
Abstract
BACKGROUND:
Patellofemoral pain syndrome (PFPS) is one of the most common knee disorders affecting women.
OBJECTIVE:
The purpose of this study was to investigate the effects of balance taping on PFPS.
METHODS:
Balance taping using kinesiology tape was applied for 2.5 months (average of 16 h/day) to both knees in a 26-year-old female nurse with bilateral PFPS.
RESULTS:
The congruence angle decreased in the right and left knees from 30
CONCLUSION:
Considering the outcome of the study, we recommend balance taping as a complementary treatment method for PFPS.
Introduction
Outcomes of the patient-specific functional scale
Outcomes of the patient-specific functional scale
PSFS, Patient Specific Functional Scale.
Patellofemoral pain syndrome (PFPS) is one of the most common knee disorders affecting women [1]. PFPS is characterized by peri-patella pain in or around the patella (behind the kneecap) when sitting or squatting with the knees flexed or while ascending or descending stairs [2]. PFPS can be caused by several factors such as an increased Q-angle [3, 4], weakness in the quadriceps [5], and reduced flexibility of the lower extremity [5, 6].
Lateral displacement of the patella within the fem-oral trochlea occurs in patients with PFPS [7]. The degree of malalignment in PFPS can be identified via the congruence angle (the angle formed by the line bisecting the sulcus angle and the line connecting the vertex of the sulcus angle to the lowest point on the patella) [7]. A normal congruence angle is typically around
PFPS patients with abnormal structures in the lower extremity may experience excessive stress on the patellofemoral joint [10, 11]. Weakness in the vastus medialis oblique in patients with PFPS may contribute to abnormal lateral displacement of the patella [12]. Therefore, we aimed to investigate the effects of repeated balance taping using kinesiology tape in a female nurse with PFPS.
A 26-year-old female nurse with bilateral PFPS presented with knee pain when sitting after standing, standing after sitting, or kneeling. The patient was evaluated by the same examiner (who was blinded to the experiment) before the treatment, after 1 month, and after the final treatment. Radiographs were obtained before treatment and after the final treatment with the same radiologist, X-ray machine, and high-quality film plates. The pain corresponded to a Numeric Pain Rating Scale (NPRS) score (0, no pain; 10, the worst imaginable pain) of 6/10, but she did not receive any particular treatments. The Patient Specific Functional Scale score (PSFS; 0, unable to perform the activity; 10, able to perform the activity) [13], which is a useful tool for assessing the patient form the activity) was 17/50 (Table 1). In the initial assessment using radiological angles, the right and left congruence angles were 30
The initial congruence angle of both knees (A, right congruence angle; B, left congruence angle).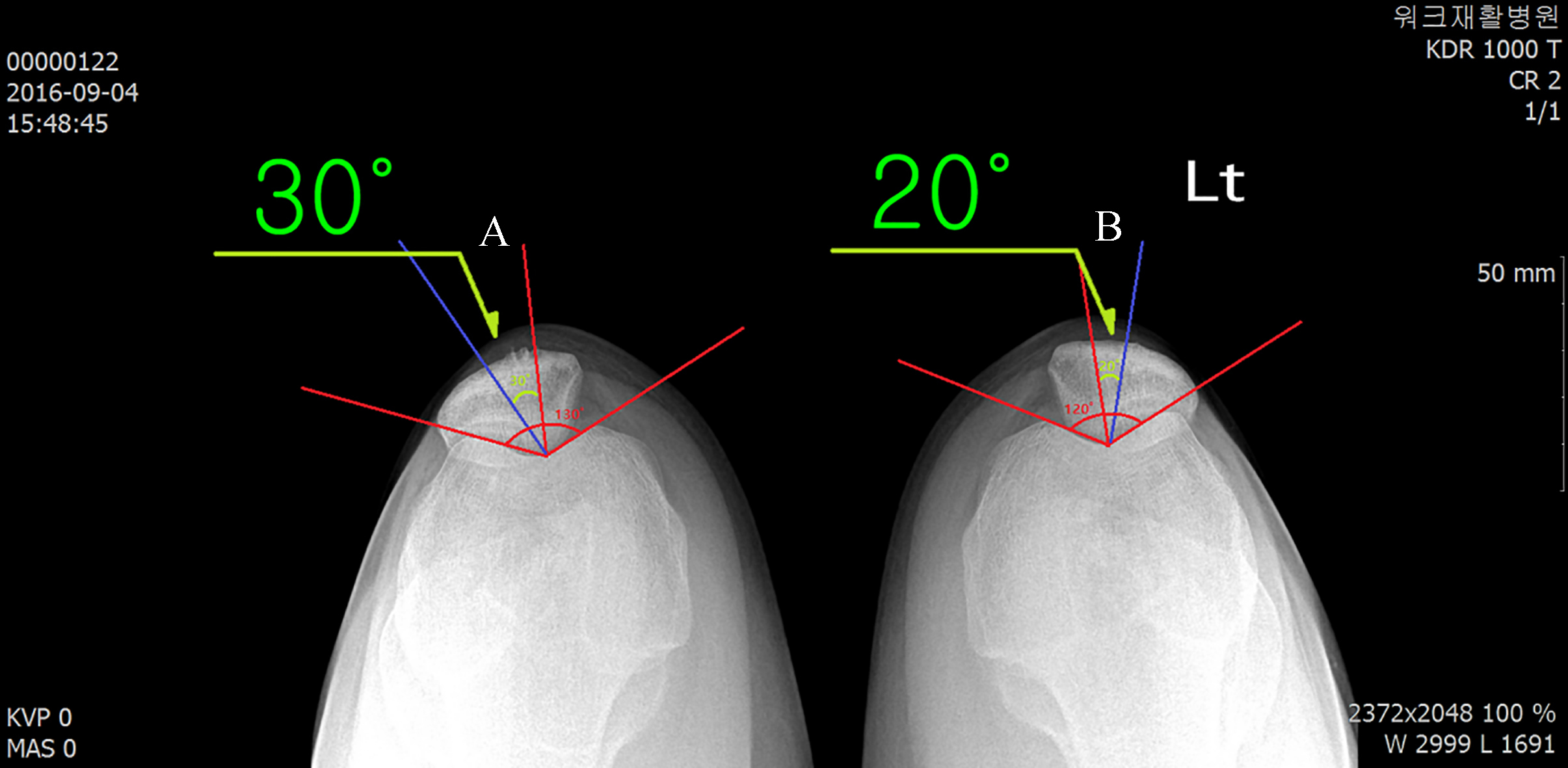
Balance taping using the kinesiology tape for musculoskeletal disorders [14] was applied for 2.5 months (average of 16 h/day) to reduce abnormal lateral displacement in the patella. The kinesiology tape (BB TAPE, WETAPE Inc., Pyeongtaek, Korea) for PFPS was 2.5 cm wide and was applied with an approximately 30–40% stretch.
Balance taping for PFPS was performed as follows. First, the I-shaped kinesiology tape was applied via a horseshoe taping technique, where the taping began from the outer center of the patella, with the patient‘s knee slightly bent, and continued in both directions above and below the patella as the patella was moved medially. Second, another I-shaped kinesiology tape was reapplied using the same method to overlap the first taping by about 80% to reinforce the mechanical correction effects in order to maintain the medial movement of the patella (Fig. 2).
Balance taping for patellofemoral pain syndrome.
To prevent skin irritation, the beginning and end portions of the I-shaped elastic tape (approximately 2–3 cm) were applied without stretching [15], and to prevent itchiness, the tape was removed each day and new tape was reapplied [16].
After balance taping, the total PSFS score increased from 17/50 to 46/50 after 1 month and to 50/50 after 2.5 months, indicating a functional improvement in the knees. After balance taping for 1 month, the NPRS score from sitting to standing, from standing to sitting, and kneeling improved from 6/10 to 3/10. After 2.5 months of applying balance taping, the NPRS score was 0/10, indicating no pain in the knee joints. After 2.5 months of applying the balance taping, the congruence angle in the right and left knee decreased from 30
The final congruence angle of both knees (A, right congruence angle; B, left congruence angle).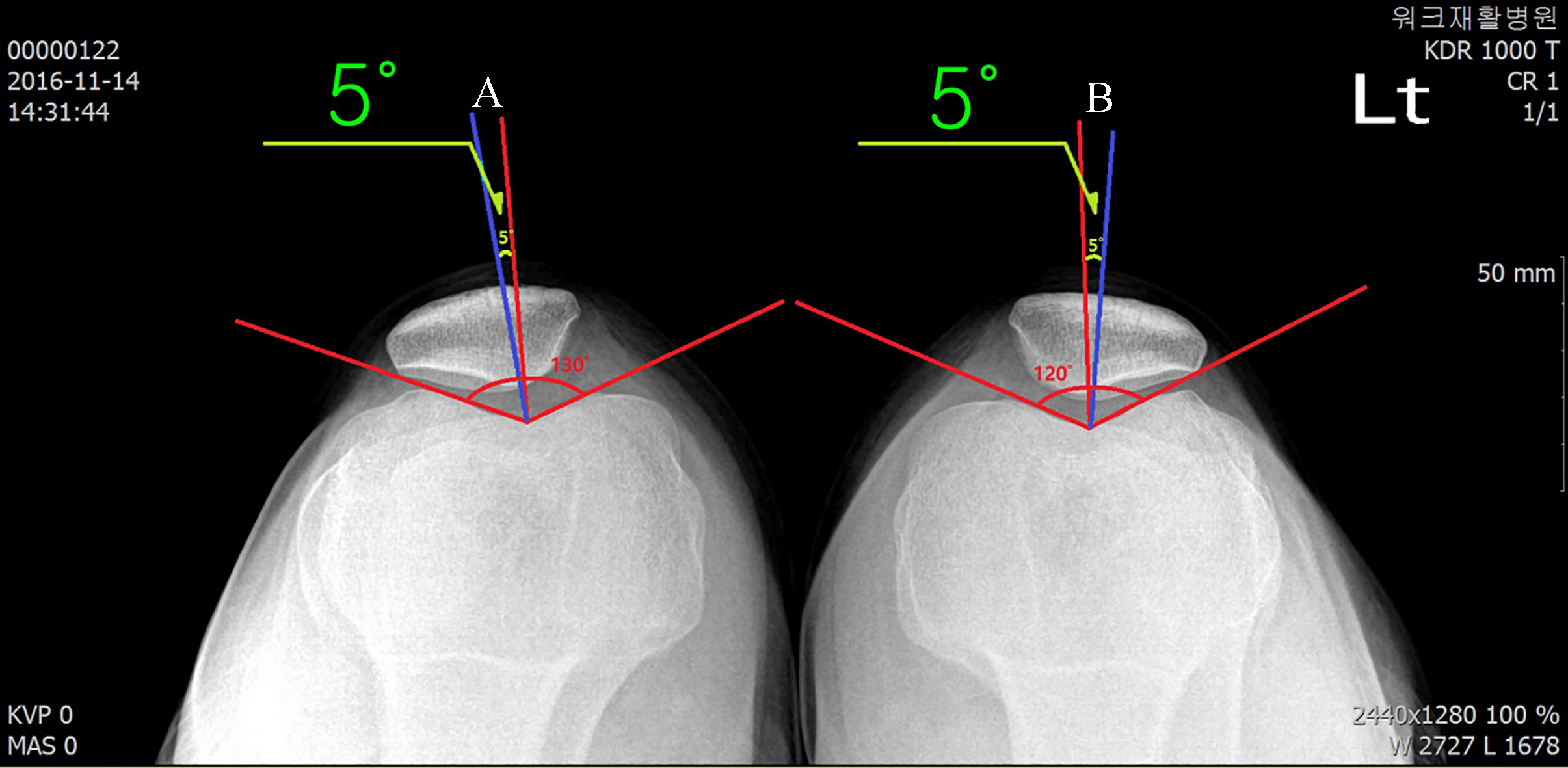
In this case study, repeated application of balance taping for 2.5 months was able to reduce PFPS. Balance taping that was repeatedly applied for medial movement of the patella with abnormal lateral displacement was able to correct patellar malalignment and ameliorate PFPS.
The I-shaped kinesiology tape applied for mechanical effect on the abnormal lateral displacement of the patella was stretched by approximately 30–40%, and as a result, reduced elasticity in the tape provided resistance when the patella moved again laterally. Even if the patella moves laterally after the balance taping is applied, the increased tension in the tape acted to cause medial displacement of the patella, which resulted in a gradual reduction in the congruence angle [17].
Application of kinesiology tape is known to stimulate lymphatic circulation [18] and cause pain relief [15, 19, 20], in addition to exerting mechanical effects on shoulder [21] and pelvis [22] malalignment. In a recent study, applying balance taping bilaterally in a patient with moderate hallux valgus for 3 months achieved pain relief with decreased right and left hallux valgus angles from 21
Although the causal relationship between alignment and pain is unclear, alignment is one of the factors associated with pain [23]. Therefore, balance taping reduced the congruence angle by correcting the abnormal lateral displacement of the patella, and this recovery of patellar alignment was able to reduce the pain that appeared during functional movement of the knees.
Based on the findings described in this case study, we believe that balance taping can be a complementary treatment method for PFPS. Additional studies are needed to examine the effects of balance taping on a greater number of PFPS patients and to compare balance taping to other conservative therapy methods.
Footnotes
Conflict of interest
The authors have no conflict of interest to report.