
Abstract
BACKGROUND:
Kinesio taping (KT) is a new taping modality frequently used in the clinical setting. However there is contradictory evidence about its effectiveness in patients with neck pain.
OBJECTIVE:
To determine the effectiveness of KT as a supplementary treatment in addition to conventional rehabilitation in patients with neck pain.
METHODS:
Forty-five subjects with neck pain were included in this controlled trial and were assigned to the following groups: Kinesio Taping, placebo (P), and conventional rehabilitation control (CR). A daily self-assessment record of perceived pain, medication intake, quality of life and range of motion was registered at baseline, posttreatment and follow-up.
RESULTS:
Cohen’s coefficient showed large effects in terms of reducing pain perception in all three groups. ANOVAs showed that the course of treatment differed across groups only for neck flexion (
CONCLUSIONS:
A protocol of manual therapy and physical exercises, significantly improved pain and mobility in patients with neck pain. We obtained no evidence of additional benefits from the use of KT in this population.
Introduction
Cervicalgia or neck pain is one of the most common sources of musculoskeletal pain in the general population and it constitutes one of the major health problems in western society. Its estimated prevalence ranges between 16.7% and 71.5%, and it should be emphasized that up to 50% of these cases could become chronic [1, 2, 3, 4].
Recently, Kinesio Tape (KT) has become a widely used tool in the practice of physical therapy. The method provides a greater pain-free range of motion in the musculoskeletal system [5]. The singular characteristics of the bandage itself and its application are probably responsible for the physiological effects attributed to Kinesio Taping: analgesic effect; effect on the muscles, by stimulating muscle tone; positional effects, in providing support to the joints; circulatory effects, by activating lymphatic drainage and microcirculation; and neuroreflexive effects.
At present, the scientific literature on KT shows contradictory results; some authors claim clear benefits while others argue that there is no significant improvement derived from the application of the KT technique [6, 7, 8, 9, 10, 11, 12]. In terms of musculoskeletal pathology, KT seems to render positive results in the management of low back pain [13, 14, 15], subacromial impingement [6, 17], patellofemoral pain syndrome [18], recurrent ankle sprain, and plantar fasciitis [19]. However, few studies show contradictory results in cases of cervical pain. More specifically, a study which included subjects who had suffered acute whiplash injury [20] showed that the use of KT provided beneficial effects when compared against a placebo control, improving cervical range of motion, and reducing the level of pain immediately after the accident and 24 hours later. The authors of the study, however, considered that their results were not clinically significant. A subsequent study demonstrated that patients with mechanical neck pain who received cervical thrust manipulation displayed greater range of rotation motion than those treated with KT. However, this study did not include placebo or control groups [21].
Given the current controversy on the presumed usefulness of KT in treating various pathologies, and the paucity of studies aimed at investigating the effectiveness of this technique in cases of neck pain or cervicalgia, the present study was designed to examine the short, medium, and long-term efficacy of KT used as a supplement to conventional rehabilitation in the treatment of mechanical neck pain.
Method
Participants
Patients from a primary health center of Toledo (Castilla-La Mancha, Spain) were selected from among those patients suffering from mechanical neck pain who had been diagnosed by their primary care physician. They were referred to the physical therapy service between February and July, and between October and November of 2011 and 2012.
First an experienced physical therapist performed a clinical assessment of patients who had been referred, fulfilled inclusion criteria and agreed voluntarily to participate in the study. At that time, the physical therapist obtained socio-demographic data (i.e., sex, age, level of education, occupation, and medication), and obtained information on the duration and localization of symptoms. Inclusion criteria were the following: (1) ages between 18 and 55 years; (2) a diagnosis of mechanical neck pain or cervicalgia by their primary care physician; (3) neck pain in situations of stretching, touching, movement, contraction against resistance, or after holding the same position for a period of time; (4) Visual Analog Scale (VAS) score equal to or greater than 50 mm [22]; and (5) asymmetrical lateral flexion of the neck of more than 5 degrees, as measured by clinimetric evaluation [23].
Exclusion criteria, were as follows: (1) neck pain resulting from cervical whiplash or direct traumatism in the neck area; (2) prior neck or shoulder surgery; (3) a medical diagnosis of fibromyalgia; (4) radiculopathy (i.e., acute sensory and motor symptoms in the innervated regions); (5) medical diagnosis of cervical osteoarthritis; (6) being involved in a legal suit; (7) to have received within the previous year, or to be currently receiving, physical therapy treatment, particularly with KT; (8) ongoing cervical pain for three months or more; and (9) allergies to any type of bandage or adhesive material.
Design
A single-blind randomized clinical trial with parallel design was conducted. Out of the 75 patients recruited from the accessible population, 45 met the selection criteria and were randomly assigned to one of three groups: Kinesio Taping group (KT) to receive real KT and conventional rehabilitation, with a mean age of 42.07 years (SD
This study was approved by the Ethical Committee for Clinical Research of the Medical Center in Toledo (Spain) and it complied with the guidelines of the Declaration of Helsinki and with current Spanish legislation for clinical trials. All participants signed consent forms after being debriefed and before their socio-demographic data were obtained. The final results of the study were reported to the patients in both groups.
Outcome measures
Dependent measures investigated in this study were pain intensity as primary outcome measure and range of motion of the cervical spine and quality of life as secondary outcomes. Data on pain and cervical range of motion were collected before treatment started (baseline measure), immediately after application of the first bandage, 24 hours later, on the fourth day of the protocol after bandage application, and at one month follow-up. Participants completed the quality of life questionnaire on two separate occasions: before beginning the treatment and at one-month follow-up.
Quality of life was measured using the Short Form 36 (SF-36) Health Survey in its Spanish version [24, 25]. It shows both high reliability and validity [26, 27, 28]. It consists of 36 items and 8 scales: Physical Function, Physical Role, Body Pain, General Health, Vitality, Social Behavior, Emotional Role and Mental Health. The scores range between 0 and 100.
The Visual Analog Scale (VAS) was used to assess pain intensity at each time-point [22]. In addition, pain across the day was also registered using this scale by recording their pain level at three different times each day: morning, afternoon, and night. The average value was calculated for further analyses. In order to test treatment effects, the mean values of the first two days and the last two days of treatment were calculated following the previous protocol. Minimal clinically important difference (MCID) ranges from 9 to 11 mm for this outcome [29]. This tool has demonstrated good psychometric properties in assessing pain intensity (ICC of 0.97 [95% CI
Cervical Range-of-Motion (CROM) was recorded by using an inclinometer (Cervical Range of Motion Device, Performance Attainment Associates, St. Paul
Manual therapy procedures during each session
Manual therapy procedures during each session
R: right; SMC: sternocleidomastoid muscle; L: left.
Finally, from the beginning through to completion of the physical therapy protocol, patients kept a simple record of their medication intake schedule, including times and drugs taken each day.
Following the protocol treatment of the Spanish hospital for neck pain, patients in all groups were instructed in postural hygiene recommendations and exercises for the cervical spine. The patients received written material on the postures and movements of daily life that might be harmful for the musculoskeletal system. In accordance with this protocol, the physical therapist teaches the patient, who is sitting on a stool, the key to holding an appropriate sitting position, while the patient is led towards a global neutral position of the spine for the next 5 minutes. The purpose is to align the lumbar, thoracic, scapular, and cervical portions of the spine, thus allowing the head to be positioned with minimum muscle exertion [30]. In the fifth treatment session, participants are taught various simple exercises to be performed four times per week at the rehabilitation service under supervision. They also receive written material detailing those exercises [31]. On the other hand, all patients across the three groups also received six 30-min sessions of manual therapy, which included the hands-on procedures described in Table 1 [32]. Patients were instructed not to perform exercises independently nor to receive other physiotherapy/medical treatments until full completion of the study (including follow up period).
Kinesio taping procedure
Following the first session of manual physical therapy, Cure Tape
(A) Kinesio Taping application in the cervical area. (B) Placebo procedure.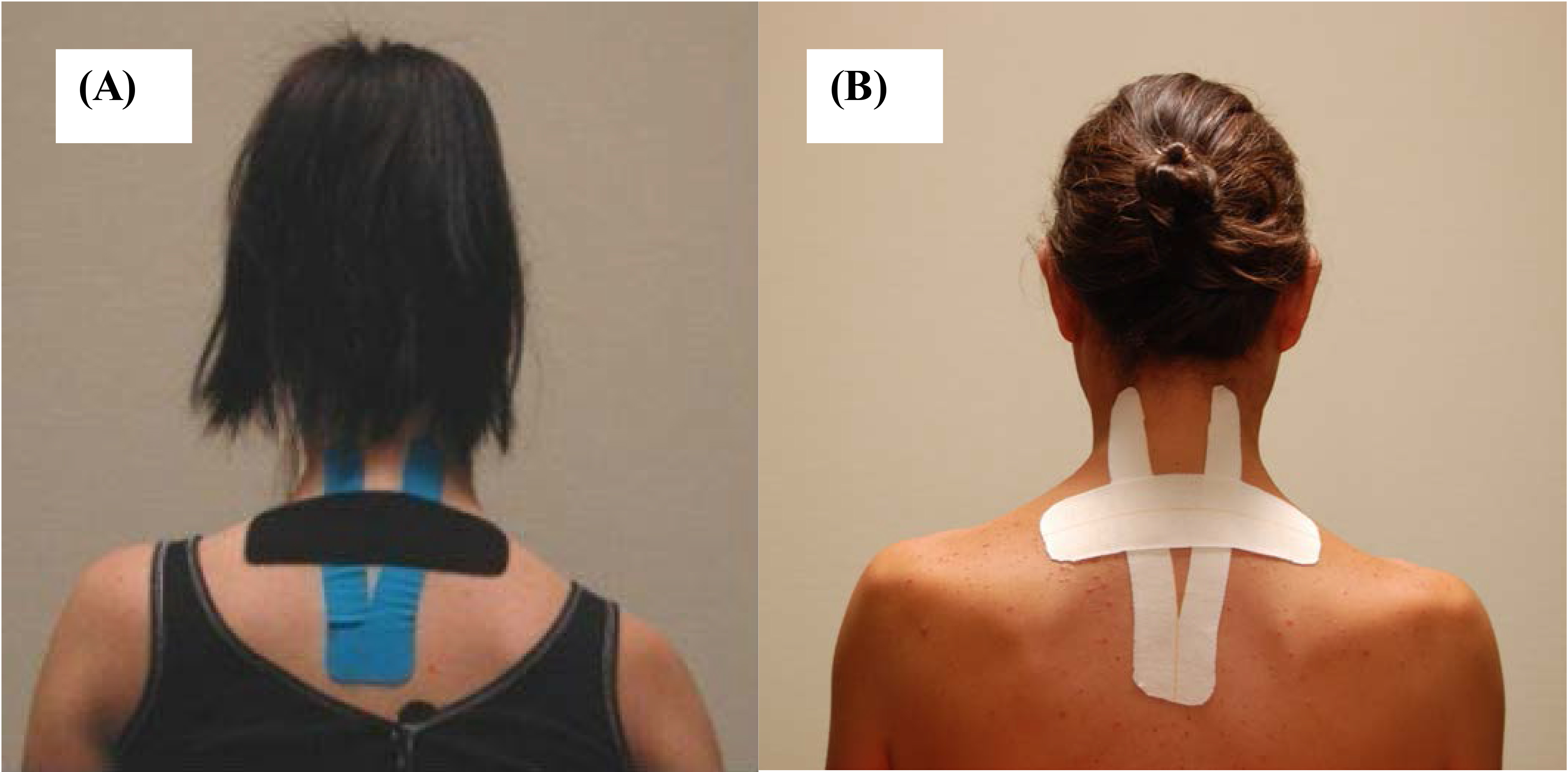
This group received two 5-cm Tensoplast
Flow chart of the recruitment of study participants, treatment protocol, and drop-out cases.
Descriptive statistics for baseline values of socio-demographic and clinical variables in the three study groups
Effect of intervention on the mean VAS score from baseline to one month follow-up. Error bars represent standard error (SE) of the mean. * Significant group * Time interaction (ANOVA, 
G*Power software, version 3.1.7 was used to calculate the sample size. According to this program a study using a sample of 15 patients per group can detect a high effect size (d
Results
Seventy-five people presenting with mechanical neck pain were assessed as potential participants. Of those, only 45 (36 females and 9 males) met inclusion criteria and were willing to participate in the study. Average age was 42.26 years (SD
The three groups were comparable in most socio-demographic, clinical, and quality-of-life variables (Table 2). With respect to mobility, the only significant difference (
Effectiveness of treatment on pain perception
In terms of the VAS scale, the Group * Time interaction for the 3
Similar results were achieved for pain across the day (no differences between groups), showing a similar reduction on this variable (3
Effectiveness of treatment on neck mobility
In order to test treatment effectiveness on neck mobility, we conducted separate Group * Time interaction 3
Effect of intervention on the mean flexion, extension, lateral flexion and rotation scores from baseline to one month follow-up. Error bars represent standard error (SE) of the mean. * Significant group * Time interaction (ANOVA, 
Repeated measures analyses demonstrated significant long-term improvements in neck flexion in all three treatment groups, when comparing range of flexion at baseline and at one-month follow-up, showing a large effect size: the KT group progressed from 47.3
Short-term and medium-term differences in neck flexion were also found in the P and CR groups. Specifically, the P group increased range of flexion from 41.3
No group x assessment time interaction was found in any of the SF-36 subscales, so it was not evidenced that conventional rehabilitation, either supplemented by KT or placebo bandaging, affected the quality of life of the participants, as measured by the SF-36 (
Prior to the start of treatment, 61.9% of the participants were medicated, while 38.1% were medication-free. Prescriptions by primary care physicians consisted of anti-inflammatory drugs (42%), muscle relaxants (4.8%), or a combination of anti-inflammatory drugs and muscle relaxants (14.3%). One week into the treatment, 14.3% of participants were medicated, while 85.7% were medication-free. There were no significant differences in medication reduction across treatment groups at any of the assessment times.
Discussion
In general, our results failed to show an additional effect of KT above and beyond those of conventional rehabilitation, as we obtained no significant differences across groups in most of the variables under study.
The most noticeable differences were obtained in terms of pain management in the Kinesio taping and placebo groups. These represented the largest effect sizes, and both were larger than the effect size found in the controls. This finding implies that a placebo effect could mediate in these interventions. Patients’ positive expectations towards therapy may induce endogenous opiate brain activation and produce an analgesic effect [33]. In addition, it is possible that patients change their behavior simply because they are taking part in the study, not because of the research treatment (Hawthorne effect) [34]. On the other hand, some authors have argued the use of a sham taping application as a real placebo because of the mechanical effect produced over de skin and consequently on the cervical range of motion. Perhaps the mechanical restraint supported by the taping gave the participants a greater awareness of the neck while moving and restricting painful movements, while Kinesio taping failed to provide an additional benefit [35].
In terms of neck mobility, all three groups showed improvements in all ranges of cervical motion. The only movement that varied across groups was cervical flexion. Immediately after the first treatment session, the KT group showed a 1.9
Our data are in agreement with those obtained in previous studies, which did not find statistically significant changes when using Kinesio Taping to prevent ankle lesions [40], to improve joint proprioception at the ankle [41], for maximum grip strength [42], spinal flexion [43], reflex response of the femoral biceps and external calf muscles [44], hamstring flexibility [45], neuromuscular performance of the femoral quadriceps [46, 47, 48], or the patellofemoral pain syndrome [49]. Other researchers who have obtained statistically significant differences when applying Kinesio Taping following cervical whiplash [20] or treating chronic low-back pain [14], ultimately considered that the degree of change was minimal and hardly significant at the clinical level. Our results indicate similar minimum differences. The relevance of this study, however, derives from the fact that it is the first investigation on the use of Kinesio Taping in neck pain in the context of primary medical care, which included placebo and control groups and followed the course of treatment throughout the one-week protocol period and at the one-month follow-up.
In summary, our results indicate a substantial effect of conventional rehabilitation (manual therapy and exercises) on pain perception, neck mobility, and quality of life, while they cast doubt on an added benefit provided by Kinesio Taping. A recent systematic review which screened 38 studies, has also pointed out that techniques such as mobilization and manual therapy (i.e. manipulation, clinical massage) are effective interventions for the management of neck pain. However, there is no evidence in favor of certain passive physical modalities such as electrotherapy or hydrothrepay [50]. Regarding exercises for mechanical neck disorders, as we included in the conventional protocol, evidence suggests its effectiveness, especially in those exercises aimed at strengthening the neck muscles and scapulothoracic/shoulder kinematics [51]. Analyzing scientific evidence, Miller et al. [52] have also stated that manual therapy and exercises provided long-term improvement in pain (Standardized Mean Difference (SMD)
The current study has a number of limitations that should be considered. Firstly, the study was designed as a single-blind trial, as the Kinesio Taping bandage needed to be applied by a physical therapist. Secondly, these results cannot be extrapolated to subjects under 18 or over 55 years of age, as that was the age range of study participants. Finally, a no-treatment control group was not included in the current study, so it cannot be established if the improvements noted in both groups are due to the interventions or simply to the passage of time.
Conclusions
Subjects suffering from neck pain who receive manual therapy, are instructed in a series of physical exercises, and given postural hygiene recommendations, experience a significant improvement in their level of pain, neck joint mobility, and quality of life. The addition of supplementary therapies such as Kinesio Taping does not appear to significantly affect clinical parameters.
Footnotes
Acknowledgments
The researchers thank all patients who participated in this study.
Conflict of interest
None to report.