
Abstract
BACKGROUND:
Latent myofascial trigger point (LMTP) is a small hypersensitive area in skeletal muscles that becomes painful under compression or stimulation. LMTPs are relevant for various musculoskeletal disorders. Although several treatments have been introduced to treat LMTP, the most efficient one is yet to be found.
OBJECTIVE:
The main purpose of the present study was to compare pressure release, phonophoresis of betamethasone and dry needling on the upper trapezius latent myofascial trigger point.
METHODS:
Sixty participants (mean
RESULTS:
Significant pain decrease, active cervical range of motion and pain pressure threshold increase were observed in the three groups (
CONCLUSIONS:
Considering the significant, positive effects of all three methods, dry needling and phonophoresis seem to be more effective than pressure release.
Introduction
A myofascial trigger point (MTP) has been explained as a hypersensitive nodule in a taut band of skeletal muscle fibers [1]. These trigger points, which are a common source of musculoskeletal disorders, may be painful under stretching or compression. They may not only be a source of local/referred pain but also range of motion (ROM) restriction and muscle contraction deficiency [2, 3]. Clinically, MTP is classified as active and latent, and spontaneous local or referred pain can be a way to differentiate the two. The absence of any pain is defined as latent myofascial trigger point (LMTP) [4]. LMTP is also associated with movement deficiency, disturbance of reciprocal inhibition mechanism, and finally, muscle and joint overload [2, 5, 6, 7]. Additionally, LMTP increases the risk of patellofemoral pain syndrome, tension headache, shoulder pain and mechanical neck pain [8]. Managing cervical trigger points, specifically the upper trapezius as one of the most common trigger points, can be considered a crucial element in mechanical neck pain [9].
LMTP treatment includes invasive methods (local injection and dry needling) and non-invasive treatment (pressure release, stretching, laser and phonophoresis) [8, 10, 11, 12, 13, 14]. Positive effects of pressure release (PR) technique on pain reduction and ROM increment have been demonstrated [2, 12, 13, 15, 16, 17, 18, 19, 20]. Because of some possible disadvantages in PR techniques e.g., technique exertion, patient discomfort and therapist’s hand overloading, other methods (e.g. dry needling, phonophoresis and laser) have been introduced recently [4, 19]. Trigger point dry needling (DN) is a therapeutic intervention advocated for inactivating LMTPs [4]; some evidence suggests DN as an effective method [13, 14, 21, 22]. About 8.6 percent of patients reported at least one adverse effects (tenderness, soreness, local hemorrhage and pain) after receiving DN treatment [23]. In phonophoresis, another suggested treatment method, ultrasonic energy is used to enhance delivery of the medication through the skin. Although phonophoresis has been mentioned as an effective treatment method in a few studies, more investigations are needed [10, 18].
Although PR, DN and phonophoresis may provide improvements for patients, in most cases, treatment was limited to one session and a short period of time [10, 17]. Therefore, this study compares PR, DN and phonophoresis in an individual with upper trapezius LMTP through more than one session. Additionally, the effect of phonophoresis with betamethasone (PB) on LMTP treatment is measured for the first time in this study.
Method
Participants
This experiment included a study of 60 men (mean
Identifying LMTP
To find LMTP regions in each session, a predesigned transparency sheet (10
Outcome measurement
For each group, pain intensity, pain pressure threshold (PPT) and active ROM were examined by an expert physiotherapist in all sessions.
Cervical ROM
Active cervical ROM, including active contralateral lateral flexion (CLF), ipsilateral lateral flexion (ILF), contralateral rotation (CR) and ipsilateral rotation (IR) of the cervical spine was measured using a Cervical Range of Motion (CROM) instrument (Deluxe, USA) It is reported as a valid and reliable goniometer (intratester ICC
Baseline participant characteristics
Baseline participant characteristics
PPT was measured with a digital algometer consistedof a 1 cm width disk located vertically on the LMTP [18]. The algometer’s pressure increased gradually (1 kg/cm
Pain intensity
The visual analogue scale (VAS) is a 10 cm horizontal line used to evaluate pain intensity. Pain was measured by an algometer while 25 Newtons pressure was exerted over the LMTP. The reliability of this method was investigated and verified in other research [25].
Interventions
Randomization was achieved through use of a computer-generated random number table (Research Randomizer, version 4; www.randomizer.org). Total treatment duration was two weeks. Considering that DN repetition may disturb its effectiveness [4], the PB and PR groups had three, and the DN group had two treatment sessions per week. To have a better statistical curve, all variables were evaluated in each session and 24 hours after last treatment session.
Pressure release
Pressure was applied slowly and progressively by the algometer disk over the LMTP. Further pressure was applied when the self-reported pain was reduced to half. The procedure lasted about 90 seconds [12, 18]. In case of pain disappearance, the technique was stopped.
Dry needling
In this group, the LMTP was detected precisely, marked with a pen, and the skin was cleansed with an antiseptic. After skin preparation, a 0.25
Phonophoresis with betamethasone
Betamethasone solution was rubbed on the LMTP cleaned by alcohol. Ultrasound waves with 1.2 w/cm intensity and 60 percent duty cycle were applied by a Pulsed 1 MHz ultrasound unit (Enraf sonopuls 434, the Netherlands) for five minutes on the identified LMTP region. During treatment, the ultrasound applicator (with a 1 cm
Data analysis
A Kolmogorov-Smirnov test was used to determine normal distribution of the variables. One-way analysis of variance (ANOVA) was performed to determine whether there was a difference between the three groups in all variables. The data obtained was coded before analysis, and therefore, the analysis process was blinded. A repeated measurement ANOVA was used to assess the effects of treatment on all parameters. Partial eta-squared (
Comparison of changes in all variables over time for each treatment group
Comparison of changes in all variables over time for each treatment group
ILF
Among the 71 initial subjects, 11 were excluded because of jump sign (
Pain intensity
The ANOVA revealed that significant differences are present for the time factor (
Mean VAS values in 7 sessions for 3 treatments group. LSD test indicated significant differences between the DN and PB related to the PR groups (
Mean PPT values in 7 sessions for 3 treatments group. LSD test indicated significant differences between the DN and PB related to the PR groups (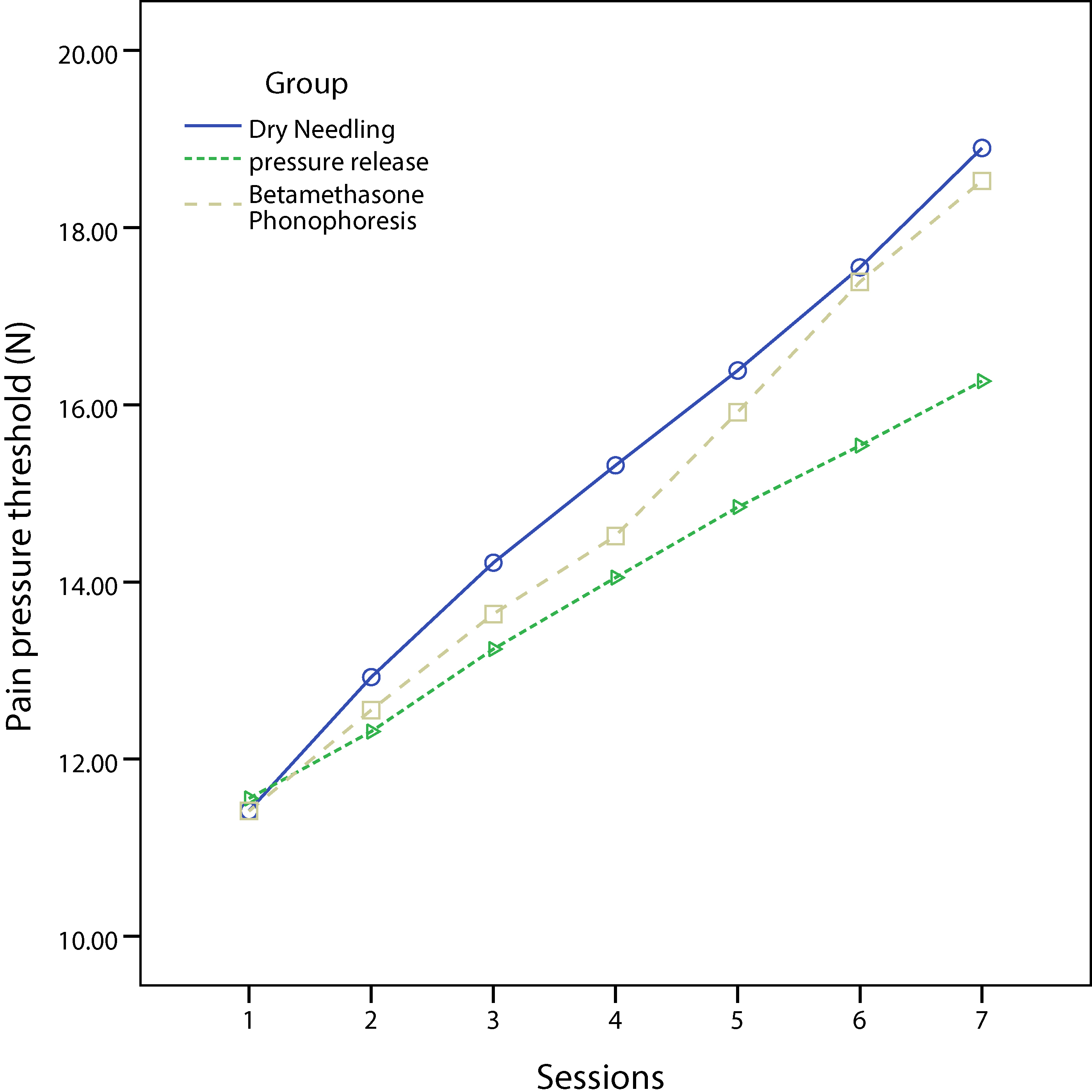
Mean CLF values in 7 sessions for 3 treatments group. LSD test indicated significant differences between the DN and PB related to the PR groups (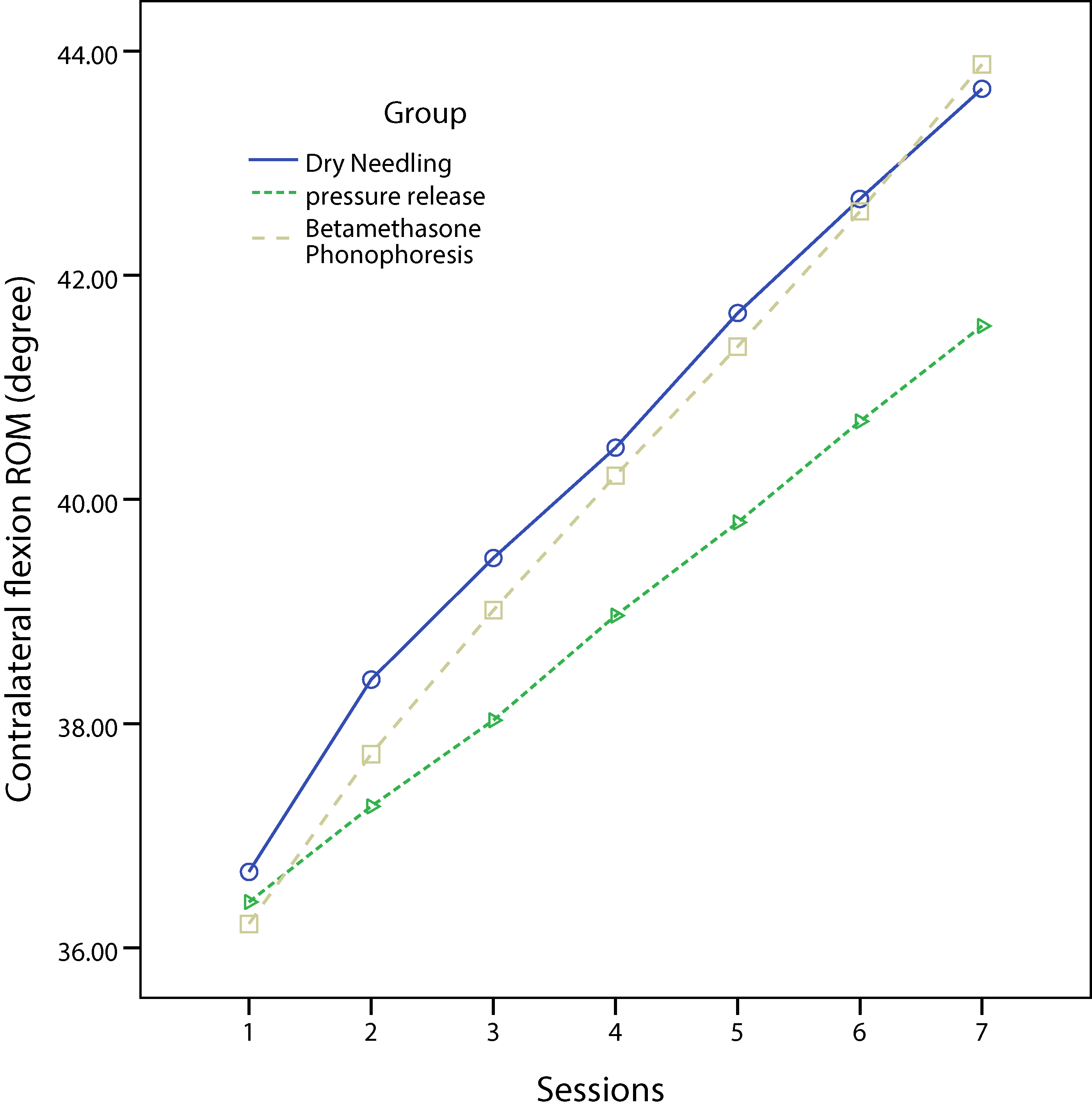
The ANOVA revealed significant differences are present for the time factor (
Range of motion
In this study, cervical ROM included ILF, CLF, IR and CR. The ANOVA test revealed that a significant time factor difference is present for ILF (
Discussion
LMTP and relevant symptoms
Although LMTPs are found in skeletal muscle fibers, they contribute to several musculoskeletal and nervous system disorders such as ROM restriction, muscle contraction inefficiency, accelerated muscle fatigability, motor control and autonomous system disturbance (Fig. 4) [2, 5, 14, 26, 27, 28]. Research has shown that LMTP could lead to tension increment and length restriction in skeletal muscles. Grieve et al. reported five-degree ankle dorsiflexion improvement secondary to treatment of active and passive myofascial soleus trigger points [2]. Zhang et al. recorded surface and intramuscular electrical activity before, during and after glutamate injection into different muscle points. Further, they reported significant muscle cramp and tension increment trigger points in comparison with healthy muscle points [28]. Interestingly, another study found a relationship between fatigue and LMTP in skeletal muscles [5]. Furthermore, an incorrect actin and myosin relationship in LMTP was reported as a cause of muscle physiological inefficiency leading to weakness without atrophy in skeletal muscles [5, 9]. Some studies have reported that motor control disorders such as early or delayed muscle activation before movement initiation, alteration in recruitment pattern and movement pattern disturbance correlated with the presence of LMTP [7, 26]. Other researchers have suggested a relationship between MTP and psychological and behavioral disorders [29].
Energy crisis, motor end plate and radiculopathy are three hypotheses that presented for myofascial trigger point formation. Myofascial trigger points also could contribute to several musculoskeletal disorders and nervous disorders.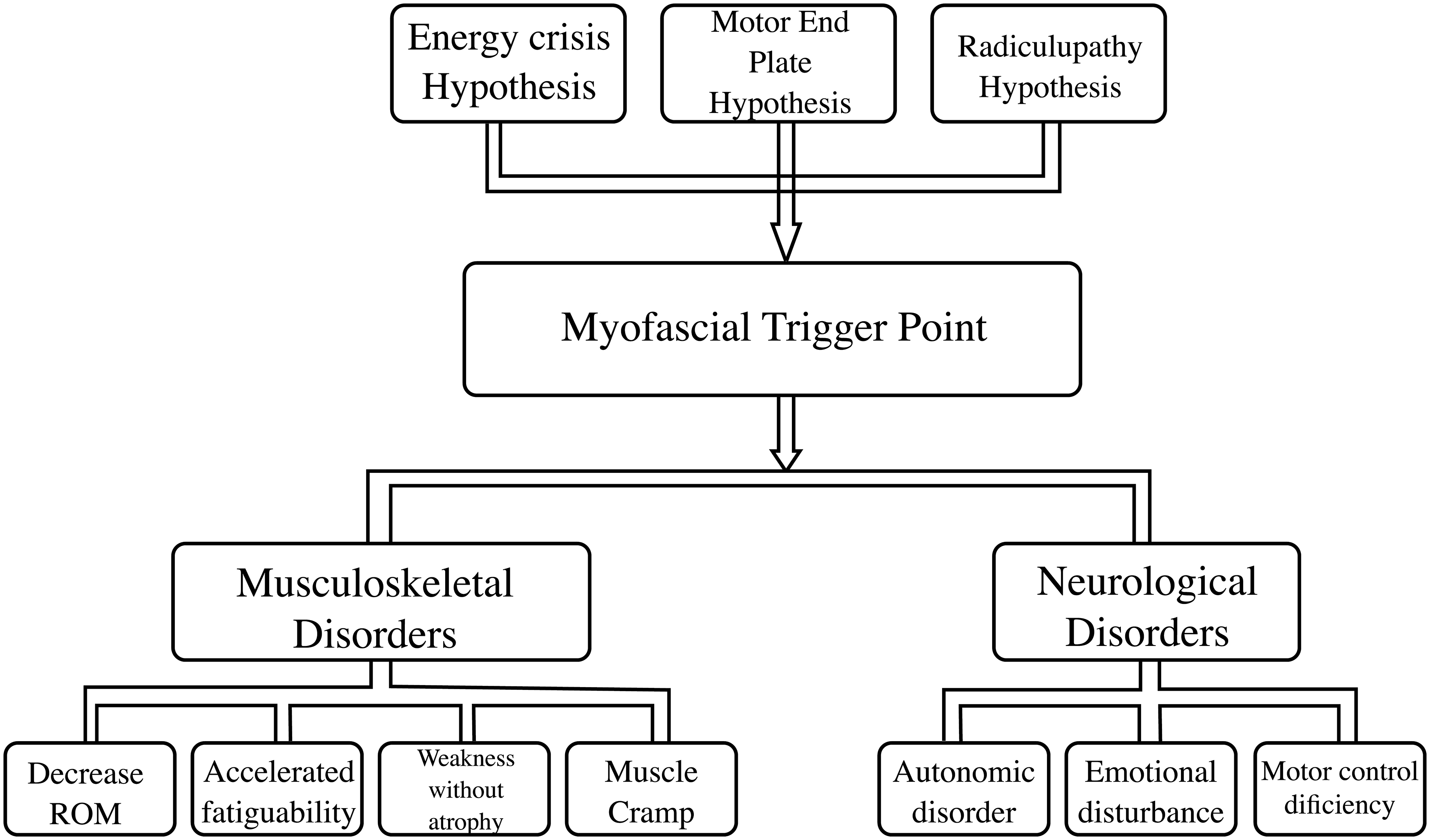
Energy crisis, motor end plate and radiculopathy are three hypothesized reasons for myofascial trigger point formation. Based on the energy crisis hypothesis, any muscular overload, including gradual microtrauma through changes in cellular membrane permeability, leads to a permanent sarcomere shortening, hypoxia and, finally, myofascial trigger point formation [1, 8, 9]. The motor end plate hypothesis was proposed to find the primary causes of the energy crisis hypothesis. In motor end plate hypothesis, excessive acetylcholine release from motor end plate on muscle and accumulation of pain-producing substance are major factors for myofascial trigger point formation. Gunn et al. developed the radiculopathy hypothesis, in which any nerve damage, including denervation and pressure on the nerve or nerve root, contributes to abnormal muscle tension and, finally, myofascial trigger point formation [1].
In this study, all PR, PB and DN groups had clinically significant improvements. Since patients with radiculopathy were excluded, the radiculopathy hypothesis would not apply in explaining the improvements in the present study. The finding of this study could be processed based on the energy crisis and motor end plate hypotheses Simons integrated in 2004. Simons showed several factors, such as correction of sarcomeres length, pain-producing substance reduction, ceasing energy crisis cycle and decreasing local hypoxia, should be attended in the treatment of LMTP [2, 18, 28].
The findings of the current randomized clinical trial suggest thatall three groups improved in pain score and PPT following treatment. Different mechanisms are proposed in pain alleviation [8, 18, 28]. The suggested mechanism in the PR technique is initial hypoxia followed by sudden blood supply increment. The final result would be pain-producing substance, local blood circulation correction and increased ROM [2, 17, 30].
Generally, mechanical and neurological aspects are considered as the dominant components to explain the changes found in the current study. Based on Simons’ findings and travelling theory, the mechanical effect of the needle will stimulate two healing processes, local muscle regeneration process and abnormal acetylcholine release cease about seven to ten days after treatment [1, 4]. Simultaneously, needle exertion itself could facilitate local stretching in the shortened sarcomere. Needle movement in muscle to optimize the effect might activate A-delta and C fibers. Such effect will remain as long as 72 hours after needle insertion [4, 8]. Also, prolonged stimulation of A-delta fiber might activate enkephalinergic, serotonergic and noradrenergic inhibitory system, implying that DN in LMTP could cause an opioid-mediated pain suppression mechanism. Intra-tissue mechanical disturbances of the needle cause pulling of collagen fibers toward the needle and initiate specific change in fibroblasts around the needle. The transduction of a mechanical signal into fibroblasts could lead to various intra- and extracellular events, leading to both sarcomere position and cellular function modification [4]. More research is needed to determine various aspects of DN mechanisms
Two significant effects of phonophoresis on LMTP contribute to ultrasonic waves and pharmacological aspects. The impact of ultrasonic waves on cells would result in a change of the outside cellular ion concentration. In other words, perhaps a transition increase in ions such as calcium might correct the sarcomere shortening in LMTP [18]. Betamethasone lotion is a safer steroid, anti-inflammatory agent and has the least side effects. Sarrafzadeh et al. revealed that phonophoresis of hydrocortisone, as an anti-inflammatory solution, was effective in the treatment of LMTP [18]. On the one hand, Ay et al. reported active myofascial trigger point phonophoresis with diclofenac had a significant improvement related to control group [10]. On the other hand, Shah et al. reported that while the level of inflammatory substance was evaluated in active myofascial trigger points, they found no significant difference between a patient with LMTP and healthy subjects [27]. Although the PB method was effective in LMTP treatment, probable ultrasonic wave side effects such as tissue destruction, blood cell stenosis and risk of tumor growth should be considered [18].
Cervical ROM
The findings of this study suggest that LMTP treatment increased cervical ROM. Some studies have shown that LMTP in a skeletal muscle could limit both inner and outer range of joint movement [2, 6, 7]. In this study, the upper trapezius muscle was shortened in ILF and CR (inner range) but lengthened in CLF and IR (outer range). Lucas et al. reported that LMTP could restrict inner active ROM of the muscle via decreasing contractile efficiency [7]. Additionally, some researchers proposed that LMTP could restrict outer active ROM of the involved muscles by increasing antagonist muscle activity and shortening the sarcomeres [2, 5, 6]. In the present study, both ipsilateral and contralateral movements (ILF, CLF, IR and CR) were significantly increased after the treatments in all groups.
Differentiation among the outcome of the three therapeutic methods
The present study’s findings suggest that DN and PB group subjects show greater improvement in pain, PPT and cervical ROM relative to the PR group after two week treatment. This difference may have its origin in a variety of therapeutic techniques. The direct access of ultrasonic waves and needle to LMTP may be considered as a rational reason to show a better result of PB and DN group relative to the PR group. In other words, tissue layers between LMTP and the location of manual pressure in the PR group may decrease the efficiency of this method. Generally, more research is needed to investigate the physiological effect of the DN and PB methods for treatment of LMTP.
Limitations
This study has a few limitations, including treatment of one muscle LMTP, lack of a control group, use of an objective device (e.g. diagnosis ultrasound) for outcome measurement and lack of including both sexes. These limitations should be considered in future studies. The comparison between DN, PB and PR was investigated for the first time in this study. Cervical rotation was also investigated for the first time.
Conclusion
In this study, although DN, PR and PB methods were effective treatments for LMTP, the effectiveness of DN and PB methods may be more significant in the treatment of LMTP. Also, no difference between was observed the DN and PB methods.
Footnotes
Acknowledgments
The authors would like to thank all subjects who participated in this study, without whose support this study could not have been completed.
Conflict of interest
None to report.