
Abstract
BACKGROUND:
Algometry, as a highly sensitive method, provides an objective insight into the degree of pain, while the use of questionnaires can estimate the patient’s psychological status in a simple way.
OBJECTIVE:
This study was conducted in order to measure the pressure pain threshold in patients with cervical and lumbar radiculopathy and to find a possible association of pain with the anxiety and depression.
METHODS:
The study examined 60 hospitalized patients with cervical radiculopathy and 60 patients with lumbar radiculopathy before starting and after finishing kinesitherapy. The research was conducted using the digital algometry device and Hospital Anxiety and Depression Scale.
RESULTS:
There was no statistically significant difference in algometric values between the patients with cervical radiculopathy and the patients with lumbar radiculopathy. The program of rehabilitation did not lead to significant improvement in the level of pain. Females have a lower pressure pain threshold than males. Psychological factors greatly affect the pain.
CONCLUSIONS:
The applied methods will provide the implementation of appropriate therapy and would achieve better verification of the results in a rehabilitation program. Radiculopathy in conservative therapy should be treated in cervical-thoracic and lumbar region together. Rehabilitation period for patients with radiculopathy have to be longer.
Introduction
Radiculopathy represents a disease involving compression and/or irritation of the spinal roots or the trunk of the spinal nerve. The compression of spinal roots could be caused by various reasons, but it is most often caused by a disc herniation, spondylosis, or thickening of the surrounding ligaments [1]. Radiculopathy can be diagnosed at any part of the spine, but the lumbar and cervical radiculopathy are more often present than radiculopathy of thoracic spine. The incidence of lumbar radiculopathy in the population ranges from 9.9 to 25%, while the incidence of cervical radiculopathy is much lower, ranging from 1–9% [2]. Spinal nerve roots in osteofibrotic space leave the dural sac to the lateral edge of the intervertebral foramina. The length of this epidural space grows from L3 to S1 vertebra, making the roots of L5 and S1 of the spinal nerve more susceptible to compression [3].
The symptoms that occur in patients with radiculopathy depend on the level at which the affected nerve roots are located and they include pain and/or sensory-motor deficits with possible reflexes damage which are followed by segmental distribution. Therefore, the condition of radiculopathy may not necessarily be associated with pain, but in most patients, the pain is the initial symptom [4]. Most often the symptoms occur at the same side of the body where the affected nerve structures are located.
Chronic radicular pain causes a decrease in the quality of life with the loss of work and social skills. A recent epidemiological study emphasizes the relationship between the pain in the lower back and the neck pain in adults [5]. Studies showed that lower pain threshold is exhibited by the patients with the pain in the neck and shoulder muscles compared to healthy subjects [6].
An abnormal sensitivity to touch or pressure is one of the most common signs of musculoskeletal dysfunction and chronic pain, and the quantitative way to measure the muscle susceptibility is algometric testing of pressure pain threshold (PPT). Algometric testing is recommended as a diagnostic tool and as a means to evaluate the effects of different treatments aimed at pain relief (physical therapy, injections and medicaments) [7]. The pressure pain threshold is usually tested on the back of the neck and shoulders on the trapezius, levator scapulae, splenius capitis and supraspinatus muscle. The most common sites for testing pain threshold in the lower back are on the erector spinae, quadratus lumborum, iliopsoas, and gluteus medius muscle [6].
The pain threshold is determined by the degree of inflammation and/or trauma, accompanying stress and subjective impression, i.e. affective and behavioral response to pain. These factors may cause sensitization of the peripheral nociceptors in the affected area [8]. Psychological factors (e.g. anxiety and depression) determine the type of reaction to a painful experience and the ability of a person to cope with the pain, but they also affect the evolution of the symptoms of chronic pain [9].
Anxiety and depression in patients with radicular pain can be detected using specific questionnaires and scales. It is recommended to use validated questionnaires for anxiety and depression, because of the better understanding of present conditions compared to the assessment of the therapist [10].
The data from the literature indicate that the PPT is lower in the neck than in the lower part of the back and that exercises within the rehabilitation program significantly reduce the pain in patients with radiculopathy [11, 12]. Also, women have in general lower PPT compared to men [13].
The hypothesis of the study: pain intensity caused by pressure on the examined point is significantly higher in patients with cervical radiculopathy compared to patients with lumbar radiculopathy; there is a significant difference in perception of pain in patients with cervical and lumbar radiculopathy before and after kinesitherapy; there is a significantly lower PPT in female patients with radiculopathy compared to male patients with radiculopathy; pain has a significant adverse effect on psychological factors (anxiety and depression) in patients with cervical and lumbar radiculopathy. This study was designed to determine the PPT in patients with cervical and lumbar radiculopathy and to assess pain coherence with psychological factors (anxiety and depression). The results obtained from the present study could help in designing better therapeutic programs in the rehabilitation of patients with radiculopathy.
Methods
This research was conducted as a prospective study with hospitalized patients, in the period from December 2015 to September 2016, at the Clinic for Medical Rehabilitation, Clinical Center of Vojvodina, Novi Sad, Serbia.
Participants
The study included 60 patients diagnosed with cervical radiculopathy (30 males and 30 females) and 60 patients diagnosed with lumbar radiculopathy (30 males and 30 females). The subjects’ age ranged from 29 to 78 years of age, mean age being 55.58.
Inclusion criteria: All patients with lumbar and cervical radiculopathy only had exercise (kinesitherapy) as a prescribed therapy. Only patients with magnetic resonance imaging (MRI) findings of radiculopathy were selected for the study. Exclusion criteria: The study did not include patients who received the medicaments from the group of analgesics, anti-depressants or benzodiazepines, and patients who had had injury or surgical treatment in any segment of the spinal column over the past year, in order to eliminate the impact of such a therapy and obtain objective results of the pain level and psychological status. Pregnant women were also not included in our study.
Procedure
The pressure pain threshold was determined on specified points using an algometer while the patient was lying on the stomach (without clothes on the target points). Algometric values were noted on a form which contained the basic demographic data of the patient (name, sex, age), and the details about the diagnosis obtained from the history of the disease (the level of radiculopathy and the side of the body with pathological changes, verified by the MRI). The pressure pain thresholds were analyzed at five points bilaterally at the cervical region and the five points bilaterally in the lumbar region in each patient (Fig. 1).
Points for algometric examination. Cervical region: 1- suboccipital point (2 cm lateral to the spinous process of axis), 2- splenius capitis, 3- upper part of trapezius, 4- levator scapulae (2 cm above the lower insertion located in the upper medial border of the scapulae), 5- middle part of trapezius; Lumbar region: 6- 2 cm lateral to the first lumbar vertebra, 7- 5 cm lateral to the first lumbar vertebra, 8- 2 cm lateral to the third lumbar vertebra, 9- 5 cm lateral to the third lumbar vertebra, 10- 2 cm lateral to the fifth lumbar vertebra.
Algometry was carried out with the Wagner Instruments digital algometer (United States, 2007). The algometer has a plunger with rubber probe, which is applied on the area of one square centimeter (cm
The psychological status was established using Hospital Anxiety and Depression Scale (HADS) [15]. The applied HADS consists of 14 questions used to measure the emotional stress of the patient, thereof 7 questions assess the degree of anxiety (HADS-A), and 7 questions estimate the degree of depression (HADS-D). Each question offers 4 answers, ranging from asymptomatic (0 point) to the maximum presence of symptoms of distress (3 points). The questions for anxiety and depression are alternately arranged, and the total score for HADS-A or HADS-D is the point summation of all 7 questions. According to the scores, the level of patient anxiety and depression was classified to one of three categories: “normal” (0–7 points), “borderline” (8–10 points), and “abnormal” (11–21 points). The questionnaire was designed to determine the possible states of anxiety and/or depression within the medical institutions, excluding a psychiatric hospital.
The duration of the treatment cycle was an average of 14–21 days. Algometric and psychological examinations were carried out before the treatment cycle (when a patient arrives in a clinic) and one month after finishing the treatment cycle (discharge from clinic) in the control examination.
Software Statistical Package for Social Sciences – SPSS 21 was used for statistical analysis of the data. Numeric features are represented by mean values (arithmetic mean) and the measure of variability (range of values, standard deviation), and attribute marks using frequencies and percentages. A comparison of the value of numerical features between the two groups was performed using Student’s t-test, while the non-parametric Wilcoxon test was applied to compare the values between three or more data sets. Testing the difference in the frequency of the attribute features was done using the
The independent Ethics Committee of the Faculty of Medicine, Novi Sad, approved the study.
Algometric values on the left side of the body of the patients with cervical and lumbar radiculopathy before starting treatment (PPTL – pressure pain threshold on the left side of the body).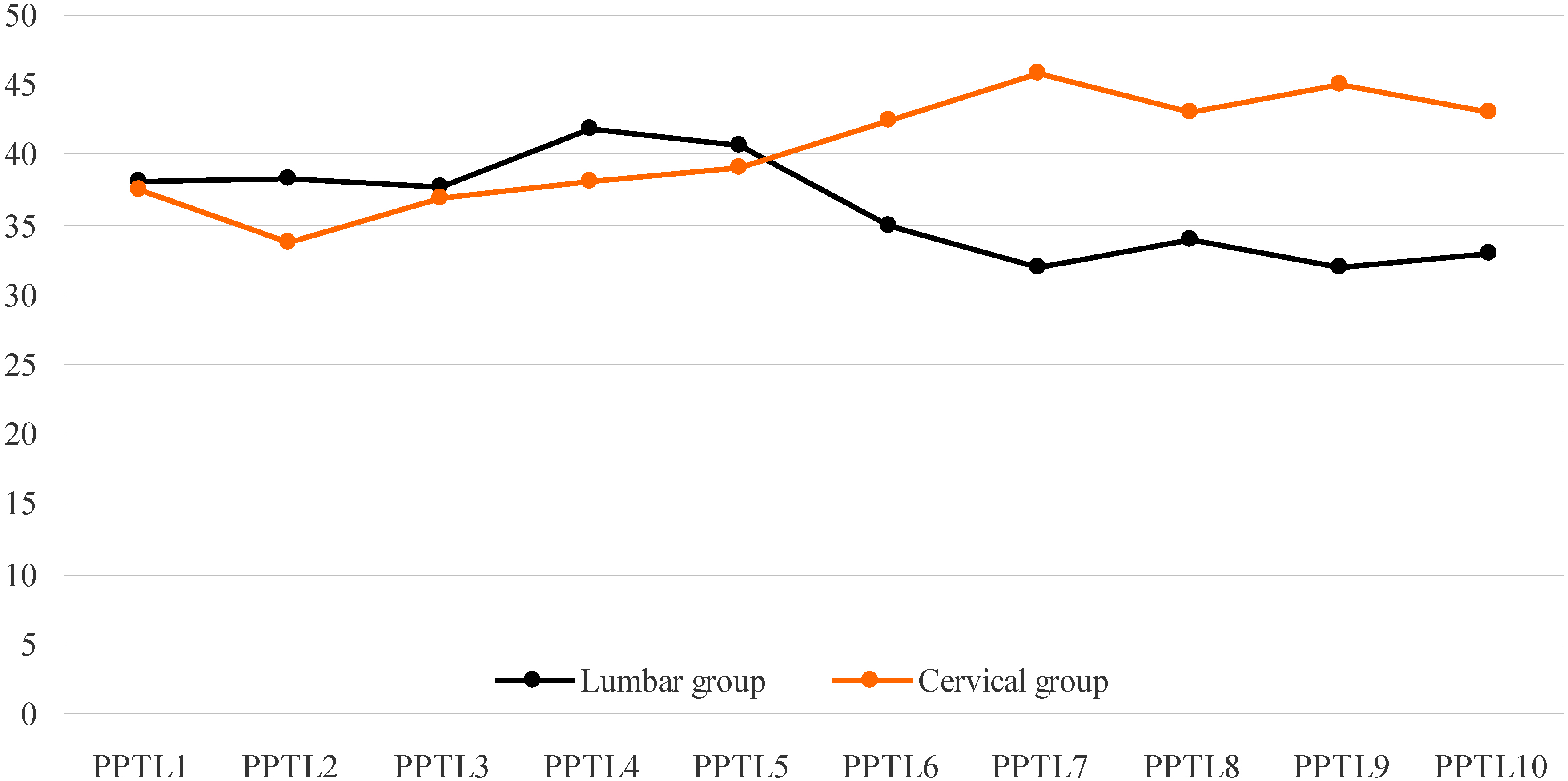
Algometric values on the right side of the body of the patients with cervical and lumbar radiculopathy before starting treatment (PPTR – pressure pain threshold on the right side of the body).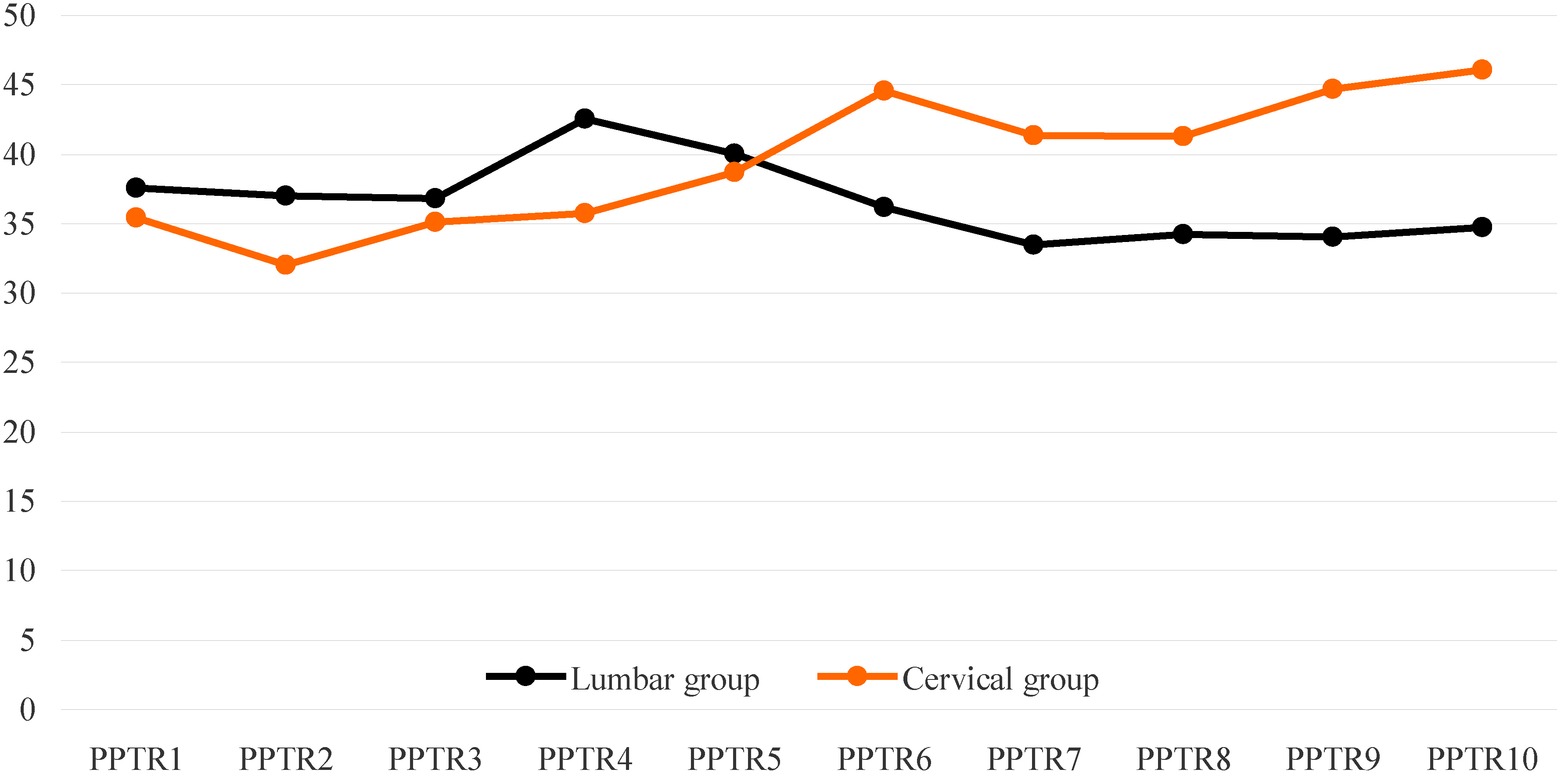
Algometric values on the left side of the body of the patients with cervical and lumbar radiculopathy after completion of the treatment (PPTL – pressure pain threshold on the left side of the body).
Algometric values on the right side of the body of the patients with cervical and lumbar radiculopathy after completion of the treatment (PPTR – pressure pain threshold on the right side of the body).
There was no statistically significant difference in the age of patients between the cervical and lumbar group (
The side of the body on which pathological changes in radiculopathy were diagnosed was analyzed in 119 patients, because in one patient with cervical radiculopathy, there was no relevant information about it. The results showed statistically significantly more patients with unilateral lumbar radiculopathy (45 subjects), compared to the patients with cervical radiculopathy, wherein the pathological changes were diagnosed significantly more bilaterally (50 subjects) (
The level of the spinal column with pathological changes in radiculopathy was observed in 78 patients, while in 42 patients, there was no relevant data due to incomplete findings of diagnostic procedures. The most common level of the spinal column with pathological change was L5–S1, present in 22 subjects (28.2%). Next by frequency was L4–L5 level, detected in 6 subjects (7.7%) and C6–C7, also detected in 6 subjects (7.7%). Other levels were significantly less marked as the place of origin in radiculopathy.
Before starting the treatment cycle, average PPT values on a 9 lumbar point on the left side (PPTL) and on the right side (PPTR) of the body (PPTL6, PPTR6, PPTL7, PPTR7, PPTL8, PPTL9, PPTR9, PPTL10, PPTR10) showed that there is a statistically significantly stronger experience of pain in the lumbar region in a patient with lumbar radiculopathy compared to the experience of pain in the lumbar region in a patient with cervical radiculopathy. A statistically significant difference in only one point of the cervical region (PPTR4) showed that the patients with lumbar radiculopathy in the cervical region were much closer to the patients with cervical radiculopathy in the cervical region according to the average PPT values (Graphs 1 and 2). Upon analyzing the PPT between the patients with cervical radiculopathy and patients with lumbar radiculopathy after completion of the treatment, statistically significant differences were not obtained at any point (Graphs 3 and 4).
The comparison of the PPT total value from cervical points in patients with cervical radiculopathy with total value of the same algometric parameter from lumbar points in patients with lumbar radiculopathy was conducted to determine which condition is more painful, cervical or lumbar radiculopathy. Before starting the treatment cycle, the mean PPT on lumbar points in lumbar radiculopathy was slightly lower than the PPT on cervical point in cervical radiculopathy, 37.21 N/cm
Average summation of HADS between patients with cervical radiculopathy and patients with lumbar radiculopathy before and after the treatment cycle
Average summation of HADS between patients with cervical radiculopathy and patients with lumbar radiculopathy before and after the treatment cycle
Analyzing PPT values from only lumbar points before and after the treatment cycle in patients with lumbar radiculopathy, it can be noticed that there were no statistically significant differences (Graphs 1–4). Comparing PPT values from only cervical points before and after the treatment cycle in patients with cervical radiculopathy, a statistically significant difference on 3 points (PPTL1, PPTL2, PPTR1) was observed in terms of pain reinforcement (Graphs 1–4).
The comparison of the PPT total value of all examined points between males and females with radiculopathy showed that, before the treatment cycle, males have a statistically significant higher value of the observed parameter than females, 43.30 N/cm
Based on the average total score, the subjects in this study were without depression, but with borderline anxiety. The difference in average total score of anxiety and depression between patients with lumbar and cervical radiculopathy was not statistically significant before or after the treatment cycle (Table 1). When analyzing the lumbar patient group before and after the treatment, a statistically significant difference in the level of depression does not exist (Wilcoxon test, Z
Radiculopathy is one of the most commonly present musculoskeletal disorders, and may be diagnosed as unilateral or bilateral [2].
Our research has shown that the unilateral radiculopathy was more often diagnosed in the lumbar region, while the bilateral radiculopathy was significantly more frequently present in the cervical spine. The most common levels of the spinal column with a pathological change in patients with radiculopathy in our study were L5–S1 and C6–C7, which is consistent with findings in the literature [16].
Pain is probably the most difficult bearable symptom for patients with cervical and lumbar radiculopathy [17]. The pain response depends on individual predisposition (gender, age, race, and genetic heritage), environmental factors (external stressors and previous painful experience) and psychological factors (anxiety, depression, and catastrophism).
Algometry is a scientific and a clinical method of quantification of the sensitivity of the soft tissue and mapping the pain [7]. The literature emphasizes that the PPT of less than 29.42 N/cm
The consideration of possible differences in the degree of pain between cervical radiculopathy and lumbar radiculopathy in our study was conducted by comparing the PPT values obtained from cervical points in cervical radiculopathy and from lumbar points in lumbar radiculopathy. A significant difference in PPT values between the neck region and the lumbar region was not established, which indicates that the cervical and lumbar radiculopathy have similar levels of pain. Observing the PPT values in all tested points, it can be noted that, before starting and after completion of the treatment cycle, the patients with cervical radiculopathy experience pain considerably on the lumbar points. In addition, the patients with lumbar radiculopathy experience pain significantly in the neck region. The obtained data can be analyzed as a result of sensitization and the occurrence of hyperalgesia in places where the pain primary did not exist. Widespread hyperalgesia is related to myofascial trigger points, which may be present independently of radiculopathy. Although myofascial trigger points could not be established with certainty in any patient, it may be assumed that the origins of the pain were trigger points in the body regions that were not affected by radiculopathy.
The radiculopathy treatment involves the application of one or more therapeutic modalities, and is commonly prescribed kinesitherapy, ultrasound, laser therapy, and manual therapy, with the use of analgesics if it is a mild extent of radiculopathy. Strengthening the muscles with exercises implemented in the physical treatment of cervical and lumbar pain conditions causes an increase in the PPT in the arms and legs and the neck muscles after a few weeks or months of exercising, the authors of several studies [12, 19] noticed. Levoska and Keinänen-Kiukaanniemi [20] state that encouraging results are achieved by prescribed exercises of kinesitherapy in patients with pain in the neck and shoulders. The active and passive exercises were applied for 2 months. After the treatment, it showed a significant reduction of pain and reduction in the number of trigger points in both groups of subjects with different types of exercise.
The treatment of patients involved in our study included only kinesitherapy in the average duration of 2–3 weeks. After the completion of the therapy, a statistically significant reduction of pain was found in only three examined points in patients with cervical radiculopathy. Probable factors of weak results of the therapeutic program include the selection of only one therapeutic modality, improperly performing exercises, and short duration of the treatment. One of the explanations for the mechanism of pain reduction with the assistance of long-term exercise is that the continued training initiates neural adaptation, mainly due to increased rates of contraction of motor units, recruitment of high threshold motor units, and better control of motor units [21]. The increased motor control means the increased activity of the afferent and efferent motor pathways, which can inhibit pain pathways.
The frequency of musculoskeletal pain disorders is higher in women compared to men [22], and pain threshold value is lower in women compared to men [13]. Women had a lower pain threshold than men in studies on head and neck muscles [23], knees [24], and stomach [25].
The examinations in our study confirmed the findings of previous studies that females generally have lower pain threshold compared to males. The cause of the difference in pain sensitivity between genders is not fully understood, but it is assumed to include a physiological (differences in hormone balance, the amount of subcutaneous adipose tissue, muscle size, and menstrual cycle), cultural, and psychological factors [9, 26].
Previous perceptions of pain were based solely on the connection between the intensity of pain and nociception. Recent findings have shown that the experience of pain also affects a wide range of psychological factors such as anxiety, depression, fear, misconceptions about the nature of pain, and the likely outcome. Anxiety and depression are conditions often present in people with chronic pain, and in many cases they overlap [27]. It isn’t yet established whether depression is a cause or a consequence of low back pain. Depression worsens the prognosis of pain in the lower back, leading to poor results of therapy, and is often unrecognized and untreated [28]. Hence, it is essential that physicians within the biomedical approach also analyze the psychological factors of diseases.
The results of our study indicate that psychological factors greatly affect the pain and that patients should be included in a multidisciplinary rehabilitation program that would involve work with a psychologist and, as a good example, the application of cognitive-behavioral therapy is proposed [29].
Limitations of the study: Patients with thoracic radiculopathy were not examined in this study. Examination on a larger number of patients with radiculopathy and their comparison would be interesting in some future research.
Conclusions
Algometry and psychological tests have not yet reached wide enough application in the diagnosis and monitoring of cervical and lumbar pain conditions, although these methods are easy to use, objective, and safe. It is particularly useful to conduct algometric testing during or after the end of the treatment, in order to verify the results of therapy protocols intended for the patient and to allow a timely response to an inadequate treatment. Similar results of algometric testing in patients with cervical radiculopathy and in patients with lumbar radiculopathy, as well as a high level of soreness in the paravertebral part of spine that is not affected by pathological changes, argue in favor of the conclusions that the spine should be seen as an entirety – “integrative model”. Radiculopathy in conservative therapy should be treated in cervical-thoracic and lumbar region together, not only depending on the level of damage, as it is currently the practice in some rehabilitation programs. Our results suggest that the rehabilitation period for patients with radiculopathy have to be longer, if not within the hospital treatment, then certainly as to regular outpatient treatment. It is also necessary to design exercises for each patient individually, according to the specific condition and to set targets of therapy. Work with a psychologist would ensure the optimization of therapeutic treatments and provide assistance to a patient in a physical and psychological sense. Considering that the comparison of the pain intensity between cervical and lumbar radiculopathy has not been available in the literature, the results of our study provide new insights into the discussed topic.
Footnotes
Conflict of interest
None.