
Abstract
BACKGROUND:
Among new technological rehabilitation systems, there are proprioceptive platforms. These could be useful to improve static and dynamic balance.
OBJECTIVE:
To evaluate technological proprioceptive rehabilitation compared to conventional rehabilitation in patients after total hip arthroplasty (THA).
METHODS:
Sixty-four patients after THA were divided in two groups: a conventional group (CG) and a technological group (TG) treated with proprioceptive platforms. Before (T0) and after 20 sessions (T1), we recorded static and dynamic balance. Clinical and disability scales (Modified Harris Hip Score, Barthel Index, Deambulation Index), pain scales (ID-PAIN, DN4, VAS) and QoL scale (SF-36) were administered to patients during T0 and T1. Mann-Whitney U test was used for stabilometric and dynamic assessments to detect differences between groups of patients and healthy subjects. The Wilcoxon signed-rank test was used for the within-group analysis and the ANCOVA test for the analysis between groups of patients.
RESULTS:
All scales improved significantly in both groups after treatment (
CONCLUSIONS:
Both treatments improved the clinical, disability, pain, and QoL scales, as well as static balance, but only proprioceptive technological rehabilitation improved dynamic balance. Rehabilitation through proprioceptive platforms can indeed improve static and dynamic balance, which are both crucial for the patient’s safety and autonomy.
Keywords
Introduction
Total hip arthroplasty (THA) is one of the most commonly performed orthopedic operations in the world. Osteoarthritis that does not respond to pharmacological and conservative treatments is one of the main indications for hip replacement. The number of hip replacement operations continues to grow on account of an increasingly older population, a reduction in the average age of the treated population and higher quality of life expectations [1].
Osteoarthritis, the most common rheumatic joint disorder, affects many different body parts, causing pain, stiffness and reduced function and health status [2]. However, irrespective of the improvement attained in both pain and function following a hip arthroplasty, a patient’s quality of life will remain lower than that of healthy adults; the persistence of functional limitations can be caused by a reduction in proprioception, which is the inevitable result of the disease, which is in turn exacerbated by surgery [3, 4].
It is unclear whether the proprioceptive deficit that accompanies degenerative joint disease derives from or contributes to the etiology of the pathological process. However, the disruption of muscle and joint mechanoreceptors caused by physical trauma results in a partial deafferentation of the joint and surrounding musculature and a consequent reduction in proprioception. The surgery subsequently exacerbates this deficit by removing anatomical parts that are rich in proprioceptive receptors and owing to the presence of postoperative pain and periods of immobility that precede and follow the surgery.
Proprioception is defined as the awareness of limb position and movement [5]. It is the sum of joint position sense (static aspect) and kinaesthesia (dynamic aspect). It is thus a prerequisite for balance control, body orientation and coordination of movements [6]. Until the last decade of the twentieth century proprioceptive rehabilitation was only added as the last stage in a retraining programme. This was probably due to a lack of knowledge regarding the physiological mechanisms that regulate proprioception, as well as possibly the belief that proprioception would reappear spontaneously during conventional rehabilitation sessions without the need for any specific retraining.
Recently, new technological proprioceptive rehabilitation systems are being tested, with the intent to focus on the presence of some form of biofeedback [7]. By providing visual and verbal feedback during rehabilitation, patients can be made aware of their movements and can receive instantaneous feedback to modify movement patterns, thereby avoiding repetition of errors and facilitating limb functional recovery. The physiotherapist can consequently monitor and, if required, modify the rehabilitation treatment according to any progress made or difficulties encountered by the patient.
Few studies have instead been published on the effectiveness of proprioceptive rehabilitation, even of the technological type, after THA [8].
Given this background, our hypothesis is that a technological proprioceptive rehabilitation that combines visual feedback and conventional rehabilitation may be more effective than conventional rehabilitation alone in balance recovery. The aim of this study was to evaluate technological proprioceptive rehabilitation (using proprioceptive platforms) compared to conventional rehabilitation after THA. Moreover, a comparison of the instrumental static and dynamic balance between patients and healthy subjects was performed.
Materials and methods
Population
Sixty-four patients who underwent THA were enrolled in the study. The patients were divided in two groups: 28 patients in the conventional group (CG) and 36 patients in the technological group (TG). Thirteen patients, who were equally distributed in the two groups, underwent surgery following a femur fracture, while all the other patients underwent surgery because of hip osteoarthritis. The CG contained 10 males and 18 females (age: 63.9
The patients’ characteristics and clinical data are summarized in Table 1. A group of 40 age-matched healthy subjects (age range: 50–70, 17 males and 23 females) were also enrolled in the study.
Clinical, disability, pain and QoL variables: means (standard deviations) for the conventional group (CG) and the technological group (TG). Comparison between the two groups at T0. Values in bold indicate statistical significance (
values less than 0.05)
Clinical, disability, pain and QoL variables: means (standard deviations) for the conventional group (CG) and the technological group (TG). Comparison between the two groups at T0. Values in bold indicate statistical significance (
The study protocol was approved by the local ethics review board and each subject provided written informed consent.
Age from 50 to 80 years; first and recent (
Exclusion criteria
Previous joint replacement surgery; cognitive deterioration defined as a Mini-Mental State Examination (MMSE) score below 23; the presence of other joint prostheses, hip congenital dysplasia or inflammatory arthritis (rheumatoid arthritis, systematic lupus erythematosus) as the primary cause for surgery, Parkinson’s disease and sensitive neuropathy.
Study design
This work was a prospective controlled study. All outcome measures were administered before (T0) and after treatment (T1); the evaluator, a single physiotherapist, was unblinded to the patients’ group assignment. Age, sex, diagnosis, latency from surgery and type of operation were recorded in every patient.
Technological instruments
The instrumental assessments and the technological rehabilitation were performed at the Rehabilitation Department of the Don Carlo Gnocchi Onlus Foundation in Rome using a bipodalic platform (Prokin, Technobody, Italy). The system provides, at 40 Hz, the coordinates of the subject’s Center of Pressure (CoP) and also a biaxial accelerometer measures trunk tilts in the antero-posterior and medio-lateral directions. The instrumental evaluations were performed in the standing position and were assessed by a blinded therapist.
Stabilometric outcome assessment
The static evaluation consisted of a stabilometric assessment to evaluate balance with the platform in the blocked position. The following parameters were considered: area and perimeter of the center of pressure, anteroposterior and mediolateral velocity of the center of pressure with the eyes open and closed. The anteroposterior, mediolateral and total root mean square (RMS) of the trunk movements (with eyes open and closed) were also calculated to measure the stability of the trunk.
Dynamic outcome assessment
The dynamic evaluation consisted of an assessment of global proprioceptive control and postural instability with the platform in an unblocked position, the level of the damper was set according to each subject’s physical characteristics. The following parameters were considered: total, anteroposterior and mediolateral dynamic stability indexes and their relative RMS.
Functional outcome assessments
Clinical and disability scales (Modified Harris Hip Score, Barthel Index, Deambulation Index) [9, 10, 11], pain scales (ID-PAIN, DN4, VAS) [12, 13, 14] and QoL scale (SF-36) [15] were administered to every patient at both T0 and T1.
Treatment
After the initial instrumental and functional evaluation (T0), both groups of patients performed post-operative conventional rehabilitation treatment, consisting of 20 daily 45-minute sessions for 4 weeks (5 times/week).
Patients included in the CG underwent group treatment sessions (3 or 4 patients) lasting 45 minutes, 5 times per week. The treatment included techniques to improve joint range of motion, muscle force, ability to adopt different postures and proprioceptive exercises.
Patients included in the TG underwent group treatment sessions (3 or 4 patients) lasting 45 minutes, on the stabilometric platform, 5 times per week. The same physiotherapist administered the proprioceptive rehabilitation treatment.
The technological experimental protocol consisted of a series of rehabilitative paths proposed automatically by the software and designed to improve the perceptive conditions of each movement. The difficulty of the exercise was gradually increased over the course of the treatment or even within the same session when the patient’s condition allowed it.
Stabilometric results: comparison between each group and healthy subjects. A/P: anteroposterior; M/L: mediolateral; OE: open eyes; CE: close eyes.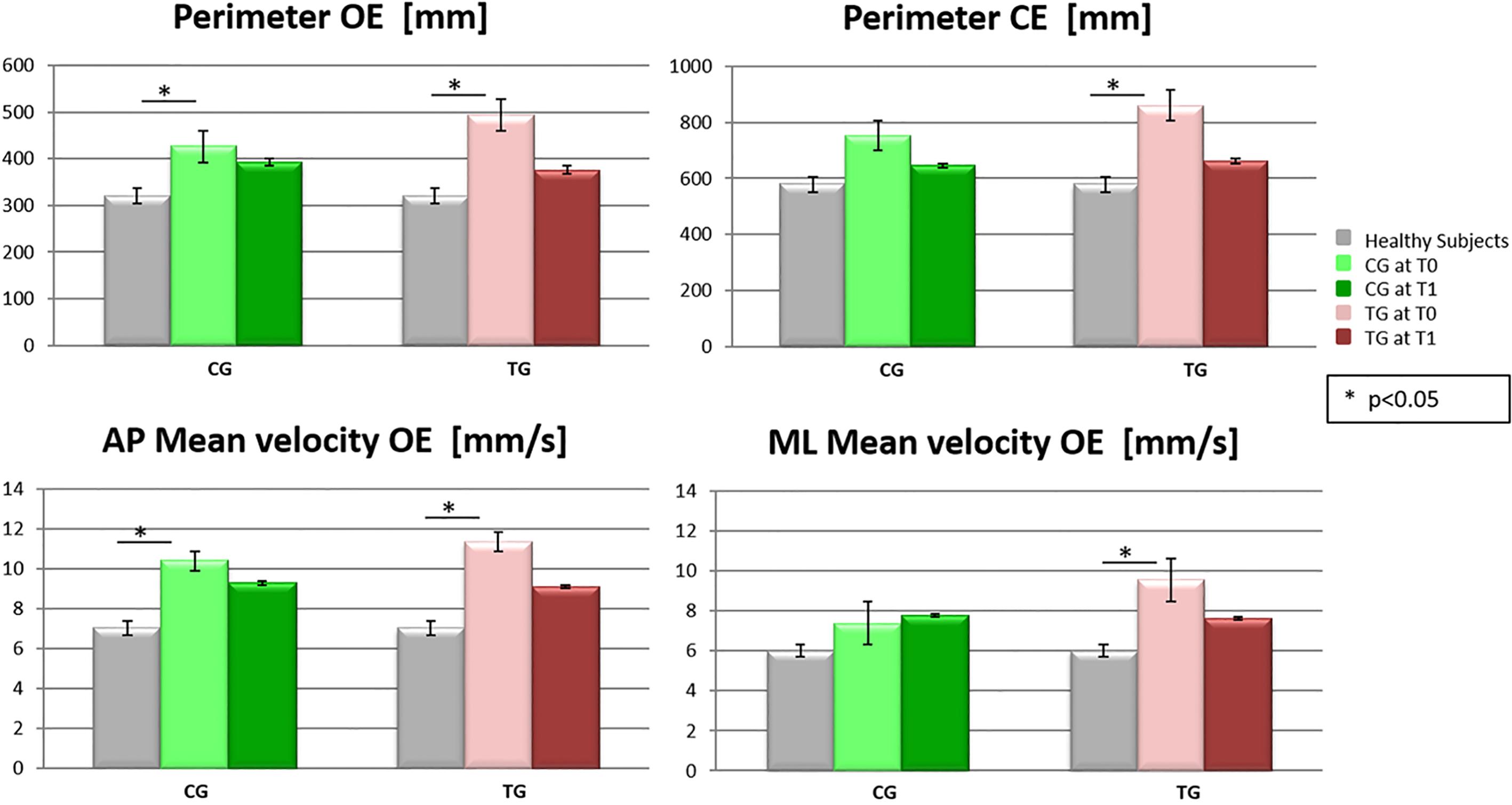
The statistical analysis was performed using the SPSS software package for Windows, version 12.0. All the data were tested for normality by means of the Shapiro-Wilk test. As the variables were not normally distributed, the Mann-Whitney U test was used for the stabilometric and dynamic assessments to detect differences between each patients group and healthy subjects at T0 and T1 evaluations. To evaluate the effects of the two treatments separately for each outcome measure, we compared the evaluation at T0 with the evaluation at T1 by means of a Wilcoxon signed-rank test. Moreover, to compare the effects of technological treatment with those of conventional treatment, we used the ANCOVA test for stabilometric and dynamic variables. The significance level for all the parameters was set at
Results
Clinical, disability, pain and QoL results
No significant differences in all outcome measures used (clinical, disability, pain and QoL) were observed between the two groups at T0 (Table 1). After therapy, both CG and TG improved in some functional, pain and QoL aspects. In particular CG improved significantly in: SF-36 Physical function (
Stabilometric results
No significant differences were observed in the stabilometric variables between the two groups at T0, except in “Mediolateral mean velocity OE” (
Comparison between each group and healthy subjects
When we compared the stabilometric variables in each group (CG and TG) at T0 with those from the healthy control group (Fig. 1), significant differences were detected for the CG in “Anteroposterior mean velocity OE” (
Stabilometric variables: means (standard deviations) obtained at T0 and T1, for both the CG and the TG, together with the results of the statistical analysis within-group analysis: T0
vs T1
, for the two groups separately; between-group analysis: CG vs TG. Values in bold indicate statistical significance (
values less than 0.05)
Stabilometric variables: means (standard deviations) obtained at T0 and T1, for both the CG and the TG, together with the results of the statistical analysis within-group analysis: T0
OE: eyes open; CE: eyes closed; AP: anteroposterior; ML: mediolateral; RMS: Root Mean Square.
Dynamic variables: means (standard deviations) obtained at T0 and T1, for both the CG and the TG, together with the results of the statistical analysis within-group analysis: T0
AP: anteroposterior; ML: mediolateral; RMS: Root Mean Square.
Dynamic results: comparison between each group and healthy subjects. A/P: anteroposterior; M/L: mediolateral; RMS: Root Mean Square.
An improvement was observed after treatment (T1) in both groups in static balance, as demonstrated by the fact that all the aforementioned stabilometric variables approached normal values (Fig. 1). Note that other stabilometric variables in CG after treatment showed significant differences: “Total (
The comparison between T0 and T1 of the stabilometric variables in each group revealed a significant improvement in the CG in “Anteroposterior mean velocity in OE (
Comparison between the CG and TG groups
With regard to the between-group analysis, we found a greater improvement in the TG than in the CG in the following stabilometric variables: “Total (
Dynamic instrumental results
In terms of the instrumental dynamic evaluation, no significant differences were observed in the outcome measures at baseline between the two groups.
Comparison between each group and healthy subjects
When we compared the dynamic variables in each group separately at T0 with the normal values, we detected significant differences for the CG in the “Total, Anteroposterior and Mediolateral Dynamic Stability Index” (
After treatment (T1), we observed significant differences in the CG in the same variables as those at T0, whereas significant differences in the TG were observed exclusively in the “Total, Anteroposterior (
Intragroup comparison T0 vs T1
The comparison between T0 and T1 of the dynamic variables in each group revealed a significant improvement only in the TG in the following variables: “Total (
Comparison between the CG and TG groups
With regard to the between-group analysis, we found a greater improvement in the TG than in the CG in the following dynamic variables: “Total Dynamic Stability Index” (
Discussion
Our study shows that rehabilitation treatment significantly improved static balance in all our patients who underwent THA. Indeed, the stabilometric variables approached normal values in both groups treated (TG and CG). However, in CG the trunk stability worsened after treatment, demonstrating that even after conventional treatment the trunk fails to recover the stability. In TG a greater improvement in static stability parameters was observed mainly in the CE condition, suggesting a considerable improvement of the proprioceptive sensitivity of patients, for which the visual stimulus is no longer necessary to maintain the stability in standing condition. Moreover, the dynamic balance significantly improved in TG: the dynamic instrumental assessment after treatment showed an improvement in the dynamic stability index in all directions only in technological group. Then our results suggest that technological rehabilitation after THA improves both static and dynamic balance, while conventional treatment improves static balance alone. As we hypothesized before the study, technological treatment results in better proprioceptive control. This result may be explained by the fact that balance and proprioception are closely related. The improvement in performance in the CE condition in our sample is a further confirmation of lower limb proprioceptive recovery. Indeed, other authors previously underlined that the hip and the knee joint play an important role in balance control in the CE condition; while the ankle joint plays the most important role in posture and balance maintenance in the OE condition [16].
In the last years, some studies are available on alterations in proprioception in subjects who have undergone THA. Post-surgical rehabilitation programs after THA should, according to current literature [17, 18, 19], be started as early as possible to prevent complications, which include deep vein thrombosis and luxation [20], to reduce pain levels, to recover joint movements [21], muscle strength [22] and tissue elasticity, to start weight bearing early, thereby achieving correct and pain-free deambulation by gradual weaning from aids. Treatment approaches can vary with regard to the frequency of care, functional activities, exercises conducted and timing: pre-surgical or post-surgical [23]; early and intensive or long-term; in a dedicated centre or at home; in group or individual rehabilitation [24, 25, 26].
Some researchers studied balance in THA patients using proprioceptive platforms after a technological rehabilitation training: some studies reported CoP trajectories using posturography early postoperative [27, 28, 29], while others propose a long-term follow-up [30, 31]. Moreover, a recent meta-analysis investigated pain, risk of falls and quality of life related to balance and proprioceptive training on total hip and knee replacement [32]. Just few data are available about dynamic stability after hip replacement [33, 34, 35] but no one reports data about technological rehabilitation. At the present no research presents simultaneously the study of dynamic stability after technological rehabilitation treatment in patients with total hip replacement.
The higher improvement in our sample using the technological rehabilitation may also be ascribed to the fact that the therapist can follow the patient during rehabilitation more effectively, as well as correct any errors made by the patient and change the rehabilitation treatment according to progress or regression in order to optimize functional recovery. This type of rehabilitation can also be used to quantify improvements and the intensity of motor training; it allows the therapist to use a wide range of exercises, thereby improving compliance, as well as other technological systems, such as videogames. The most effective exercises are those performed when the platform is mobile. Indeed, platform instability provides continual alterations in balance, forcing the muscles and nervous system to keep adjusting themselves in order to maintain body balance. Consequently, the brain receives a continuous flow of kinesthetic information that improves proprioception, kinesthetic sensitivity and balance control. This type of rehabilitation also provides visual biofeedback that makes the patients aware of their movements and consequently allows them to modify their movement patterns accordingly.
In conclusion, our results suggest that rehabilitation after THA improves static balance. When proprioceptive technological rehabilitation is combined with conventional rehabilitation, an improvement in dynamic balance is also observed.
Footnotes
Acknowledgments
We would like to thank Claudia Loreti for her technical support.
Conflict of interest
None to report.