
Abstract
BACKGROUND/OBJECTIVE:
This study aimed to investigate performance (touch-coordinate errors, inter-touch interval) of touch screen technology in adolescents with unilateral spastic cerebral palsy (USCP) and healthy peers.
MATERIALS AND METHODS:
This prospective case-control study included 31 adolescents. The participants consisted of 15 adolescents with CP in the USCP group and 16 age-matched healthy peers in the control group. All participants performed an aiming-tapping task with an Android tablet. Four sessions were randomly applied: visual feedback (VF) and no VF with the dominant hand’s index finger (DHF), and VF and no VF with the non-dominant hand’s index finger (NDHF). Inter-touch interval (ITI) and touch-coordinate errors (TCE) were calculated.
RESULTS:
There were significant differences between the groups for VF and no VF-NDHF TCE and ITI (respectively
CONCLUSION:
This study provided insight into the touch screen performance of adolescents with USCP, who performed an aiming-tapping task with a tablet. Results showed that both affected and unaffected hand performance of touch screen tasks was impaired in adolescents with USCP.
Introduction
Cerebral Palsy (CP) is the most common paediatric neurological disorder and occurs due to brain damage during the early development process [1]. Unilateral Spastic Cerebral Palsy (USCP) is characterized by the motor and sensory disorders being dominant in one side of the body. USCP is the most common clinical type of CP constituting 42% of all CP [1, 2].
Despite the multiple factors in the ethology, common causes are middle cerebral artery infarcts, hemi-brain atrophy, neuronal migration abnormalities and periventricular lesions or post-haemorrhagic porencephaly [3]. The damage in the corticospinal pathway (which directly affects hand motor neurons that control selective upper extremity movements) and other motor pathways causes motor deficiencies such as muscle weakness in the upper extremity and absence of selective finger movements. USCP of middle cerebral artery origin can affect the somatosensory system and fine motor skills, especially in children [4]. Light touch, discrimination, stereognosis, proprioception and voluntary muscle activation are frequently disrupted. These children therefore have difficulty in coordinating and controlling movement, as well as using visual, proprioceptive and tactile information [5]. In addition, the disorder in motor planning affects fine motor skills [6, 7]. The functional disorder in the upper extremity observed in USCP has a negative effect on independence, employment opportunities, and inclusion in social and home environments [7].
Touch technology has become critical in many areas such as social life, communication, and personal or occupational activities. This technology is commonly used in shopping centers, airports, automated teller machines (ATMs), smartphones, computers and tablets [8]. According to 2011 data, the number of touch screen devices was expected to increase from 665 million in 2011 to 1,350 million in 2014 [9]. Furthermore 1.3 billion touch screen panels were shipped worldwide in 2012 and this is expected to consistently increase to 2.8 billion touch screen panels in 2016 (IHS DisplayBank). Devices with the ubiquitous touch technology are quite appealing to children and youth of all ages.
Despite ubiquitous touch screen technology, there are no studies on adolescents with USCP covering this subject. In the literature, limited studies investigated the touch screen performance of participants with disabilities [8, 10]. They proved that there are differences between disabled and non-disabled subjects in the performance of reciprocal tapping and the characteristics of touch [10]. In another study that evaluated touch screen performance in two groups, with and without disabilities related to motor control including subjects with cerebral palsy (CP), Huntington’s disease (HD), multiple sclerosis (MS), Parkinson’s disease (PD) and tremor [8]. The performance was found to be directly related to the button size. These results indicate that touch performance is different in subjects with a motor control disorder and healthy individuals.
The current study on touch in adolescents with CP is important because of the deterioration of motor skills in these individuals. Other studies have reported variances in touch characteristics such as dwell time, impulse and force in subjects with disturbed touch performance [10]. Various skills of children with USCP have become increasingly important for the use of touch technology [11].
Measurement of touch screen accuracy may be useful in the treatment of USCP as it can provide important information on touch skills. Quantification of these skills might help in i) the selection of therapy style and duration, ii) the grading of USCP regarding the upper extremity, hand and related motor skills, and iii) new therapy development for the improvement of related motor functions. Comparison of touch performances of adolescents with USCP and their healthy peers might help implement the above. This study therefore aimed to evaluate the touch technology usage skills of adolescents with USCP and their healthy peers. Our hypothesis was that the error rates and completion time in using a touch screen would be higher in adolescents with USCP, in both the affected and unaffected upper extremity, than that of their healthy peers.
Methods
Participants
A and B show the software’s cross signs with (B) and without visual feedback (A). C shows a subject during a recording session.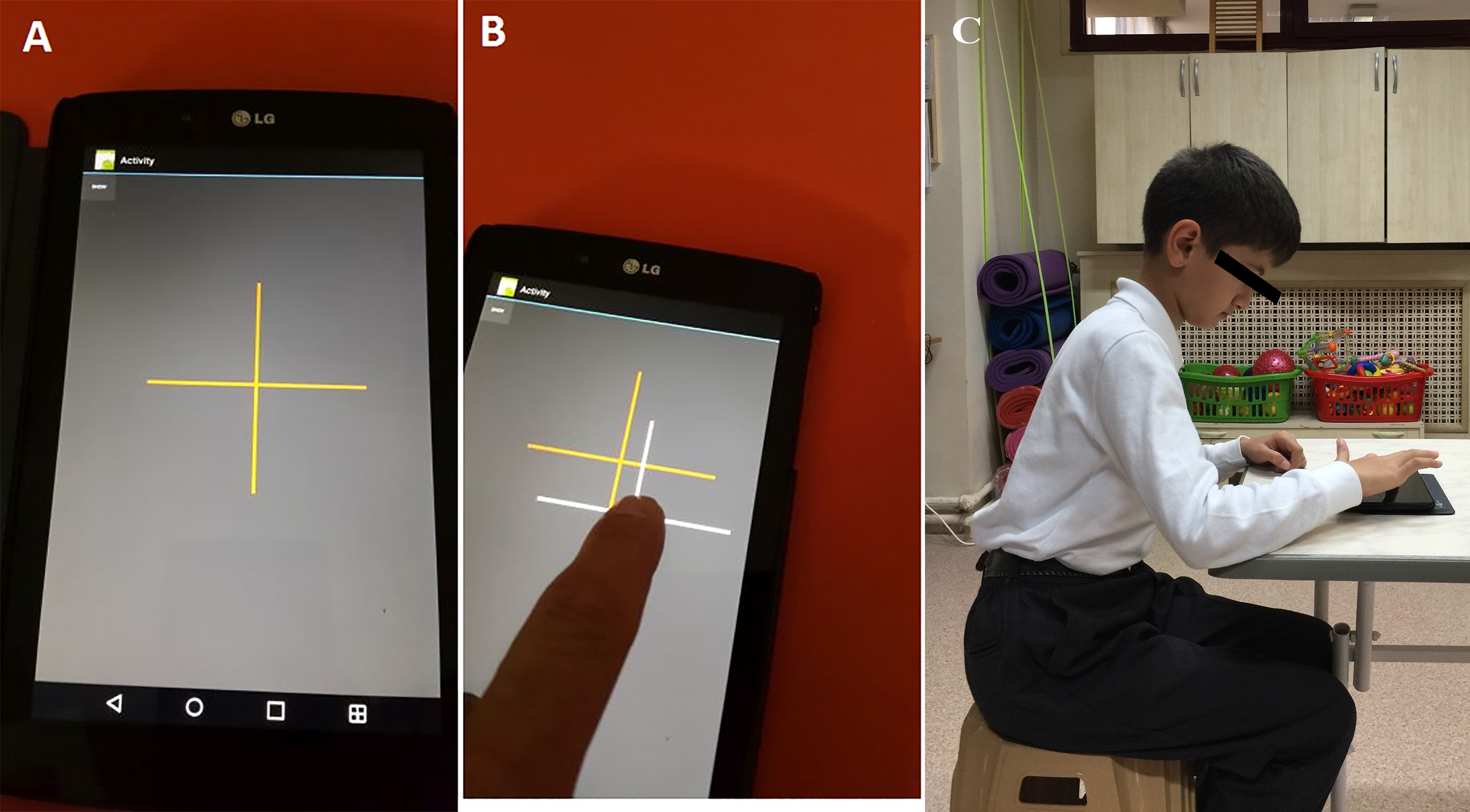
This prospective case control study included a total of 31 adolescents and took place between September 2015 and November 2015 at the Department of Physiotherapy and Rehabilitation of Hacettepe University. Fifteen adolescents with a USCP were chosen for the USCP group and 16 healthy peers were chosen for the control group. Age and gender distribution was similar in the two groups with both groups consisting of adolescents between the ages of 10 and 15 years. The adolescents had to be able to follow and accept verbal instructions, and should have no visual impairment. Exclusion criteria for the USCP group were: (1) levels IV and V of the Manual Ability Classification System [12]; and (2) orthopedic surgery or botulinum toxin injection in the past six months. The children with CP had no muscle soreness and stiffness that could prevent the hand function. Adolescents whose parents/guardian refused to participate were also excluded from the study. Permission of the University Ethics Committee was received and written informed consent was obtained from each participant and/or parent. The study was performed in accordance with the Helsinki Declaration.
The Gross Motor Function Classification System Expanded and Revised (GMFCS E&R) and Manual Ability Classification System [12] levels of the children were classified by the first author, a physiotherapist with eight years of experience in pediatric rehabilitation [13, 14].
Body composition
Body composition was evaluated by body mass index (BMI) calculated with the formula of weight in kilogrammes divided by the square of the height in meters. Weight was measured with a standard electronic device and height with a stadiometer.
Experimental task
All subjects were seated on a chair in front of a table (Fig. 1C). The chair’s height was adjusted to allow each subject to place an elbow on the surface of the table. The subjects could comfortably press the Android tablet’s screen (LG G Pad 7: 7” touch screen, Android OS 5 tablet computer) (Fig. 1C). A native Java-based Android software was developed to display cross signs. The lines of the signs were 56 mm long and 1 mm thick (Fig. 1A and B) on random coordinates of the screen. After a red-colored cross sign was displayed, the software recorded the touch point’s coordinates and the time until the participant touched the screen. This produced a beeping sound to give the user auditory feedback that the touch was detected. The authors could also set the software to provide visual feedback (VF) through the display of a white cross sign rather than a red one. The VF was coordinated to occur simultaneously with the auditory feedback (Fig. 1B).
The software could quickly be used in two modes: VF and no VF. The software displayed random cross signs after each touch. First, each user tried both VF and no VF sessions by using index fingers for a few minutes to adapt to the device and the task. Then, four sessions were randomly applied: VF with the dominant hand’s index finger (DHF), no VF with DHF, VF with the non-dominant hand’s index finger (NDHF), and no VF with NDHF. At least 40 touches were recorded consecutively in each of the four sessions. A rest period of 3–4 minutes was provided between each session. The recordings from the USCP and control groups were assessed by the second author.
The mm distances between the centers of the displayed red crosses and the actual touch points were calculated as touch-coordinate errors (TCE) for all sessions (
Physical characteristics of the subjects
Physical characteristics of the subjects
Inter-touch intervals (ITI) were calculated using the time-intervals (ms) between two consecutive touches. The ITI values were calculated for each session [15].
The Statistical Package for the Social Sciences (SPSS) version 21 for Macintosh (IBM SPSS Statistics; IBM Corporation, Armonk, NY, USA) was used to analyze the obtained data. One-sample Kolmogorov-Smirnov Tests were used to evaluate distribution of variables before test selection. Descriptive analyses were presented using medians and the interquartile ranges (25%–75%) for the non-normally distributed and ordinal variables. Differences in physical characteristics between the USCP and control groups were analyzed using the
Results
The subjects consisted of 15 adolescents with USCP in the USCP group (seven males, eight females; mean age 12 y 4 mo (SD 2 y 8 mo), range 10–15 y) and 16 age-matched healthy peers in the control group (eight males, eight females; mean age 12 y 3 mo (SD 2 y), range 10–15 y). Descriptive statistics are shown in Table 1. Baseline data showed the groups to be well matched in terms of age, height, weight, BMI and gender.
Investigation of the effect of variables on TCE and ITI
Table 2 presents the effect of independent variables such as group, age, BMI, GMFCS and MACS on TCE and ITI. The group variable had an effect on the TCE value as with VF-DHF, no VF-DHF, VF-NDHF and no VF-NDHF (
Evaluation of group, BMI, age variables on TCE and ITI by linear model
Evaluation of group, BMI, age variables on TCE and ITI by linear model
There was no significant difference of the GMFCS vs MACS classifications on the TCE and ITI values in the USCP group.
Table 3 presents median TCE and ITI in the USCP and control groups and their comparison. There was no statistically significant difference between the VF-DHF and no VF-DHF TCE and ITI values in either group. There was also no significant difference between the VF-NDHF and no VF-NDHF TCE and ITI values in either group. We found no effect of visual feedback on TCE and ITI values in the two groups. Figure 2A and B show TCE and ITI values for all four sessions.
Within-group touch-coordinate error (TCE) and inter-touch interval (ITI) values of each session comparisons
Within-group touch-coordinate error (TCE) and inter-touch interval (ITI) values of each session comparisons
A. Median touch-coordinate error (mTCE) values of each session are displayed. B. Median inter-touch interval (ITI) values of each session are displayed.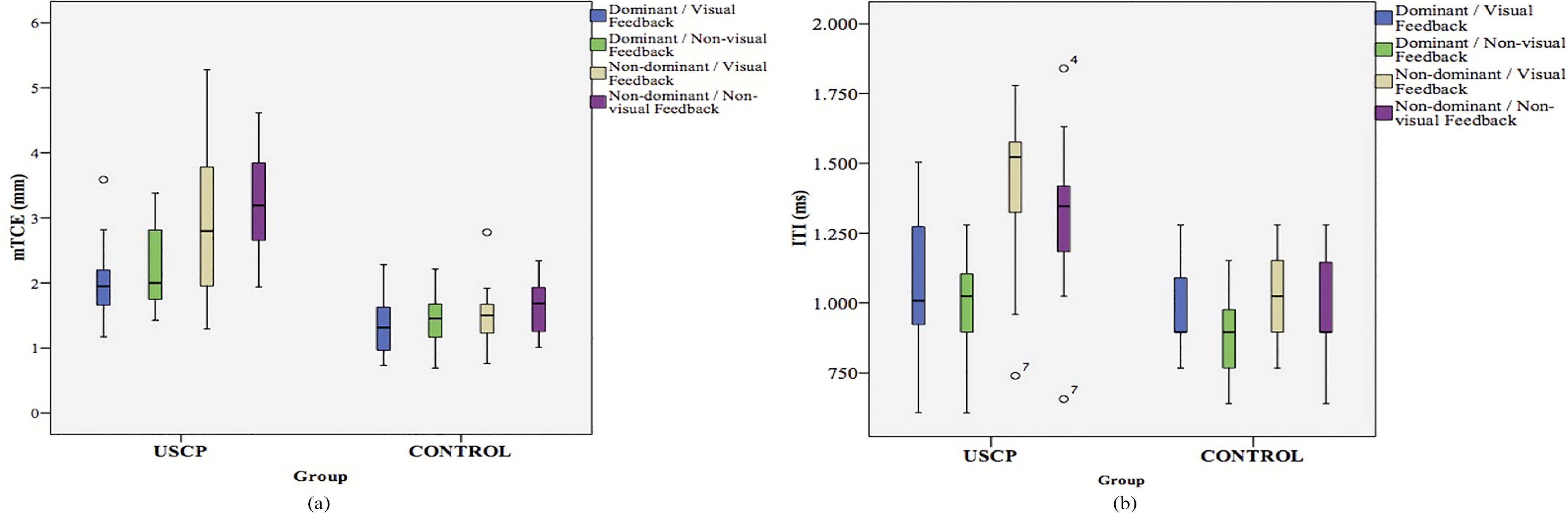
There was no statistically significant difference between ‘VF-DHF and VF-NDHF’ and ‘no VF-DHF and no VF-NDHF’ ITI and TCE values in the control group. There was also no hand dominance effect on TCE and ITI in the control group.
When we compared the unaffected (dominant) and affected (non-dominant) hand in the USCP group, there was no difference in TCE values with VF, but a statistically significant difference was present without VF (
There was a statistically significant difference between the groups for VF-DHF TCE values (
Between-group touch-coordinate error (TCE) and inter-touch interval (ITI) values of each session comparisons
Between-group touch-coordinate error (TCE) and inter-touch interval (ITI) values of each session comparisons
A statistically significant difference also existed between the USCP group and the control group for no VF-DHF TCE values (
This is the first reported study on the use of touch screen technology by adolescents with USCP. The most important finding of our study was that the TCE of both the DHF and NDHF of the adolescents with USCP with or without a VF were higher than their healthy peers. Another important finding was that there was no difference on the affected and non-affected side TCE with VF while the TCE was increased in the unaffected side when VF was not present in the USCP group. Similarly, Soylu et al. [15] demonstrated that the visual feedback decreased the incorrect entry and centring error in health adults while using a smartphone.
The selection of the age group is very important for the studies on the fine motor skills of children related to touch screen technology. Other studies have demonstrated that the “fingertip coordination” reaches the adult level between the ages of six and eight, and the coordination of grasp-drop strength reaches the adult level between the ages of eight and ten [1, 16]. We therefore determine the threshold for this study as the age of 9, when the fine motor skills reach maturity.
Postural control comprises the protection of balance, the control of body position in space, the relationship between the body segments, and the relationship of the body with the environment for its tasks [17]. Postural support is therefore important in order to perform cognitive tasks, especially for children with CP who have postural control deficiency. Chourasia et al. [17] found that the completion time and error rate increased during the standing task in their study on the effects of sitting and standing on touch performance. We therefore tested the adolescents with USCP in a sitting position during the aiming-tapping task in order to better demonstrate their upper extremity skills.
Various studies in the literature on the limitation in upper extremity skills of children with USCP have focused on different aspects such as sensation, motor learning, neglect and proprioception. Auld et al. [18] found that the tactile function of the affected hands of children with USCP were worse than either hands of healthy children. This was demonstrated in their study on the tactile functions of 52 children with USCP and 34 healthy children between the ages of 8 and 17 years. In addition, they indicated that the non-affected hand also had tactile impairment in approximately 53.8% of the children with USCP while their results indicated no difference between the dominant and non-dominant hands of healthy children [18]. We similarly found in this study that the TCE rate was 1.3 times higher in the NDHF of adolescents with USCP, both with and without VF, compared with the control group. Wingert et al. [19] found the error rate to be higher than the control group in their study on fixed position sense in children with CP with and without visual support but this difference was not statistically significant. They reported the position sense error to be twice as high in the group with CP than the control group [19]. We did not evaluate proprioception in this study but the TCE rate in NDHF was 1.8 times higher in the group with USCP. Wingert et al. [19] found the error rate to be lower in both the dominant and the non-dominant sides with visual support and stated that vision adaptation was necessary for learning and practicing movements in individuals with CP. Similarly, our findings showed the importance of VF as the TCE rate was 1.5 times higher without VF on the affected side, while we found no difference with and without VF in the dominant upper extremity in adolescents with USCP. VF resulted in a decrease of TCE in both hands while this decrease was more prominent on the affected side in the USCP group. The limitation in upper extremity fine motor skills have indicated that visual support is important for these subjects when using touch screen technology. However, the ITI duration was longer for both hands, with or without VF, than in a healthy group. We believe the time parameter that can influence performance of a movement could also affect technology use of children with CP.
There are only a few studies in the literature on the use of touch technology by individuals with motor disorders and these have focused on adults. The main strength of our study is that it is the first to investigate the use of touch technology, which is used almost everywhere today, by adolescents with USCP. Chen et al. [8] studied the effect of button and space dimensions on the use of touch technology by individuals with various motor skills. Their study included 38 adults with motor disorders such as CP, Huntington’s Disease, Multiple Sclerosis, Parkinson’s Disease and tremor and 15 healthy individuals. They proved that the impaired group made 2.9 times more mistakes and tasks took 2.2 times longer [8]. Irwin and Sesto [10] separated 37 individuals with motor disorders into gross (CP and Huntington’s Disease) and fine motor control groups in their study on the touch characteristics and performances of individuals with and without a movement disorder. The group with a gross motor disorder tapped 2.8 times less than the healthy control group during the reciprocal tapping task and the group with a fine motor control disorder tapped 1.8 times less [10]. The average dwell time was longer (0.21
Limitations
One of the limitations of this study was that we did not evaluate the effects of the aiming-tapping task on dwell time and impulse parameters. Future studies should focus on investigating the effects of dwell time and impulse in adolescents with USCP. Another limitation of this study was the small amount of participations. Future studies should include a large sample size to evaluate touch performance of adolescents with USCP. In addition, in this current study, we included adolescents with USCP with Levels I, II and III of MACS. Researchers should investigate the touch screen performance in more involved children with CP.
Conclusion
Touch technology is now indispensable. It has therefore become important to identify the difficulties of using touch technology for adolescents with CP. This identification is necessary in order to help them become involved in the society. This study has proven that there are delays in the use of touch technology with both the affected and non-affected hands of adolescents with USCP, compared to their healthy peers. In light of these results, the functions of the non-affected upper extremities should also be focused on the clinic, in addition to the affected upper extremities. We believe using visual support during the rehabilitation program will increase the effect of the treatment. Insight into using touch technology in adolescent with USCP, clinicians should involve touch technologies in their upper extremity rehabilitation programs to improve participation of adolescent with USCP.
Footnotes
Conflict of interest
The authors have no conflict of interest to declare.