
Abstract
BACKGROUND:
The prevalence of low back pain (LBP) in athletes across a variety of time frames and sports is not known.
OBJECTIVES:
To systematically collate and appraise studies on the prevalence of LBP in athletes and stratify by point, one year and life-time prevalence.
METHODS:
A comprehensive search was conducted in February 2016. The following sources were individually searched: PubMed (1950 to present), Ovid SP Medline (1950 to present), ISI (1982 to present) and Google Scholar; Surveys were included if they aimed to report the prevalence of LBP amongst the athletes. Two reviewers independently evaluated the methodological quality of the studies.
RESULTS:
The literature search generated 4379 records. Title and/or abstracts were reviewed by two investigators and full-texts of 201 relevant articles were selected for further evaluation. Studies were included if they reported the prevalence of LBP in an athletic population (any level of participation in sports and any age range) and were written in English. Furthermore, to adequately assess the prevalence rate, studies had to report the number of athletes with LBP as a percentage of the total number of athletes. Studies that did not contain necessary data to calculate prevalence rate including case reports and non-original studies were excluded and 41 studies entered the bias assessment step. A bias assessment was applied to the methodology of 41 studies, and 36 with low to moderate risk for bias were included in this review. LBP in athletes was shown to have a point prevalence ranging from 10% to 67%, a one-year prevalence ranging from 17% to 94%, and a life-time prevalence ranging from 33% to 84%. The highest prevalence of LBP was found among skiers, floorball players and rowers and the lowest were found in shooters, golfers and triathletes.
CONCLUSION:
Like general population, LBP is quite prevalent among athletes. There is a lack of sound data on the prevalence and mechanism of LBP in some popular sports such as volleyball, swimming and track and field. The lack of standardization of research methods and outcome measurement tools are significant problems in literature. Researchers need to use standard and internationally acceptable definitions for LBP and related functional disability. Investigators are encouraged to conduct epidemiologic studies, along with search for possible mechanism of LBP, by recruitment of large sample population of the athletes who are selected through randomization of the national population and adopt recent recommendations for a standard definition of LBP.
Introduction
Low back pain (LBP) is the most common musculoskeletal condition [1] with a lifetime prevalence of more than 80% [2] in the general population. There is also accumulating literature on the prevalence of LBP in athletes [3, 4]. However, prevalence studies on back pain in athletes can be problematic for several reasons. First is the failure to employing generally acceptable definitions of LBP [5, 6]. This includes the severity, location, and duration of pain that constitutes an episode of LBP [7, 8]. Second is the real potential for methodological flaws that result in bias in the target population [9, 10]. Recall bias and incomplete or poor response rate can clearly impact the quality of any prevalence study. Therefore, to the goal of this systematic review was to identify and collate studies on the prevalence of LBP among athletes, and to review the methodological quality of the relevant literature regarding the prevalence of LBP among athletes in different sports.
Methods
Protocol
Review protocol which is provided in following is based on PRISMA guideline.
Eligibility criteria
Studies were eligible if they reported the prevalence of LBP in an athletic population (any level of participation in sports and any age range) and were written in English.
The critical appraisal tool of the study [10]
The critical appraisal tool of the study [10]
Critical appraisal of epidemiological studies
Low risk of bias: further research is very unlikely to change our confidence in the estimate. Moderate risk of bias: further research is likely to have an important impact on our confidence in the estimate and may change the estimate. High risk of bias: further research is very likely to have an important impact on our confidence in the estimate and is likely to change the estimate.
A comprehensive search was conducted on February 2, 2016. PubMed (1950 to present), Ovid SP Medline (1950 to present), ISI (1982 to present) and Google Scholar were individually searched using specifically developed search strategies for epidemiological research. Keywords included: ‘back pain’ or ‘low back pain’ or ‘lumbar pain’ or ‘backache’ or ‘lumbago’ and ‘prevalence’ in combination with ‘sport’ or ‘athlete’ or the names of different sports including those listed by the International Olympic Committee [11]. Addition- ally, the cited references from the manuscripts were reviewed to identify additional articles that may have been missed by the initial search. Titles and abstracts of identified studies were scrutinized for relevance to the topic, and full text of selected studies were obtained for further evaluation. This study did not consider any specific definition for LBP as inclusion criteria. The point prevalence of LBP is considered as the number of athletes with LBP divide by the total number of athletes over the past 48 hours of study. The one year prevalence of LBP is considered as the number of athletes with LBP divide by the total number of athletes in the past year of study. The lifetime prevalence of LBP is considered as the number of athletes with LBP at any time in their lives divide by the total number of athletes in a study. This review considered athletes as individuals who have developed skills, physical stamina and strength to participate in sports. Studies with participants from all age range, any gender, and with any level of sports experiences were enrolled in the review.
Study selection (inclusion/exclusion criteria)
Studies were selected if they reported the prevalence of LBP in an athletic population and were written in English. Furthermore, to adequately assess the prevalence rate, the studies had to report the number of athletes with LBP as a percentage of the total number of athletes. Publications were excluded if they did not have data allowing for this percentage calculation. Additionally, manuscripts had to report the period of the measurement (e.g. point, one year, life time) to facilitate prevalence calculations. Studies that did not contain necessity data to calculate prevalence rate including case reports and non-original studies were excluded.
Data collection process (data extraction)
A data-extraction form was designed a priori, and a panel of 3 academic experts assessed its face validation. The same 2 reviewers (F.F. and M.R) independently in an unblinded standardized manner extracted data from each article using the data-extraction form. Disagreements were resolved in the same manner as for study inclusion. Where available, the prevalence of LBP by age group and gender was abstracted.
Risk of bias in individual studies
Using a previously standardized and reliable bias assessment tool (assessing risk of bias in prevalence studies provided by Hoy et al.) (Table 1) the external and
Summary of reviewed studies with low to moderate risk of bias
Summary of reviewed studies with low to moderate risk of bias
M: Male, F: Female, CS: Cross-Sectional, Pros: Prospective, eQ: electronic Questionnaire, PQ: Printed Questionnaire, HT: History Taking, Ex: Clinical Examination, CR: Completion Rate.
Flow diagram of study selection.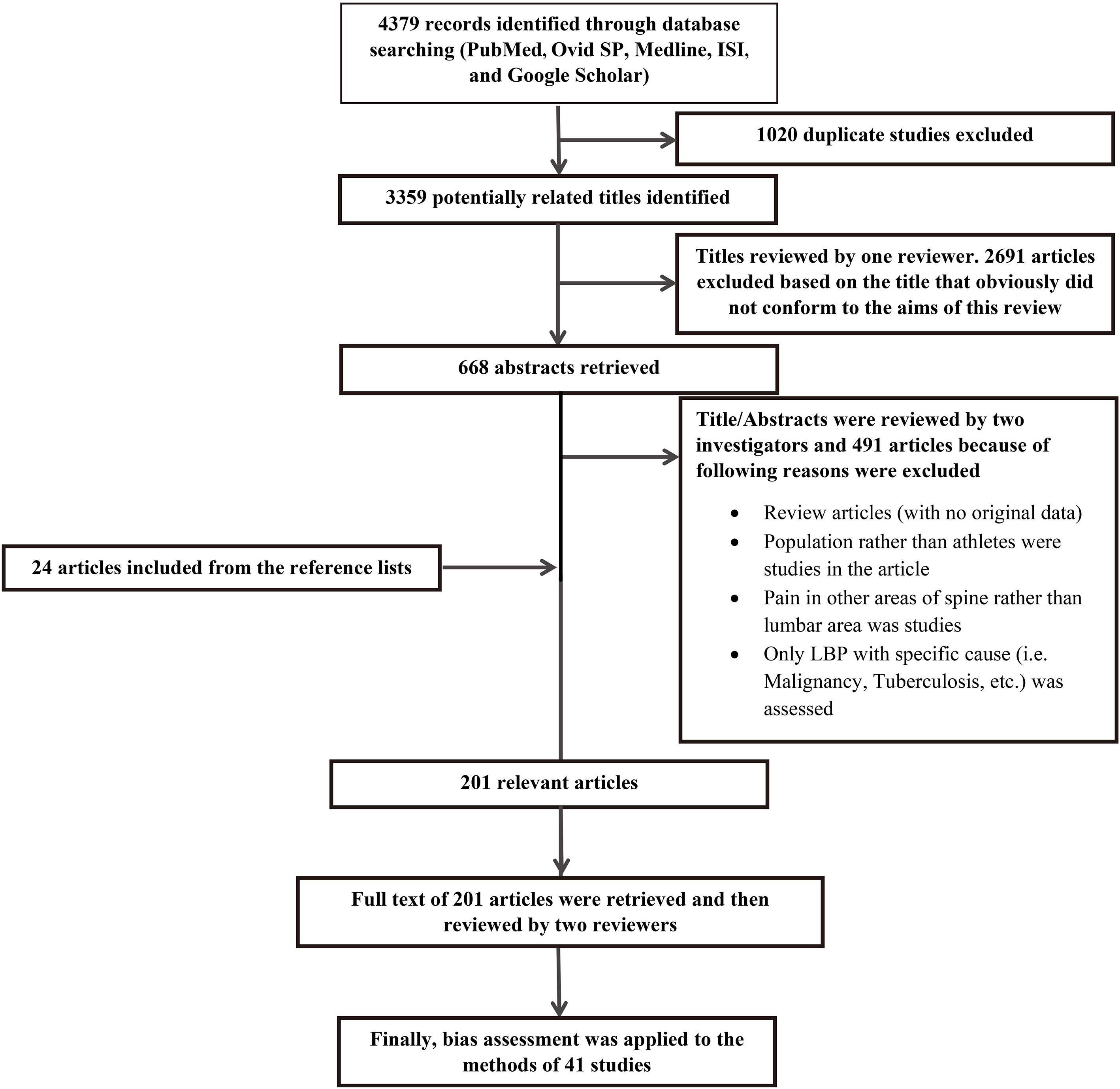
The rates of response to different questions of the quality assessment tool.
LBP definition of different studies with low to moderate risk of bias
NS: Not Stated.
LBP prevalence in different reviewed studies with low to moderate risk of bias
Wl: Weightlifting, TF: Track and Field, Wr: Wrestling, Or: Orienteering, IH: Ice-Hockey, Di: Diving, Ro: Rowing, Sk: Skiing, Fo: Football, Ha: Handball, SS: Speed Skating, Vo: Volleyball, Bb: Basketball, Fu: Futsal, Te: Tennis, Ba: Badminton, Sw: Swimming, Sh: Shooting, Ka: Karate, Fl: Floorball, F: Female, M: Male.
LBP point prevalence of different sports.
LBP one-year prevalence of different sports.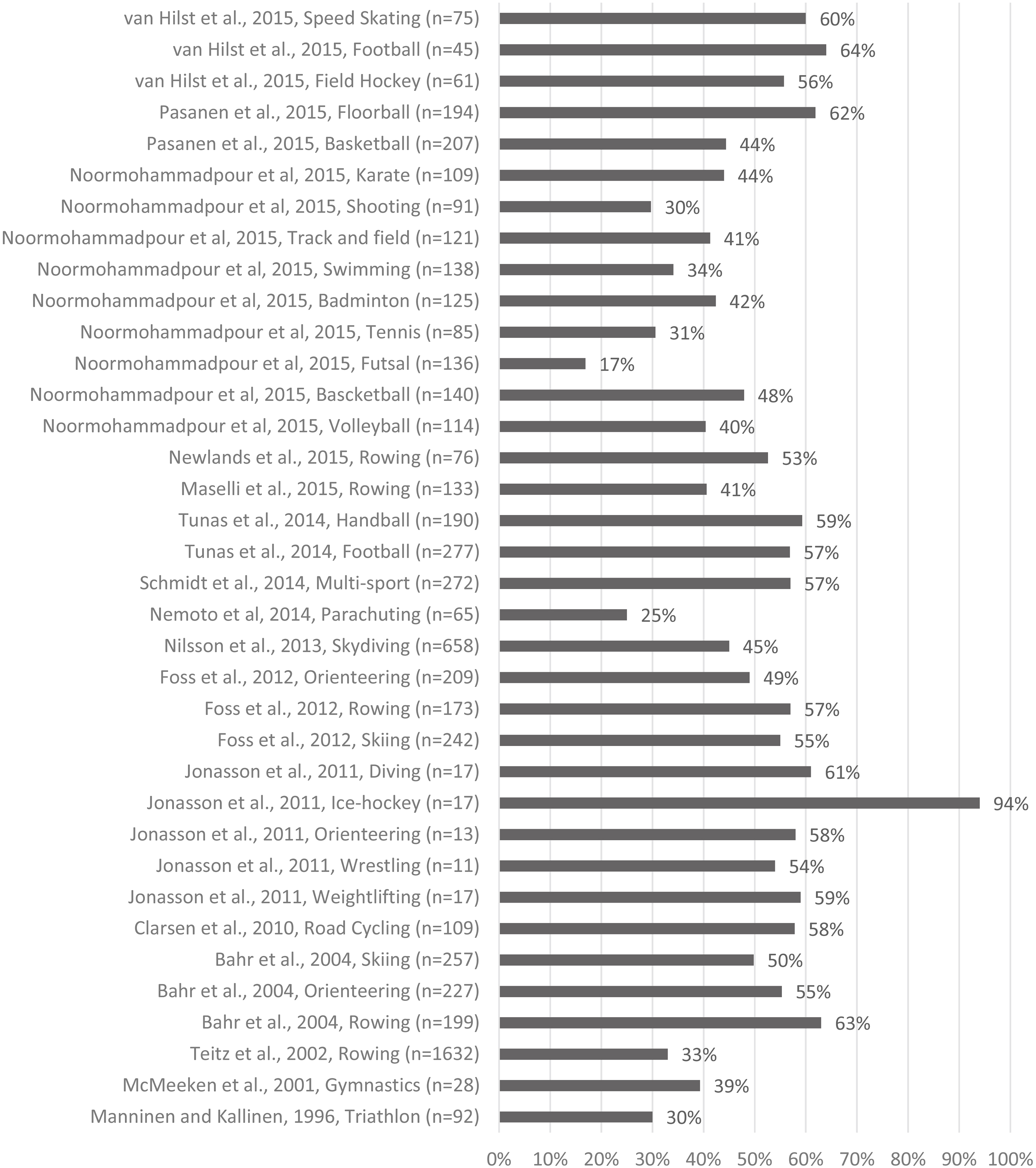
LBP life-time prevalence in different sports.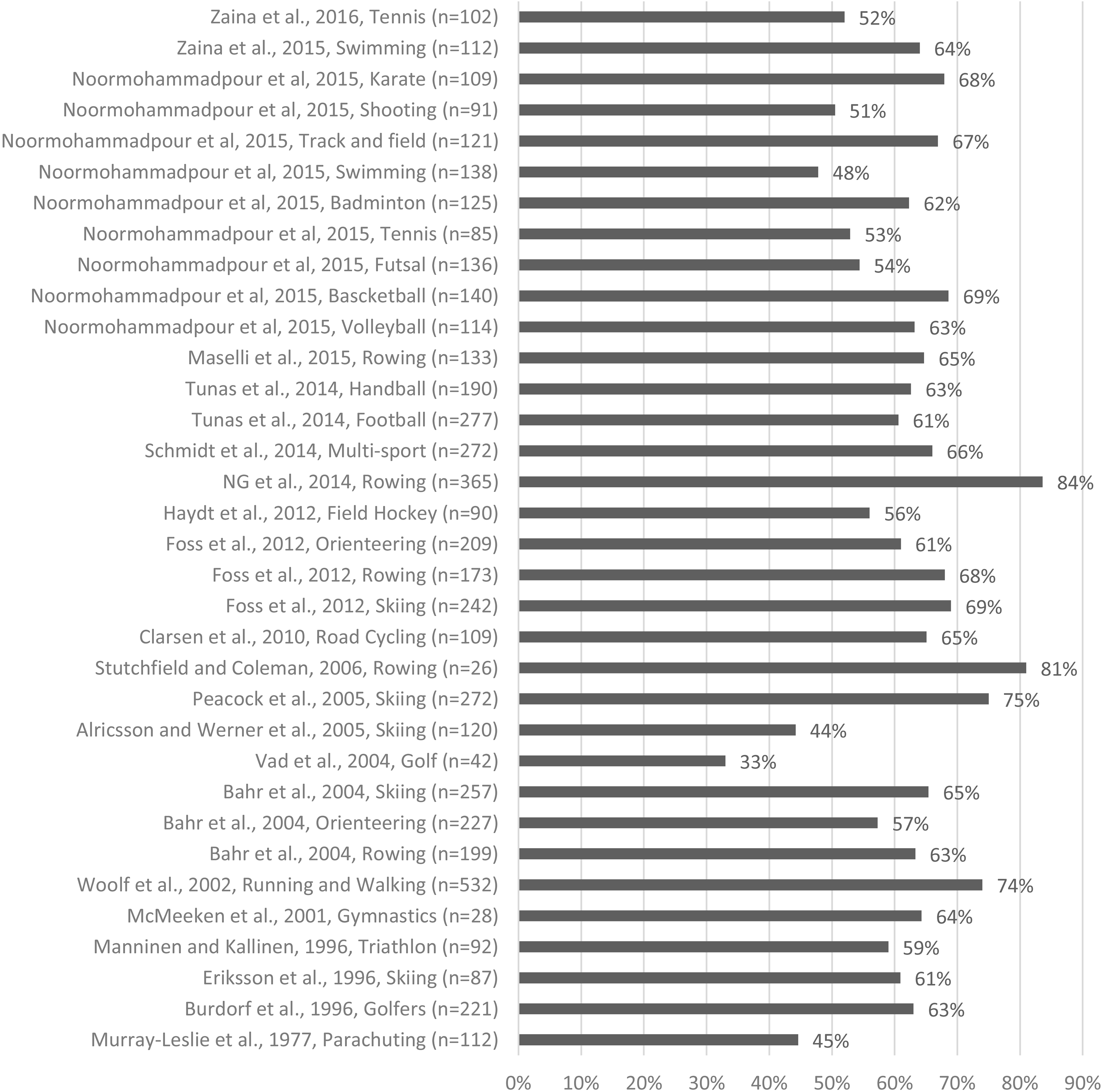
internal validity of the studies were assessed by two investigators [10]. In cases of uncertainty or disagreement between the investigators, it was resolved by discussion between the 2 reviewers. If no consensus could be reached, a third investigator reviewed the study to break the impasse. Based on the overall bias assessment score, articles were divided into low, moderate or high risk of bias. Study articles with high risk of bias were excluded. Data of papers with low to moderate risk of bias were included.
Figure 1 shows the flow diagram of the study selection [12, 13]. The literature search generated 4379 records. The titles and abstracts of these results were reviewed for relevance, further narrowing the results to 201 full-text articles for further review. Studies were included if they reported the prevalence of LBP in an athletic population and were written in English. Studies that did not contain necessity data to calculate prevalence rate including case reports and non-original studies were excluded. After applying the inclusion and exclusion criteria 41 manuscripts remained. A bias assessment was applied to these studies, resulting in (Tables 1 and 2 and Fig. 2) [4, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53] a total of 36 eligible epidemiological studies with low to moderate risk for bias were included in this review [4, 14, 15, 18, 19, 20, 23, 24, 25, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53]. Table 2 presents the methodological quality assessment of the publications. Figure 2 shows the bias rating for the studies, by each item of the risk assessment tool. Disagreements between the reviewers about the study selection and data extraction were primarily caused by differences in interpretation and were resolved in all cases. The primary inter-rater agreement for study inclusion (Kappa: 0.74) and data extraction was acceptable. Table 3 shows the study characteristics of the included publications.
LBP definition
Out of 36 studies included in this review, 10 studies (30%) failed to even state a definition for LBP in the publications (Table 4). Additionally several studies also did not use the internationally acceptable LBP definition for epidemiologic studies (e.g. the low back pain is a pain between the last rib and lower gluteal fold, which is bad enough to limit or change athletes’ daily routine or sports activities for more than 1 day) [6].
Back pain prevalence
Prevalence of LBP varied significantly between studies (Table 5) and sports. Additionally a wide variety of follow-up duration was reported across studies (Figs 3–5). The point prevalence of LBP among athletes has been reported to be between 10% to 67 % (Fig. 3) with the lowest point prevalence reported among shooting athletes [3] and the highest reported among skiers [27]. The one-year prevalence of LBP among athletes also varied widely (Fig. 4), with rates as low as 25% in parachuters [20, 41] and as high as 94% in ice-hockey players [37]. The reported life-time prevalence of LBP among athletes (Fig. 5) also ranged from 33% in golfers [29] to 83.6% in rowers [43]. The sample size of participants in the most of the studies was relatively low, while a high number of participants has been recommended for prevalence studies [48]. In the included manuscripts, three articles have more than 1000 participants [3, 24, 45], four articles studied from 500 to 1000 athletes [4, 25, 38, 40], and sample size in the remaining articles was less than 500 individuals.
Discussion
The results of this study revealed that similar to general population, the prevalence of LBP among athletes is high. The highest rate of point prevalence of LBP was found among skiers [27], floorball players [49] and rowers [43]. Extracted data showed that rowers also had the highest rate of life time prevalence [43] of LBP.
These findings are plausible given that skiing and floorball requires a flexed position of the back and frequent back twisting movements [19, 30, 49, 54, 55]. Regarding rowing, the repetitive cyclic flexion and high physical rotation loading of the spinal column [24, 43, 56] has been suggested as possible mechanism of LBP. In this review rowing and skiing were the most common studied sports. The combination of a high prevalence of LBP among skiers and rowers along with the published descriptive mechanisms of injury might explain a higher interest of epidemiologic researchers in these fields. Regarding the one-year prevalence of LBP, the highest rate was reported by Johansson et al. [37] who revealed that 18 out of 19 Swedish top ice-hockey players (94%) had LBP during the past year. Although the small sample size of the study and high frequency of dropouts limit the value of this study, the high prevalence of LBP among these athletes more highlights the importance of longstanding LBP in professional contact sports such as ice-hockey [37].
This review showed that the lowest rate of point prevalence (10%) was seen in shooters [3]. To our knowledge no previous study has studied LBP in shooters alone or comparing to general population. Surprisingly our review also showed that low rates of point prevalence of LBP were been reported among triathletes [20] and golfers [18] (12% and 13%, respectively). This finding is in line with the study by Vad et al. [29] which reported that only 33% of golfers experience LBP during the life time, which is lower than all other athletic groups and the general population [57]. Previous basic studies have shown that a golf swing generates significant rotational forces in the lumbar spine, which has led to many expert opinions regarding a high prevalence of LBP in golfers [58, 59, 60]. Low rates of point and life time prevalence of LBP among golfers from this review seems to contradict that thought process. It is not clear if golf is protective of LBP or if this result is due to a selection bias.
In this review, nearly one third of the studies (
Despite the increasing scientific evidence regarding the prevalence, mechanism and possible risk factors of LBP among athletes practicing different sports [64], the lack of standardization of research methods and outcome measurement tools continues to be a significant problem in assessing this literature [65]. To ensure that results of different LBP epidemiologic studies among athletes are comparable which is essential to increase the body of knowledge in this area, the researchers need to use standard and internationally acceptable definitions for LBP and related functional disability. Also reliable and validated sports specific LBP outcome measurement tools need to be used. Therefore, development of relevant outcome measurement tools such as sports specific quality of life and functional disability measurement tools seems quite necessary [65].
Assessment of LBP prevalence through medical records and public health registries might lead to underestimation of the number of subjects with back pain. Therefore, to ensure that results of different studies are comparable, data regarding the LBP status of athletes should be collected through a methodologically sound designed study and data should be collected directly by the researchers.
Another factor that might be considered in the interpretation of the prevalence of LBP among athletic population is the level of sport expertise and experience of subjects in different studies [5, 66]. While elite professional athletes commonly receive higher levels of medical care and health consult than general population, higher physical loads on these athletes, including repetitive compressive loading and high volume of training load without adequate recovery periods might increase the likelihood of elite athletes developing spinal overuse injuries and LBP [4, 67, 68, 69]. Accordingly, to increase the comparability of the study results, it seems quite logical to recommend researchers to measure the level of expertise and years of sports experience of athletes in period prevalence studies.
Limitations
Differences in age [1, 61], gender [1, 70, 71], hours of training per week [58, 72] and history of LBP [3] of the subjects recruited in studies are other factors which limit the possibility to compare the results of different studies. Unfortunately, because of mentioned diversity of pooled data, the data obtained from the studies included in this review is insufficient to ascertain the time trend of sports related LBP over the recent years. This finding could be beneficial for assessment of current preventive and therapeutic policies which already been established by international organizations. As another limitation in our review we excluded articles written in languages other than English due to lack of professional translator and having no access to non-English gray literature. Finally, this review did not compare the case selection, data gathering, outcome measures, and dropouts between selected and unselected studies.
Final recommendation
Our results show that the overall prevalence of LBP among athletes is high. There is a lack of sound data on the prevalence of LBP in some popular sports such as volleyball, swimming and track and field in the literature. With the increase in the sample size, standard error and random error decrease [48]; therefore, Investigators are encouraged to conduct epidemiologic studies by recruiting large sample population of athletes who are selected through randomization of the national population and adopt recent recommendations for a standard definition of low back pain.