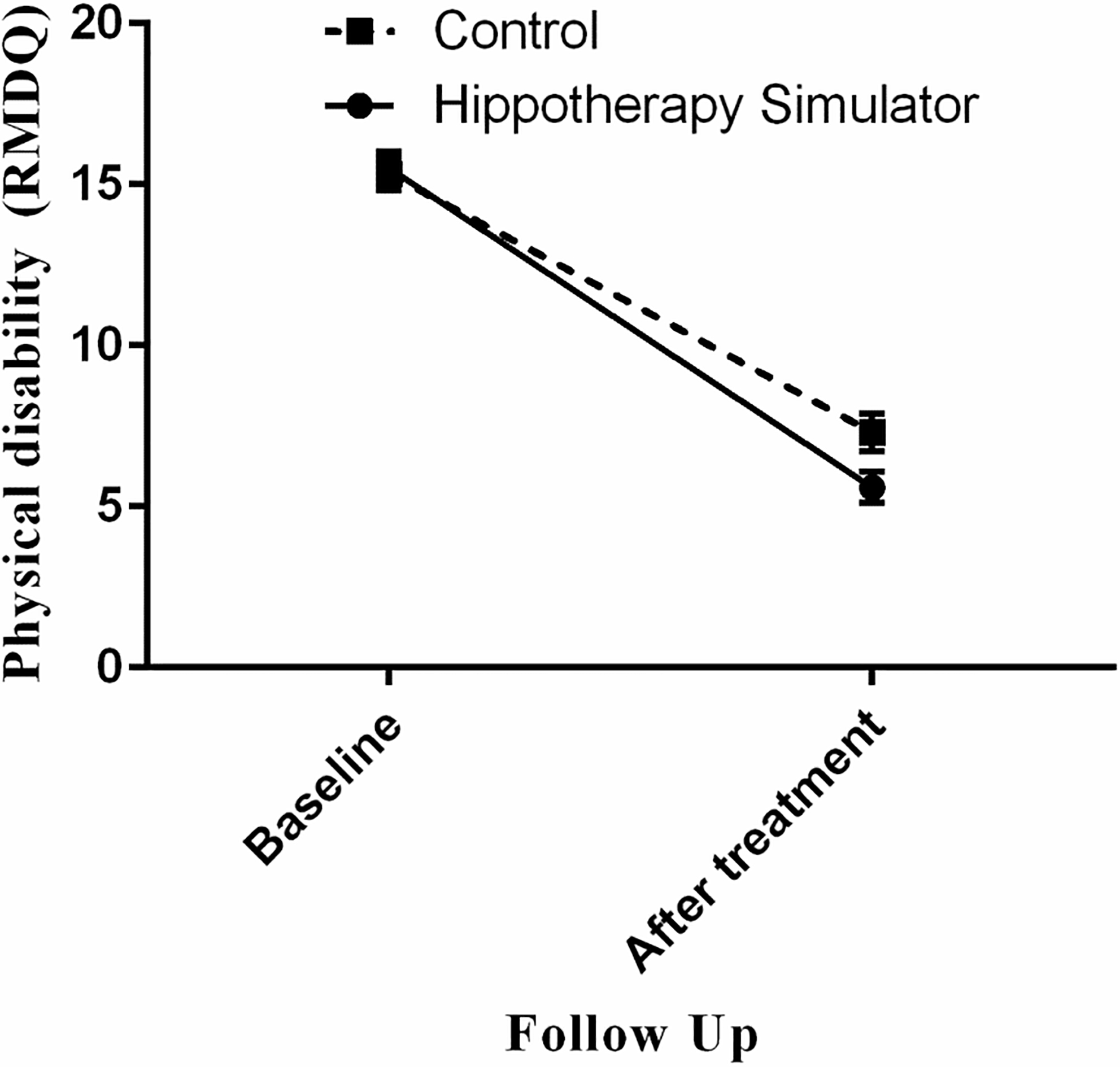
The trial recruited 80 patients with low back pain, predominantly male (70%) with mean age of 46.24
The results show that going through eight days of treatment results in significantly lower pain intensity in both groups. The pain score decreased by 35.95
Comparison of the change scores between the study groups revealed that pain intensity improvement was higher in the hippotherapy simulator group over the first eight days of treatment. Also, undergoing hippotherapy simulation sessions resulted in considerable superior improvement in physical disability with regard to the Roland Morris Disability Questionnaire (point changes in hippotherapy group vs. control group: 9.90
The present study demonstrates that the degree of disability and intensity of LBP decreases significantly in the intervention group in comparison with the control group. This indicates that a hippotherapy simulator can be regarded as a conservative therapy option for treatment of mechanical LBP. It shows no additional benefits for lumbar spinal range of motion. A hippotherapy simulator simulates the movements of an actual horse as a rhythmic gesture, excluding the heat of the animal’s body. There is very little evidence on the efficacy of hippotherapy for the treatment of mechanical LBP. To our information and as per current scientific resources, available evidence about the usage of hippotherapy in subjects with mechanical LBP is exceptional.
A few studies have examined the effect of horse therapy for LBP. As in the present study, these studies have shown that hippotherapy decreases pain and disability scores and increases the segmental stability of the spine [12, 18, 49, 50]. Because a hippotherapy simulator is a mechanical device and not a real horse, it is difficult to determine if the therapy influences a subject’s self-image. Several studies have reported the overall effect of hippotherapy on regulating muscle tone, reducing pain, improving postural control, and providing psychological benefits in subjects with neurological impairment [49, 51, 52, 53]. Lechner et al. found that the spasticity-reducing effect of hippotherapy were significantly different from other interventions (sitting astride a Bo bath roll, and sitting on a stool with a rocking seat) used for self-rated spasticity by VAS. However, the effects on spasticity were not permanent. Only the hippotherapy group reported mental well-being [54]. It should also be noted that numerous physiological differences exist between these patients and the subjects with mechanical LBP, including spasticity.
The development of chronic LBP results from pathogenic mechanisms, including connective tissue plasticity (pain psychology, postural control, and neuroplasticity) [55]. It can be deduced that hippotherapy improves these biomechanical impairments and can decrease pain and physical impairment in subjects with mechanical LBP. Because a hippotherapy simulator imitates three-dimensional movement of a horse, the results obtained in this study were expected to be equally effective. The physiological origin of hippotherapy is the multi-dimensional transference of a horse’s motion over to a subject’s trunk [56].
In hippotherapy, the subject makes no effort at controlling the animal. Instead, with every step the animal takes, the subject responds to the three-dimensional motion deviation. Focused alteration of the animal’s rapidity and route of motion afford chances for randomization, protective, and responsive reactions from the subject. Reactions to equilibrium disturbances increase in output and effectiveness with repetition chances [57]. Additionally, favorable effects of hippotherapy on muscle power have also been shown in studies. Giagazoglou et al. [58] established the positive effects of a training program on subjects’ lower limb muscles. Throughout horse-assisted activities, the periodic forward and backward motions of the horse may strengthen leg muscles of subjects and correct gravity shift and postural reactions [59].
Although the relation between lumbar range of motion and functional ability or disability of subjects with chronic LBP is weak or non-existent [60], these have traditionally been the standard assessments used to determine disability in subjects with LBP. There are several assessment techniques for measuring range of motion of the lumbar spine. In this study, end range of motion during simple movements was measured by Modified Schober’s test. It was observed that the hippotherapy simulator and physical therapy alone resulted in the same amount of improvement in lumbar spinal range of motion. Contrary to the results of the present study, Janura et al. [61] reported that hippotherapy may improve the range of motion of the knee joint in the sagittal level as well as the flexion of the hip joint in subjects with chronic LBP. The importance of the decreased lumbar range of motion in subjects with LBP is unclear, because many people without LBP also have limited range of motion. Range of motion can vary by time of day, the effort the subject expends, and many other factors [5]. The improvement of the lumbar range of motion in both groups could relate to the exercises recommended during the course of treatment. The lack of more pronounced improvement in the range of motion of the spine in the intervention group revealed that hippotherapy and the hippotherapy simulator have no extra effect on improving lumbar range of motion.
The current study has some limitations. The subjects represented a sample of subjects with mechanical LBP referred for physiotherapy. Although this sample is believed to be representative of subjects with symptomatic mechanical LBP in theory, these findings may not generalize to all subjects. In addition, the information about how the device simulates the movement of a real horse is limited to the description given by the manufacturer. Attention should be given to the similarity of movement between the hippotherapy simulator and actual horse therapy and its effects on the human body. Furthermore, the follow-up for the current study was only immediately after the end of the treatment period, and there was no further follow-up to determine the long-term effects. The sample size of the present study was also small and the participants were restricted to an identified range of pain score at baseline, which further restricts the generalizability of the results. This was a single-blind, randomized trial instead of a double-blind technique which would have affected the results.
The results obtained from this study should be assessed in subsequent studies so as to determine the effect of the hippotherapy simulator under other conditions. It is noteworthy that no adverse effects were observed during this study.
Conclusion
A combination of use of a hippotherapy simulator and physiotherapy can further decrease pain and disability in subjects with LBP. However, no extra benefits improving lumbar spine range of motion were observed. Clinical trials on a larger scale should be conducted to confirm the results and determine whether or not hippotherapy simulators can improve the long-term outcomes of treatment for LBP.
Footnotes
Acknowledgments
The authors would like to thank the participants who helped to conduct this study and the staff of the Physical Medicine and Rehabilitation Research Center (Tabriz, Iran) for their assistance during the study. The study protocol was approved by the Research Ethics committee of the Tabriz University of Medical Sciences. Written informed consents was taken from all participants. The clinical trial was registered in the Iranian Registry of Clinical Trials with reference number IRCT201012014104N3, available at: , accessible through the world health organization database of clinical trial registries. This study (the design of the study and collection, analysis, and interpretation of data and writing the manuscript) was financially supported by the Physical Medicine and Rehabilitation Research Center of Tabriz University of Medical Sciences.
Conflict of interest
None to report.