
Abstract
OBJECTIVE:
To examine the immediate effect on dynamic and static balance of a manual protocol of plantar stimulation in healthy subjects.
MATERIALS AND METHOD:
Of the 144 healthy and physically active volunteers recruited, 98 subjects participated. Subjects were randomly assigned and allocated to the experimental group (EG) (
RESULTS:
In the dynamic balance, a group effect was found in the anterior direction, posteromedial direction and composite scores of the mSEBT when groups were compared by limb. Changes in the posteromedial direction of both limbs (right limb:
CONCLUSIONS:
The application of a 10-minute manual stimulation protocol without joint mobilization, addressed to stimulate the plantar cutaneous mechanoreceptors, could elicit benefits on dynamic balance. This improvement was observed bilaterally even though only one plantar surface was stimulated. As balance deficits may impair functional movements and regular training in sports, this intervention aims to ameliorate dynamic balancing ability could improve the functional recovery of sport gestures.
Keywords
Introduction
Static balance is the ability to establish a stable base of support and maintain position while minimizing body movement [1]. Dynamic balance is the ability to perform a standardized movement around a base of support while maintaining a stable position [1]. Therefore, balance control is an essential requirement for functional movements, especially in regular training of athletes implying development of complex technical movement and injury prevention [2].
Controlling and maintaining balance is a complex process in which the musculoskeletal system, the nervous system and visual, vestibular and somatosensory information are involved [3]. Despite this multiple sensory involvement, in general, the central nervous system relies primarily on one sense at a time for postural orientation by pondering the accuracy of this information [4]. In this regard, scientific literature about postural control has focused on the role of the somatosensory system [5]. Specifically, data have supported the participation of the plantar cutaneous mechanoreceptors (MCR) in this process [6].
Owing to their location between the body and the ground, MCR provide detailed information about properties of the supporting surface, body position and movement in relation to the base of support [7, 8]. Consequently, several studies suggested that plantar cutaneous afferences from the soles of the feet could potentially provide valuable feedback for balance regulation [6, 9, 10]. In this regard, pressure has demonstrated to stimulate MCR [11]. The employment of textured insoles and surfaces [12, 13], a medial arch support [14] and vibration [15] has been explored previously to stimulate plantar sensitivity and to improve balance control [9]. Likewise, manual stimulation of the plantar sole has been shown to improve assessment of pressure cues from the supporting area on firm surface, causing better distribution of body weight over the two feet [3, 16]. Specifically, Preszner-Domjan et al. [3] studied the effect of manual stimulation of the sole on postural stability in healthy young adults. Postural stability in quiet stand was assessed with eyes open and closed, on a firm surface and then on a foam surface before and immediately after the intervention. All the participants received ten minutes of manual sliding and static pressure applied to the plantar surface of both feet. Their results showed that the sway path decreased significantly on the AP and ML directions under firm surface and eyes closed conditions. These authors highlighted the interest to investigate whether the changes on postural control of manual stimulation would be similar if it was applied only in one of the two soles. Therefore, exploring the effects of plantar stimulation without joint mobilization techniques could provide physical therapists and exercise therapists an effective and low-cost tool that could be useful to improve balance in sport gestures in different disciplines [9, 17].
Accordingly, in this study it was hypothesized that the application of manual stimulation techniques on the sole of one foot, following an easily reproducible protocol, could improve balance. Thus, the purpose of this study was to examine the immediate effect on dynamic and static balance of the manual stimulation of the sole of one foot in healthy subjects.
Methods
Participants and design
A total of 144 healthy subjects, who regularly did physical exercise, volunteered to participate in this study. Participants were recruited from (blinded), where the study took place, in July 2015. Exclusion criteria were: age
A single-blind randomized controlled trial was performed in the authors’ university research laboratory. Simple randomization allocated participants to the experimental group (EG) or to the control group (CG). A random-number table was used for allocation and concealment was performed by using opaque sealed envelopes. Before enrollment, all participants were informed and provided written informed consent. The study was approved by the authors’ University Human Research Ethics Committee (protocol number H1393258758403) and all procedures were conducted according to the Declaration of Helsinki. The study was registered at www.clinicaltrials.gov (blinded).
Outcomes were measured before and immediately after the intervention by two researchers blinded to group assignment. One assessor evaluated the dynamic balance and the other assessed the static balance. An external assistant not involved in the study performed assignment. According to group allocation, EG participants received plantar stimulation while CG participants remained seated. A physical therapist, with over 15 years experience in the field of manual therapy and who was blinded to baseline data, performed the intervention. Participants were asked to refrain from conducting any exercise in the 2 hours prior to participating in the study and to wear shorts to avoid any additional skin stimulation on the legs.
Intervention
A 10-minute manual stimulation was applied to the plantar surface of the right foot [3]. The subject was positioned on a plinth in a supine position. The sequence of the applied techniques is explained in Fig. 1.
Diagram of the manual stimulation applied on the right foot. The techniques were applied with both thumbs and the following sequence was carried out: A) Sliding pressure in longitudinal direction (lines) performed on each interdigital space and on the internal longitudinal arch (5 repetitions of 10-second duration each); B) Sliding pressure in transverse direction on the region of the metatarsal heads (5 repetitions of 5-second duration each); and C) Static pressure on the head of the first and the fifth metatarsal bones, the center of the midfoot and the heel (5 repetitions per point of 10-second duration each).
To avoid bias, the intensity and duration of the stimulation were standardized. The therapist applied the techniques on a dynamometer (Nicholas Manual Muscle Tester, Lafayette Instruments, Lafayette, IN.), ensuring a mean pressure of 48 N
Demographic and anthropometric data (height, weight and length of both limbs) were registered. Limb length was measured (in cm) from the most inferior aspect of the anterior superior iliac spine to the most distal portion of the medial malleolus with a cloth tape [18], after stabilizing the pelvis [19]. Before testing, a demonstration of each assessment procedure was explained.
Dynamic balance was assessed by using the modified Star Excursion Balance Test (mSEBT) [20]. A grid formed by three 120-cm lines, made with standard tape, running at an angle of 120
The testing grid for the modified star excursion balance test. Toes should be placed at the 0 mark position (grey dots) for the anterior (A) reach, while the heel should be placed at this mark for the posteromedial (PM) and posterolateral (PL) reaches.
Diagram of subject flow from recruitment to data analysis.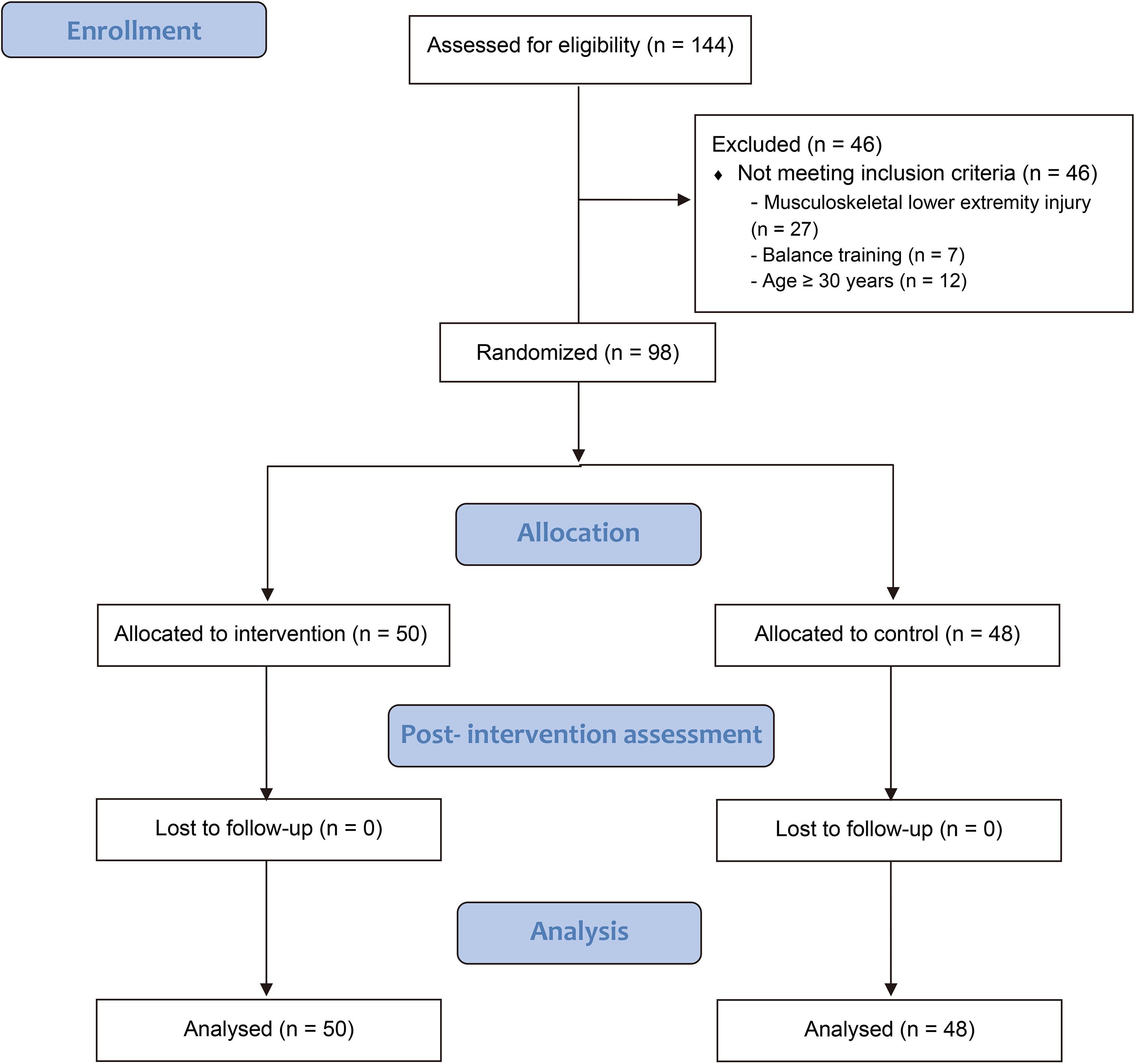
Static balance was assessed by using the Unipedal Stance Test (UPST) [23]. Participants were asked to maintain balance for as long as possible in one-leg stance with eyes closed to avoid visual input. Subjects began in a relaxed standing position, barefoot, with eyes open and their weight evenly distributed on both feet. They were then asked to cross their arms over the chest and close their eyes. Once they felt their posture was stabilized, they had to stand on one limb while raising the other so that the raised foot was near but not touching the stance limb. Subjects were timed from the moment they lifted the foot off the floor to a maximum of 45 seconds [22]. Reasons for the trial to be disregarded and repeated were: (1) use of the raised foot (touching the floor or moving it away or toward the standing limb); (2) uncrossing the arms; (3) moving the standing foot to maintain balance; and (4) opening eyes. Participants performed one trial with the right limb followed by one trial with the left limb, thus completing one set. Subjects performed 3 sets with a 1-minute rest between sets to avoid fatigue. Duration of each trial was recorded. The average time of the 3 trials for each limb was used as dependent variable.
A prior power analysis using the Gpower software [25] indicated that a total sample of 98 subjects would be needed to detect medium effects (
Changes scores (postintervention values minus baseline values) of the UPST time and the mSEBT normalized individual directions and composite scores were used for statistical analysis. To compare the change of the dynamic and static balance between groups by limb, a series of 5 mixed-model 2-by-2 ANOVAs were performed on each dependent variable, with group as between-subjects factor (EG versus CG) and limb as within-subjects factor (stimulated versus non-stimulated). If between-group differences were significant, appropriate post-hoc analysis was performed. In addition, to discriminate real changes from measurement errors, the standard error of measurement (SEM) was estimated from baseline data (SEM
Results
Ninety-eight volunteers meeting the inclusion criteria, who were randomly assigned (EG,
Demographic data and baseline characteristics of participants
Demographic data and baseline characteristics of participants
Values are expressed as mean
The results of the mixed-model 2-by-2 ANOVAs are shown in Table 2. Regarding the dynamic balance, a significant group effect was found for the A direction, PM direction and composite score of the mSEBT. Post-hoc analysis indicated that for both limbs the PM direction change was significantly greater in the EG than in the CG (right limb:
Comparisons between groups by limb
Standard error of measurement and the smallest detectable change of each variable
Data were taken from the baseline data of all participants. SEM: Standard Error of Measurement (SEM
This study showed an immediate effect on dynamic balance of the suggested manual stimulation. This improvement was observed bilaterally even though only one plantar surface was stimulated. In particular, the EG improved in the PM direction and composite score of the mSEBT. The PM direction has been reported to better represent the overall performance of the mSEBT [26]. However, the proposed protocol did not modify the static balance assessed by the UPST. Therefore, our findings suggest that the stimulation of the sole of the foot by using a 10-minute manual therapy protocol without joint mobilization could have an influence on the plantar MCR, offering benefits on dynamic balance.
In the side-by-group analysis, a group effect was found in the dynamic balance. There was a between-group statistical significant difference in the PM and A directions and composite change score of the mSEBT for both limbs. These variables resulted in a higher increase in the EG than in the CG. Therefore, a bilateral immediate effect was shown, although only one sole was stimulated. Spinal and supra-spinal mechanisms are involved in the sensorimotor control of posture [27]. Hence, the protocol may have triggered the mediation of these mechanisms, accounting for the bilateral improvement.
To perform the PM direction reach, subjects maintain balance by shifting their bodyweight forward, thus increasing the pressure on the forefoot sole. Besides, owing to the reduced visual awareness, an increased demand is placed on the somatosensory feedback [28]. In fact, improvement in this direction of young female athletes has been attributed to dynamic balance enhancement [29]. Consequently, assuming that the applied protocol focused on the metatarsal region (Fig. 1), this finding may stem from an increase in the sensitivity of the MCR of the forefoot sole.
The change of the A direction reach was higher in the EG than in the CG, although it was under the SDC. The A reach has been shown to be more constrained by mechanical restriction than by sensorimotor deficits in chronic ankle instability [30]. Besides, it is primarily a sagittal plane movement in which visual information in reaching with the foot is easy to obtain.
Regarding the static balance (UPST time), the improvement for the right limb was greater in the EG than in the CG, but this between-group difference was not statistically significant. This finding may be related to: (1) limb dominance (92.8% of right-leg subjects); (2) the ceiling effect of the test, though we followed a 45-second UPST trying to avoid it [23, 31]; and (3) the baseline average value of our sample (Table 1), which exceeded the normative value in healthy people (9.4
It has been stated that during static balance the stimulation of the skin produces a clear sense of pressure change on the sole [32]. To maintain an optimal postural control, the stimulation of the sole somatosensory receptors was proved to increase the plantar feedback when eyes are closed [12]. Though the stimulation protocol of this study increased the time in the UPST, this improvement did not reach statistical significance. In this regard, when other mechanical stimuli were applied, similar results were found. The use of a 5-hertz platform during 10 minutes yielded no significant changes on the static balance in healthy subjects [9]. By contrast, this form of stimulation of the sole MCR could compensate for a superficial plantar sensory deficit in older subjects. Likewise, other authors [8] found no significant differences in standing balance parameters when a control and a textured insole were compared.
Clinical importance
The clinical importance of the data presented herein stems from their applicability to the functional recovery in sports or several pathologies. The current study has demonstrated positive effects in healthy subjects, thus our stimulation protocol could be tested in different sports that require balance control, as those related to asymmetric positions, i.e. hockey, tennis or gymnastics. In addition, our protocol may reduce lower extremity injuries since balance is essential for optimal performance and prevention of athletic injuries. Likewise, the intervention could also be applied to several pathologies, as plantar fasciitis, sensitivity changes with gait alterations, etc., in order to reinforce the proprioceptive awareness of movement and position.
Strengths and limitations
According to our results, a 10-minute manual stimulation protocol without joint mobilization applied on the sole of one foot has an immediate effect on the dynamic balance of healthy subjects. Other authors [3] showed that this kind of stimulation is only effective in improving the static postural control in healthy adults in the absence of visual information. Nevertheless, although the same pressure was used, the exact protocol or the duration and direction of each maneuver were not specified. By contrast, we have used a thorough methodology, controlling the duration in all the interventions and applying the protocol on a single foot.
Few studies have investigated the effect on postural stability of other types of manual stimulation, named manual therapy and mobilizations of the feet [34] and foot massage [16, 35]. However, they did not assess the effect on the dynamic balance.
To the best of our knowledge, there is no other investigation in which a reproducible plantar stimulation protocol alone had an immediate effect on the dynamic balance in healthy subjects. As a reduction in balance occurs after a short period of immobilization [33] and taking into account that joint movement restriction is quite usual in sports injuries, this intervention could offer a suitable, fast, simple and low-cost alternative.
In this study the main limitation was the reduced immediate effect found on static balance. Perhaps, the use of instrumental assessment systems would have yielded more meaningful results. Likewise, though the mSEBT is frequently used as a clinical measure, is quite subjective. Thus, it is recommendable to confirm the results of the dynamic balance by using more objective methods (e.g. force plates). The subjects of the study were physically active, doing exercise between 2 and 5 times a week. However, the time and type of exercise were not exactly controlled. Besides, since neurologically healthy subjects were included in the study, generalizability and external validity of the results may be limited.
Finally, it would be interesting to study if the effect of the stimulation can be sustained over a longer period of time if a greater number of sessions is used. Future studies on the medium/long-term effect of the suggested protocol in athletes with balance deficits after injury, are needed.
Conclusions
Manual plantar stimulation is effective in improving the dynamic balance assessed by the mSEBT. This protocol has an immediate effect on the PM direction and the composite score. However, the immediate effect on static balance evaluated by UPST did not provide conclusive results.
Balance deficits can impair everyday functioning and cause a worse performance in regular training, producing injuries in athletes. Moreover, many complex technical movements are dynamic. Thus, all those interventions aiming to improve dynamic balancing ability are of clinical relevance to any rehabilitation program. manual plantar stimulation may be a useful tool for the purpose of improving dynamic balance.
Footnotes
Conflict of interest
None to report.
Appendix
Formulas used to normalize reach distances and to calculate the composite score of the Star Excursion Balance Test [17, 20].
The formula used to normalize reach distances to subjects’ leg length was:
The composite score was calculated by using to the following formula:
where