
Abstract
BACKGROUND:
Nonspecific Chronic Low Back Pain (CLBP) is a condition difficult to treat due to multiple etiopathogenesis and there is wide consensus on the multidisciplinary approach. In physiotherapy, the Medium Frequencies (MF) diathermy has recently been introduced but without enough evidence of effectiveness.
OBJECTIVE:
To explore the effects of a deep heating therapy (DHT) produced by a MF diathermy for the treatment of CLBP compared with a superficial heating therapy (SHT). The study was a double blind randomized trial.
METHODS:
Forty-nine patients affected by CLBP were randomly subdivided in 2 groups and treated with either DHT (450 KHz) or SHT via electric resistance applying the same instrument on the lumbar spine. NRS (Numerical Rating Scale) for pain and ODI (Oswestry Disability Index) for disability were used as outcome measures. The follow up was: T1, 15 days (end of the therapy); T2, 30 days; T3, 45 days after T0.
RESULTS:
Both therapies were effective in reducing pain throughout the follow up with greater improvement in DHT group at T1. DHT resulted to have a higher efficacy with respect to SHT in reducing disability (ODI) throughout all follow ups.
CONCLUSION:
This study provides evidence of the positive effects of MF radio waves diathermy in the treatment of CLBP.
Background
Nonspecific low back pain (LBP) is one of the most diffused pathologies of the spine [1, 2]. Possible noninvasive treatments have been widely studied [3, 4] without any conclusive evidence on their efficacy. As far as chronic nonspecific low back pain (CLBP) is concerned, which refers to LBP lasting more than twelve weeks [5, 6], it is commonly believed that the best therapeutic approach should be multidisciplinary [3] due to a most probable mixed etiopathology of this condition [7, 8, 9]. Physical modalities have always been largely used for the treatment of CLBP, despite the low quality evidence of studies supporting them [3, 10]. Among these, ultrasound therapy seems to be beneficial in the short term, but not for CLBP [11, 12]. TENS is also not indicated in the management of CLBP [13] and so is LASER therapy [4, 15], while acupuncture has proven to be effective in combination with other therapies [16].
The use of heat is probably the oldest form of physiotherapy. Heat therapy can be delivered superficially (Superficial Heating Therapies, or SHT) with low direct penetration. There is some evidence that superficial heat therapy reduce pain and disability in the short term, in a mixed population of patients with acute and sub-acute LBP and that the combination with physical exercise can improve its efficacy [17]. In addition, heat can be dispensed deeply, employing instruments able to transfer it in depth, such as ultrasound and, particularly, radio waves (Deep Heating Therapies, or DHT). Radio waves diathermy is largely used in the treatment of CLBP [18], although with very different modalities [19, 20, 21, 22]. Discovered at the beginning of the 1900s, in the last fifty years radio waves diathermy was mostly performed with High Frequency (HF) waves (27 MHz); then, with Ultra High Frequency (UHF) waves (2.45 GHz, 433–920 MHz) and more recently, with Medium Frequency (MF) waves (450–1000 KHz). This latter has the advantage of a greater tissue-penetration and a better localization of energy in the target area [23].
Despite the rapid and wide diffusion of the new MF waves therapy, in our knowledge no studies are available, in particular on spine pathologies, where it is one of the most used therapies. A few studies on different radio waves diathermy (UHF and HF) can be found in literature [19, 20, 21, 22] without agreement on findings.
The aim of the present study was to evaluate the efficacy of a diathermy treatment with MF radio waves for nonspecific CLBP. For this purpose, this treatment has been compared with a superficial heat delivered by an electric resistance. Already in the past phantom models demonstrated that the thermal gradient induced by a thermal applicator, like the one used as control in the present study, is very steep and limited to few millimeter in depth and that the temperature rise is negligible [24, 25].
In the present trial the two sources of heat have been emitted separately and alternately by the same instrument, with the use of a software able to automatically generate either type of heat treatment (blind and random) and, consequently, create the-two well distinct groups.
The hypothesis is that the greater penetration of MF radio waves in the tissues would be more effective in the treatment of nonspecific CLBP compared to superficial heat.
Methods
This Phase IV study has been approved by the local Ethics Committee (Protocol n. 0.005.787-13/02/2014).
Study designs and participants
A total of 63 CLBP patients attending the Physio- therapy Unit of our Institute were screened (34 females and 29 males). Fifty eligible patients based on the inclusion criteria, and who voluntarily agreed to participate in the study, were enrolled. One patient dropped out for personal reasons; therefore 49 patients completed the study: 26 females and 23 males, with a mean age of 60 years (SD 11.1) and a mean Body Mass Index (BMI) of 25.9 (SD 3.5) (Fig. 1).
Flowchart of the experimental study. CLBP: Chronic Low Back Pain. DHT: Deep Heating Therapy (consisting in radio waves 450 KHz diathermy). SHT: Superficial Heating Therapy (consisting in electric resistance heating).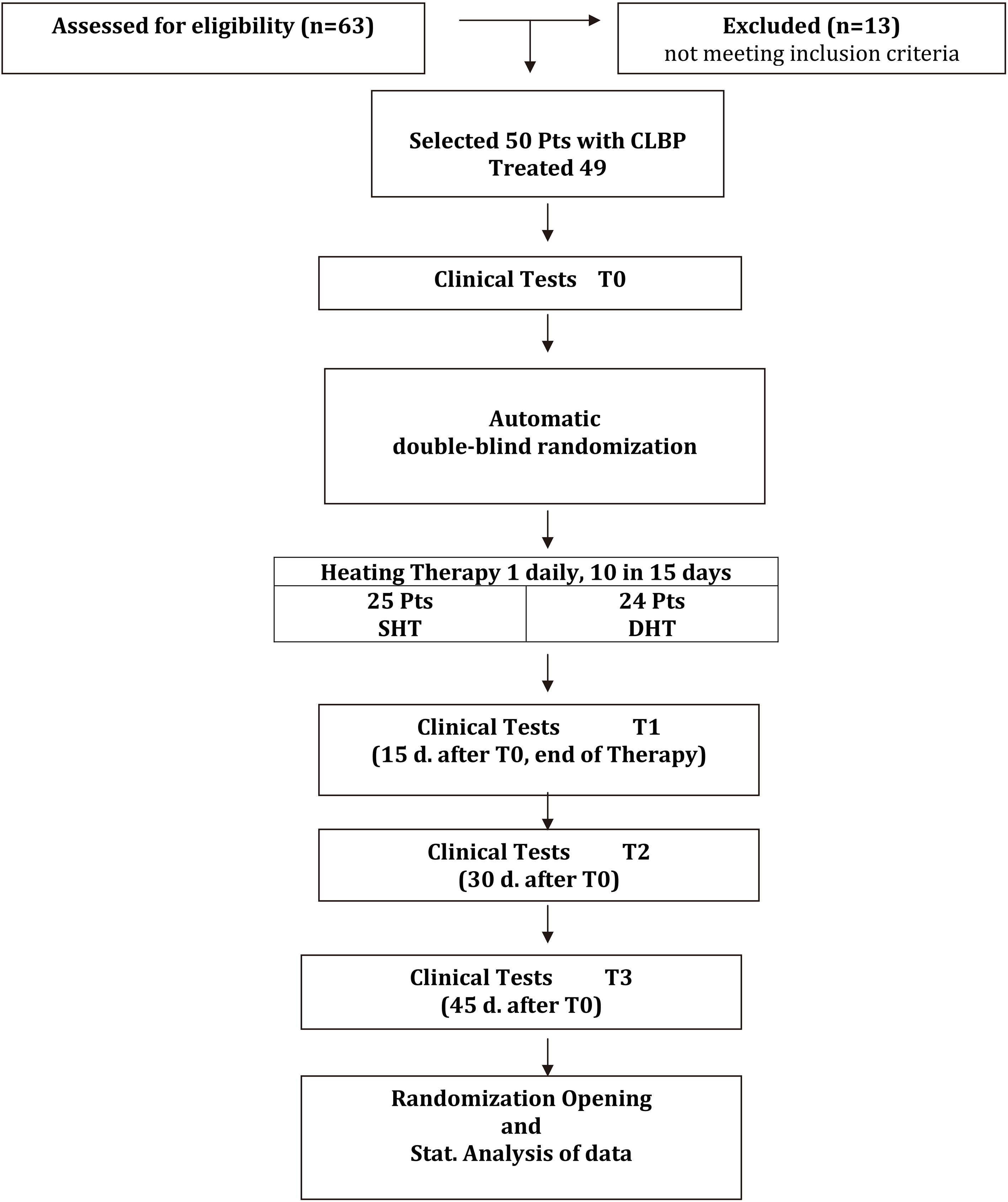
Schematic representation of the DHT/SHT system. The experimental hand-held delivery device (Active Electrode) is able to emit both DHT and SHT. DHT mode: the radiofrequency (MF 450 KHz) is working and the resistance is not connected. SHT mode: the radiofrequency is not working and the electric resistance is connected.
Patients with nonspecific CLBP (more than 12 weeks) localized below the scapulae (shoulder blade) and above the cleft of the buttocks without any specific cause detectable (e.g. infection, neoplasm, metastasis, rheumatoid arthritis, fracture or inflammatory process).
Exclusion criteria
Patients affected by the following conditions were excluded from the study: recent vertebral trauma; pain caused by major rheumatic diseases affecting connective tissue, or inflammatory conditions. Patients with dermatitis or with skin local lesions; with medical history of neurological diseases caused by altered heat-pain perception (central or peripheral paralysis of the nervous system); with any type of pace-maker; with local metal implants, such as articular prosthesis, or other materials that could concentrate the electromagnetic field lines. Patients with malignancies; taking opiates, major analgesics or corticosteroids drugs. Patients who had undergone previous physical radio waves diathermy or other hypertermic therapies in the last 3 months.
Informed consensus
All patients who participated to the trial were informed about the content of the study and signed the informed consent form.
Randomization
The type of therapy, DHT or SHT, was chosen by the device according to a random numeric sequence elaborated before the start of the study by Emildue
DHT group: 24 patients were treated with heat therapy delivered by induction via the transit of radio-frequency in the human body. SHT group: 25 patients were treated with heat therapy delivered by the electric resistance.
The instrument used in the study was an experimental device, specifically set up for the trial by Emildue
Deep Heating Therapy (DHT) system was based on the emission of MF radio waves, frequency
The treatment was released to the patient using two electrodes: an active electrode and a return one; biological tissues interposed between the electrodes were heated because they represented the dielectric of the system. The active electrode was of circular shape, with a diameter of 7 cm. The return plate was a 20
Superficial Heating Therapy (SHT) system; in this mode the heat was generated by an electric resistance (maximal power of 150 W), using the same exit of the radio frequency. The resistance, applied to the active electrode, was not visible from the outside.
When the electric resistance was running (SHT mode), the radio waves emission was automatically switch off. On the contrary, when the unit was working in DHT mode, the heat was only generated by the emission of radio waves while the electrical resistance was disconnected. However, in both treatments the patient always felt a temperature increase under the active electrode (Fig. 2).
Mode of treatment
The same graduate physical therapist (LC) always delivered the treatment in outpatient clinics regimen, according to the following scheme: 1 treatment of 20 minutes per day, for 10 in 15 days.
Position
The patient was set in prone position with the elec- tric return plate under the abdomen and the active plate on the back. The entire treatment was performed with the use of a conductive cream to allow the right transfer of energy to the patient.
The same timing of fixed and moving electrode phases was used in both DHT and SHT groups.
For analgesic purposes the occasional use of Paracetamol 1 g/day max 3 times per week was tolerated.
Outcome measures
The primary endpoint was pain reduction in patients with CLBP and the secondary endpoint was the evaluation of the disability caused by this condition. For this purpose the Numerical Rating Scale (NRS) for quantitative measurement of pain (score 0–10) [25] and the Oswestry Disability Index (ODI) for disability [26, 27] were used respectively.
All tests were carried out by the same physiatrist (AZ) at the following time points: T0: before treatment (baseline); T1: 15 days after T0 (at the end of the therapy); T2: 30 days after T0; T3: 45 days after T0 (Fig. 1).
Statistical analysis
Determination of study sample size: the following assumptions were made for calculation of valid sample size: level of significance (
For each group of the study mean and standard deviation were calculated. Difference within each group were evaluated by Anova repeated measures and post hoc pairwise analysis with Sidak correction for multiple comparisons, at follow up T0, T1, T2 and T3. Age and BMI were normally distributed according to the Kolmogorov Smirnov but their variance was not homogeneous by the Levene test so they were analyzed by Mann Whitney test. Sex was analyzed by Pearson’s chi-squared test, evaluated by exact method.
General data of patients
General data of patients
DHT: Deep Heating Therapy (radio waves 450 KHz diathermy). SHT: Superficial Heating Therapy (electric resistance heating). BMI: Body Mass Index. NRS: Numerical Rating Scale of pain. ODI: Oswestry Disability Index.
The analysis between the two groups for NRS and ODI was carried out by means of the Mann Whitney test on percent Delta along the follow up. Cohen’s d was calculated to evaluate the effect size [28].
All statistical analyses were considered significant for
Trend of NRS values in DHT (continuous line) and SHT (dotted line) groups. NRS: Numerical Rating Scale of pain. DHT: Deep Heating Therapy (450 KHz diathermy). SHT: Superficial Heating Therapy (electric resistance heating). CI 
Trend of ODI values in DHT (continuous line) and SHT (dotted line) groups. ODI: Oswestry Disability Index. DHT: Deep Heating Therapy (450 KHz diathermy). SHT: Superficial Heating Therapy (electric resistance heating). CI 
The two groups were homogeneous at baseline (T0) for age, BMI and sex, although a slight prevalence of female patients was present in the DHT Group. Both NRS and ODI values were not statistically different at baseline (Table 1).
Forty nine patients completed the study; tolerance to therapy was very good in both groups: adherence was 100% and none of the patients missed a treatment session; all patients were subjected to the scheduled tests up to 45 days. None of the patients took the rescue therapy during the study.
NRS
Analysis by separated groups
Repeated measures ANOVA was significant for both groups (
Outcome measures along the follow ups within the groups: Anova test and post-hoc analysis
Outcome measures along the follow ups within the groups: Anova test and post-hoc analysis
DHT: Deep Heating Therapy (radio waves 450 KHz diathermy). SHT: Superficial Heating Therapy (electric resistance heating). NRS: Numerical Rating Scale of pain. ODI: Oswestry Disability Index.
Comparison between groups: percent delta along follow up
DHT: Deep Heating Therapy (radio waves 450 KHz diathermy). SHT: Superficial Heating Therapy (electric resistance heating). NRS: Numerical Rating Scale of pain.
At post-hoc analysis both groups registered a significant decrease of NRS at T1 (
Comparison between groups showed a significant difference (percent delta) at T1 (
ODI
Analysis by separated groups
Repeated measures ANOVA was significant for bothgroups (respectively
Post-hoc analysis showed a significant difference of ODI at T1 with respect to baseline only in DHT Group (
Analysis between groups
In the comparison between groups, percent delta values were significantly different in favor of the DHT group throughout the follow up (respectively T1:
Discussion
In the present study both DHT and SHT demonstrated to be effective in reducing nonspecific CLBP. DHT, with MF radio waves, allowed better result than SHT in improving disability. The best result obtained with MF radio waves heat therapy (DHT) confirms the hypothesis of the present work that the greater penetration of MF radio waves in the tissues is more effective compared to superficial heat.
Actually, all superficial heating therapies are essentially based on the release of infrared radiations that can reach deep tissues only indirectly, by conduction from surrounding tissues or by convection via blood circulation [24]. It can be deduced that treating a biological target (in this case the lumbar spine and deep soft tissues) with a direct form of energy, can have some therapeutic advantage. This seems to support the role of mechanical causes (inter-vertebral disk, articular facets, sacral-iliac articulations pathologies and muscle diseases) compared to neurological and psycho-social causes in nonspecific chronic LBP [8, 29, 30, 31, 32].
These considerations are confirmed by the Oswestry Disability Index, demonstrating a constant and notable decrease of disability in the DHT group from one follow-up to the next, approaching in time to minimal levels of disability, corresponding to a value below 20% [26]. It is very likely that the reduced disability obtained by DHT group is a direct consequence of the effect of diathermy on extensibility of deep tissue, as already demonstrated by other authors, in different body districts as shoulder, ankle and knee [33, 34, 35], although using other types of radio waves (HF and UHF).
Among previous studies on the use of radio waves diathermy, we found conflicting results. Shakoor et al. [22] performed a study on CLBP comparing a therapy based on the combination of short waves (HF) and NSAIDs to a therapy based on the combination of sham short waves and NSAIDs. The frequency used in their study (27.12 MHz) was relatively close to the MF band of our trial (450 KHz). The authors found a statistically significant difference in favor of the treatment with HF waves compared to the sham treatment at 3 weeks after the end of the trial. Unfortunately, despite leading to results very similar to ours, this study was not a true double blind because the sham instrument did not produce heat.
Durmus et al. [20] carried out a trial in CLBP using tests very similar to those used in the present study (VAS and ODI) and a protocol based on a combination of microwaves (UHF: 2.45 GHz) and exercises, compared to a group performing only exercises. The study, which was randomized but not a double blind, did not show significant differences between the groups.
Akyol et al. [36] used the radio waves (HF: 27.12 MHz) and physical exercise in a group of knee osteoarthritis (OA) patients, compared to a sham diathermic treatment and physical exercise, without a significant improvement in pain and disability. The authors used a very complex double blind design: in order to confuse the heat sensation of diathermic and sham treatment, both groups of patients were pre-treated with hot pack.
A similar double blind method was used by Leung and Cheing [33] in the treatment of frozen shoulder, with a better result in the diathermic group.
Rabini et al. [35] carried out a clinical double blind study on knee OA, comparing a DHT treatment to a SHT treatment. The authors, in the group DHT, used a diathermic device delivering microwaves (UHF: 434 MHz); in the SHT group he used the same hyperthermia device, kept warm at 38
One of the strongest points of the present study with respect to previous literature is the double blind design, achieved by a computerized system applied to the device to provide both DHT and SHT. We believe this has been an important step toward a real randomization. It is in fact well known that is quite difficult to have a real double blind setting in physiotherapy clinical studies. Furthermore, the reported studies never used MF radio waves. For these reasons our trial is unique and not comparable to other studies performed in the past.
Another important aspect is the absence of a considerable drop-out rate from the study (one patient declined to participate to the study for family problems), demonstrating that heat is a form a physiotherapy well tolerated by patients with CLBP and chronic disability.
Given the widespread diffusion of CLBP in the population, the main limitation of the study was the small number of patients (
In conclusion, with the numbers of the present study, the Deep Heating Therapy, based on targeted MF waves diathermy, seems to be effective in the treatment of nonspecific CLBP, and could be considered for the multidisciplinary management of this complex pathology.
Footnotes
Acknowledgments
The study was supported by Emildue
Conflict of interest
None to report.