
Abstract
BACKGROUND:
Prolotherapy (PrT) is an increasingly popular regenerative injection treatment for the management of musculoskeletal injuries. The diagnostic injection is a method for selecting suitable patients to apply PrT using subcutaneous 5% dextrose solution.
OBJECTIVE:
The study aims to assess the PrT usage and modifications in the treatment of chronic low back pain and lumbar disc herniation and to define diagnostic injection procedure for PrT.
METHOD:
Two thousand three hundred and eighty-two patients with low back pain or lumbar disc herniation were evaluated at the Traditional and Complementary Medicine Practice Center in Ankara, Turkey. Six hundred fifty-four patients were included in the study. Diagnostic injections were performed on all patients who were thought to be eligible candidates for PrT indications. A 4-or-6 week interval was allowed between treatment sessions.
RESULTS:
Xix hundred and fifty-four patient treatments were completed. The Visual Analogue Scale (VAS) scores decreased to 5.1
CONCLUSION:
PrT can be regarded as a safe way of providing a meaningful improvement in pain and musculoskeletal function compared to the initial status. Diagnostic injection is an easy way to eliminate patients and may become a favorite treatment modality. 5% dextrose is a more simple and painless solution for PrT and also has a high success.
Introduction
Prolotherapy (PrT) is an increasingly popular regenerative injection treatment used for healing damaged or degenerated connective tissues (i.e., ligament, tendon, cartilage) [1, 2, 3, 4]. Its use began in the 1930s [5] and includes irritant solution injections into tender ligamentous/tendinous attachments. In the 1950s Hackett determined protocols of injection derived from his clinical experience [5, 6].
Chronic musculoskeletal pain improves due to inadequate repair of connective tissue following an injury [6]. Also, pain and disability are frequently derived from these degenerated structures, and PrT can stop or reverse these degenerations at the tissue level [3, 6]. The reduction and regeneration mechanisms of pain are not clear yet [1, 2, 7, 8], but can be defined as the effect of local inflammation or impulse of local growth factors’ release or down-regulation of neuropathic inflammation or a combination of all [2, 7].
Hypertonic dextrose is the most common injection solution used in trials [1, 7, 9]. Irritant solutions can cause osmotic rupture of local cells and increase growth factors from these different types of human cells. Further, a hypertonic environment can cause the release of DNA-encoding growth factors [3, 7, 10]. Also, varied irritant solutions stimulate fibroblast cells. Growth factors enable fibroblasts to be activated and released. These activated fibroblasts secrete new collagen fibrils necessary to repair damaged ligaments/tendons that promote healing [4, 6]. PrT can improve stability by tightening and strengthening the joint stabilizing structures [4, 6, 11]. Improved joint stabilization can contribute to tissue healing by increasing local blood flow and excitability of mechanical receptors and decreasing the excitability of pain receptors [3, 6].
Enthesofascial (EF) PrT is known as the classic method. The bony cortex/enthesis and joint space are the locations of injections. Myofascial (MF) PrT is the injection of specialized soft tissue which overlies the bony cortex and is below the subcutaneous fascia. The indications are musculotendinous degeneration, intrasubstance tendon or muscle tears, and fascial defects that prevent muscle function. The neurofascial (NF) PrT is the injection of the regions close to peripheral sensory nerves and especially these nerves’ fascial penetration points from where they reach the subcutaneous area. The aim of PrT is soft tissue repair or functional restoration, but NF PrT provides restoration of function rather than proliferation in small nerves. The reparative proteins and their teamwork for nerve repair are not well-known, but nerves can be said to be largely collagen-based by structural overlapping with ligament and tendon components (i.e., perineurium and epineurium). Nerves are designed to react in a similar series of growth factors; thus, they may be involved in soft tissue repair mistakes. Dextrose is thought to be potentially therapeutic for small nerves [3, 11].
There are no specific guidelines or published clinical trials showing a meaningful difference in treatment protocols for PrT [5, 11, 12]. The current study aims to evaluate the PrT usage and modifications in the treatment of chronic low back pain and lumbar disc hernia and to define diagnostic injection procedure for PrT.
Materials and methods
The study was conducted at the Traditional and Complementary Medicine Practice Center, Gulhane Training and Research Hospital, University of Health Sciences, Ankara, Turkey, whiched opened in January 2017. A physician (IS) with 12 years of clinical experience administered the injections and modified the practice. The local ethics committee approved the study protocols (no. 19/104).
Subjects
Between January 2017 and January 2019, 2382 patients with low back pain or lumbar disc hernia were evaluated. The treatment was not approved for 112 of them; 650 patients were given an appointment date for the first treatment session, 854 patients were continued, some of the patients were excluded due to other reasons shown in Fig. 1, and 654 patients whose treatments completed were included in the study. Demographics of patients who completed treatments are shown in Table 1.
Demographics of patients
Demographics of patients
LBP: Low back pain; LDH: Lumbar disc hernia.
Flowchart of the study.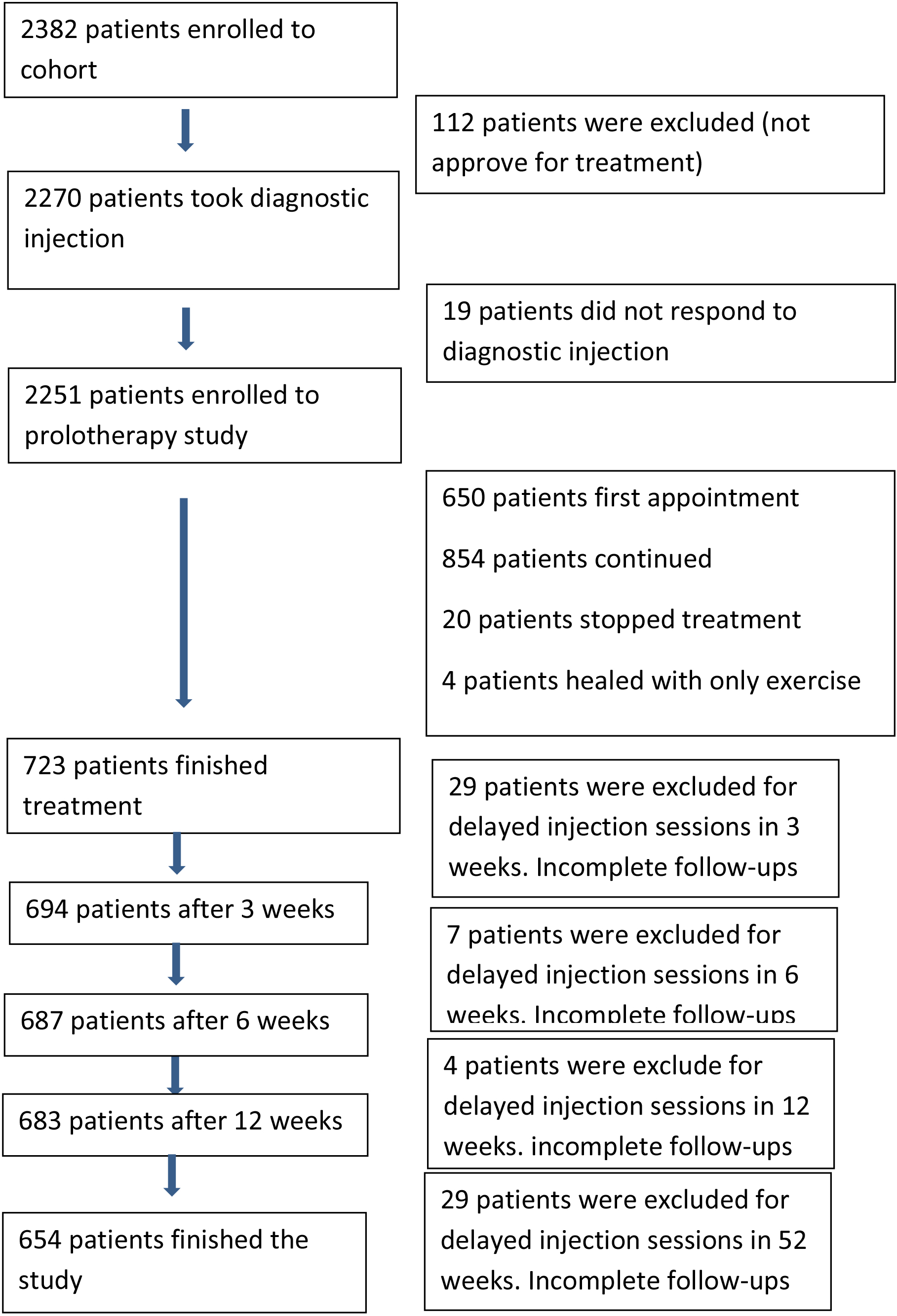
The exclusion criteria are immunodeficiency, cancer, active inflammatory/connective tissue disease, unstable hypertension, active endocrine/neurological disorder, pregnancy and anticoagulant usage.
The description of diagnoses was based on instability and pain with the palpation of ligaments’ reflecting points on whether or not the presence of lumbar disc protrusion in the magnetic resonance imaging (MRI). Primary outcomes for improvement of pain were described as no pain feeling with palpation and lower than 2 of VAS scores. Poor clinical results were determined as pain feeling with palpation and higher than 2 of VAS scores.
Three points diagnostic injections were applied to all patients who were found to be eligible for the treatment. 5% dextrose solution was injected subcutaneously. These 3 points correspond to A, B, C points of the posterior sacroiliac ligament for low back disorders (Fig. 2) as defined by Hackett et al. [6]. After the injections, patients rested for 15 minutes and were then re-evaluated. If the patients’ pain was considerably reduced or a relief seen in the related joint movements after 15 minutes, the patients were included in the PrT treatment list.
3 points of the low back region (red circles).
For the PrT injections, 22-gauge, 1.5”-long needles and 5% dextrose solutions were used. PrT injections were performed by Hackett’s procedures [6]. The patient was in a prone position, and a pillow was placed under the abdomen. Two ml of 5% dextrose was injected into the posterior sacroiliac ligament, iliolumbar ligament, transverse ligament insertions, transverse processes of L1-L2-L3-L4-L5-S1 vertebrae bilaterally in case of tenderness. The patient waited for 4 or 6 weeks to the subsequent injection session due to the tissue repair process. All material preparations and injections were performed by the same physician (IS) in the same center. The hot application was prescribed for 10 minutes each 2 hours when they had pain after the injection.
All patients were reminded to avoid taking non-steroid anti-inflammatory drugs and limiting the overuse of painful joint at each appointment during the treatment period. All patients were prescribed a standard home exercise program, including range of motion, stretching, and strengthening exercises for four weeks.
The percentage of VAS scores in 52 weeks.
Patients started the exercise program three days after the injection. Range of motion and stretching exercises were used at the beginning of the program. After two weeks, strengthening exercises were adjoined to the program. Education was given to patients about exercise programs.
Statistical analysis
All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) version 20.0 for Mac (SPSS Inc., Chicago, IL, USA). Continuous variables were shown as mean
The differences of VAS scores in each follow-up section
The differences of VAS scores in each follow-up section
The number of patients in the differences of VAS scores frequencies at each follow-up section
The difference of VAS scores before and after diagnostic injections.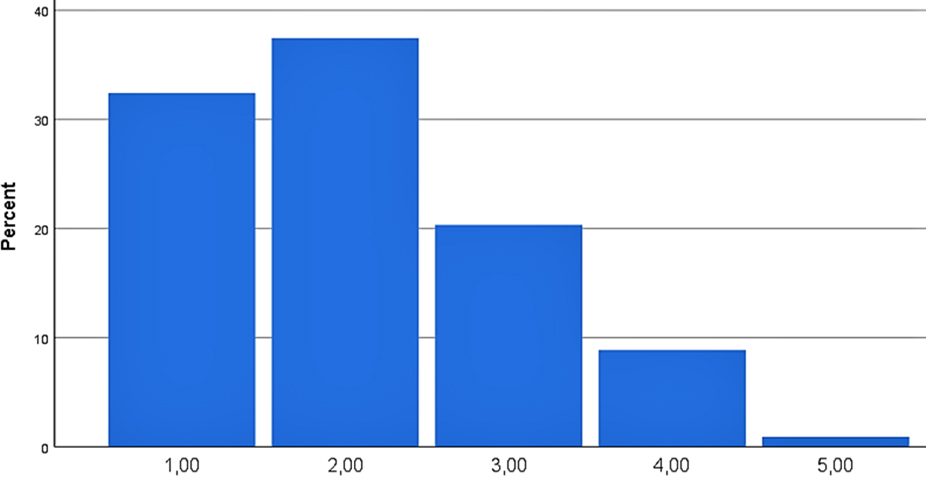
The difference of VAS scores before and after treatment.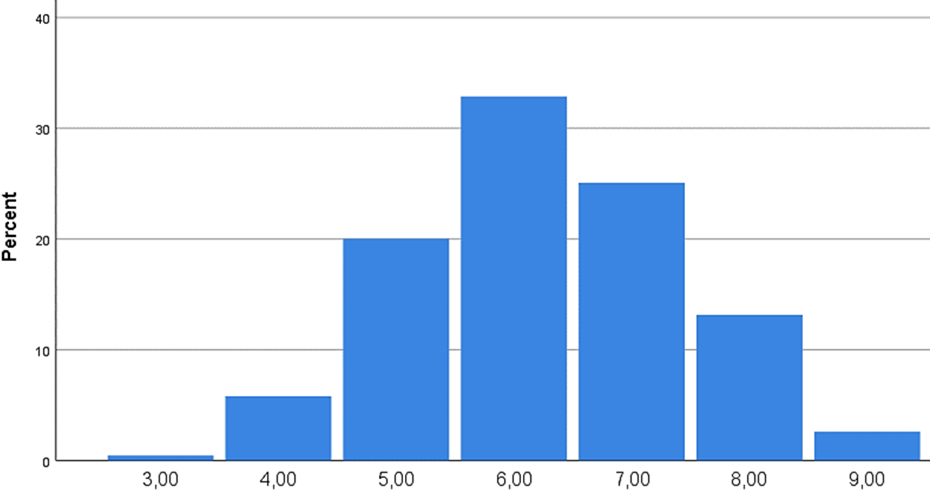
Two thousand three hundred eighty-two patients were evaluated. The results of diagnostic injections of 19 patients were insufficient, so they were not accepted to treatment. Six hundred fifty-four patients’ treatments were completed. The VAS scores decreased to 5.1
Discussion
PrT has been shown to be one of the most successful regenerative injection methods as it uses different concentrations and combinations of dextrose [13, 14, 15]. For the treatment of musculoskeletal problems, we used 5% dextrose without adding local anesthetics and obtained successful results as stated by the previous studies in which hypertonic dextrose with local anesthetics was preferred. Hence, we achieved the same effectiveness by avoiding the possible side effects of local anesthetics.
Diagnostic injections have not been mentioned in PrT studies in the literature yet. We have defined a 3 points diagnostic injection for the low back. Diagnostic injections have been performed to assess the origin of the patient’s pain. If the pain was originated from ligaments, the diagnostic injection would work at that moment; but if the pain was reflecting from another region, the reflected pain could not be treated with this injection method. Correct patient and indication selection, repetitive injections, and long-term patient follow-up are critical success factors.
In our study, we observed high pain relief rates, which may depend on diagnostic injections. The needles used in injections cause traumatization so that focal bleeding may induce an inflammatory response, which may induce the healing mechanisms [16]. This process cannot be completed within 10 minutes, but a decrease in pain and comfort in movements occurs. Relaxation of the fascia, the gate-control theory, or the placebo effect might be the real reason for the success of PrT. Perhaps it causes relaxation of the fascia overlying the ligaments that correspond to the three points, thereby relieves the pressure above. According to the gate-control theory, it can be said that the original pain is suppressed and reduced by creating a new pain [17].
In previous studies, 5% dextrose was used for short-term pain relief. However, no study focused on its long-term therapeutic effects. Kim et al. compared the efficiency of dextrose, saline, and lidocaine in 64 patients with typical myofascial pain [18]. Mean VAS scores were not considerably different in each group before and after the injection. However, after seven days, only superficial 5% dextrose injections showed significantly lower scores. The mean pressure threshold, before and after the injection, was not different in the three groups. After seven days, the superficial 5% dextrose group demonstrated a meaningful higher value. Superficial 5% dextrose injections for sensory nerves decreased trigger point-related pain more than lidocaine [18, 19]. We used 5% dextrose for diagnostic injections similar to this study. Dextrose might act on sensory afferent nerves related to chronic musculoskeletal pain in such ways that can be detected by patients as relaxation and decreased pain with movements [19]. Maniquis-Smigel et al. investigated the short-term effectivity of 5% dextrose in chronic low back pain [20]. In their randomized double-blind controlled study, thirty-five patients had low back problems that caused reflecting pain in the gluteal region or legs for at least six months. A single epidural 10 mL injection of 5% dextrose and 0.9% saline were compared. 84% of the dextrose patients and 19% of the saline patients noticed pain reduction by four hours at a
Considering the mechanism of PrT, only one body region should be injected in a session. If there is more than one injured region to be injected, the clinician should choose. In our clinic, the treatment was started from the low back region first. We believed that the effectiveness of general treatment would increase if healing of the body core was achieved first. The core is the anatomical and functional centerpiece and the dynamo of the body [21]. The core is responsible for the transmission of force between the upper and lower halves of the body [22, 23, 24]. All motions are created from here, then transferred to the extremities [24]. Morphological studies support our clinical practice [25]. Tsuji et al. [26] observed a relationship between sacral inclination-knee flexion contracture and patellofemoral pain syndrome. They claimed that the primary source of this process is the low back alignment problem and defined this condition as a spine-knee syndrome. So, if the treatment is started from the core, the healing of other regions would be faster and for a longer period.
Hypertonic solutions (12.5–30%) have been frequently used for trials and recommended in books published up to now for PrT treatment. Concentrations of dextrose solution higher than 10% have been proposed to create inflammatory response and proliferation. Jensen et al. [27] designed an animal study to determine optimal concentrations and claimed that only concentrations below 10% stimulate the proliferation of cells; however, they do not have any effectivity on the inflammatory process histologically. An adult fibroblast culture study demonstrated that 5% dextrose increased gene expression in angiogenetic and apoptotic factors [28]. In most studies, it is declared that some patients experience extreme pain and fatigue after the injections due to an inflammatory reaction, moreover become unable to tolerate and decide to give up [13]. In our study, few of the patients complained of pain and fatigue. Our results are similar to the previous studies in which higher dextrose concentrations are used for the same indications. We believe that 5% dextrose should be a more comfortable, patient-compliance-enhancing treatment occasion with a similar clinical achievement rate. This is the first study using 5% dextrose solution PrT in the literature.
In other studies, PrT solution was a mixture of hypertonic dextrose and local anesthetics [13]. The experimental studies have shown that local anesthetics inhibit collagen synthesis, retard and disturb wound healing in this way [29]. Superficial 5% dextrose injections have been considered to be more effective than lidocaine for trigger point-related pain relief [18, 19]. We used %5 dextrose to have both proliferative and local anesthesia efficacy in light of these findings.
The success of the treatment has increased significantly as a result of the diagnostic injections. Surgery is recommended when all other conservative treatments fail to yield results. We also recommend surgery for patients whose diagnostic injections are failed.
The majority of patients have continued their exercise program. There are conflicting results of studies using PrT and exercise for chronic low back pain in the literature. In a randomized controlled trial with 2
Limitations of our study are the lack of a placebo control group and randomized controlled design. Therefore, randomized controlled studies are needed.
Conclusion
PrT can be regarded as a safe way of providing significant amelioration in pain and musculoskeletal function compared to the initial status. The diagnostic injection is an easy way to choose appropriate patients for PrT. 5% dextrose is a more simple and painless solution for PrT, also has a high success. More studies may light up the dark sides of this procedure by defining the diagnostic injections for other parts of the body and the content of solutions.
Author contributions
AO, IS, OK: Data curation, Writing-Original draft preparation, Visualization, Investigation, Supervision. IS: Conceptualization, Methodology, Software, Validation.
Funding
The authors received no financial support for the research and/or authorship of this article.
Footnotes
Conflict of interest
The authors have no conflicts of interest to declare.