
Abstract
BACKGROUND:
Shortening of tensor fasciae latae is one factor that causes a functional leg length discrepancy. A shoe lift has been used to correct the compensatory posture resulting from the discrepancy. Despite the potential therapeutic benefit of a shoe lift, the mechanism by which it exerts its effect is unclear.
OBJECTIVE:
To investigate the effect of a shoe lift on tensor fasciae latae length during standing with an artificial functional leg length discrepancy using ultrasonic shear wave elastography.
METHODS:
Twenty-two healthy individuals performed static standing under three conditions: drop of the pelvis and flexion of the leg resulting from fixing in the hip abduction position using a hip orthosis (functional leg length discrepancy condition); drop of the pelvis by the orthosis, but no flexion of the leg due to a shoe lift (shoe lift condition); and normal bilateral standing condition. The shear elastic modulus of tensor fasciae latae was calculated using ultrasonic shear wave elastography.
RESULTS:
The shear elastic modulus was significantly lower in the functional leg length discrepancy condition than in the shoe lift and normal conditions (
CONCLUSIONS:
Using a shoe lift for the functional leg length discrepancy can result in a functional hip position that elongates tensor fasciae latae.
Keywords
Introduction
Total hip arthroplasty (THA) is a valuable procedure for the relief of chronic pain and functional disability and is effective in improving patients’ quality of life and physical function [1]. However, a third of patients after THA have a perceived leg length discrepancy (LLD) and have poorer functional outcomes [2, 3].
Previous studies have found that many patients with a perceived LLD after THA had a physically functional LLD rather than an anatomical LLD [2, 4]. The functional LLD after THA is caused by pelvic obliquity that results from soft tissue tightness in the structures that cross the hip joint [5]. Another previous study reported that most patients with a perceived LLD had both flexion and abduction contractures of the hip joint after THA [6]. In particular, the hip abduction contracture resulted from tight hip abductors that can tilt the pelvis downward on the affected side and lead to apparent lengthening of the ipsilateral leg. The relative lengthening of the affected leg compared to the contralateral leg can cause the perception of leg lengthening on the affected side and a compensatory postural adjustment such as a slightly flexed position of the ipsilateral hip and knee joint on standing.
The discomfort felt due to a functional LLD can be improved using a shoe lift under the unaffected leg. In a recent study of the use of shoe lifts with progressively thinner heights, the functional LLD of the patients who received early postoperative intervention with a shoe lift was significantly improved compared to the control group [7]. The use of shoe lifts that are adjusted to the height of the functional LLD could correct the flexed leg of the compensatory posture and help to passively elongate the length of the hip flexors and abductors.
One study reported that tensor fasciae latae (TFL) of the hip flexors and abductors could be quantitatively evaluated for elongation during stretching using ultrasonic shear wave elastography (SWE) [8]. SWE allows non-invasive and reliable measurement of muscle elasticity [9]. Previous studies confirmed a strong linear relationship between the shear elastic modulus measured by ultrasonic SWE and the referral setting to elongate the muscle length using the simultaneous tensile test [10] or passive ankle joint motion [11]. Therefore, ultrasonic SWE would be useful to measure changes in muscle length of the TFL. In the present study, a functional LLD was created artificially, and the effect of the functional LLD on TFL length and the effectiveness of a shoe lift for changing TFL length were investigated by ultrasound SWE.
Methods
Participants
Twenty-two healthy young adults were recruited at a university between May and December 2018. They had no history of hip pain and no limitation of hip or lumbar trunk motion. They all provided written informed consent prior to the measurement procedures. This study protocol was approved by the Ethics Review Board of the Yamagata Prefectural University of Health Sciences (#1806-08).
The sample size needed for one-way analysis of variance (ANOVA) with repeated measures [effect size
Standing postures from the coronal and sagittal planes in the three conditions. FLLD, drop of the right side of the pelvis and flexion of the right leg resulting from fixing the position in 20
Each participant wore a hip orthosis (Newport 3, Orthomerica Products, Orlando, FL, USA) with a range of motion adjustment on the right hip to artificially create a functional LLD and was then instructed to stand on two force plates. The support base was set at a width of 40 cm, considering the thigh cuff width of the hip orthosis. Trials under three bilateral standing conditions were then conducted as follows (Fig. 1): functional LLD condition, drop of the right side of the pelvis and knee flexion resulting from fixing the position in 20
Shear-wave elastography
The shear elastic modulus of the right TFL was performed in each of three standing conditions using SWE (Aixplorer, SuperSonic Imagine, Aix-en-Provence, France) with an ultrasound transducer (50-mm-long SL-15-4 linear ultrasound transducer). The SWE mode was selected, and both the SWE image and B-mode image were displayed using a dual screen configuration. The following default SWE settings for the system were used: standard SWE acoustic power, spatial smoothing of 5 and medium persistence. On SWE elastograms, the tissue elastic modulus was displayed in kilopascals (kPa) using a default chromatic scale with progression from blue to red, indicating low to high shear modulus (stiffness).
A typical example of shear elastic modulus measurement at the tensor fasciae latae (TFL). The lower image shows a B-mode ultrasound image, and the upper image shows a color-coded box. The mean Young’s modulus of the three regions of interest (Q-box: 5.0-mm-diameter), arranged longitudinally in the TFL, is calculated. The shear elastic modulus is obtained by dividing Young’s modulus by three.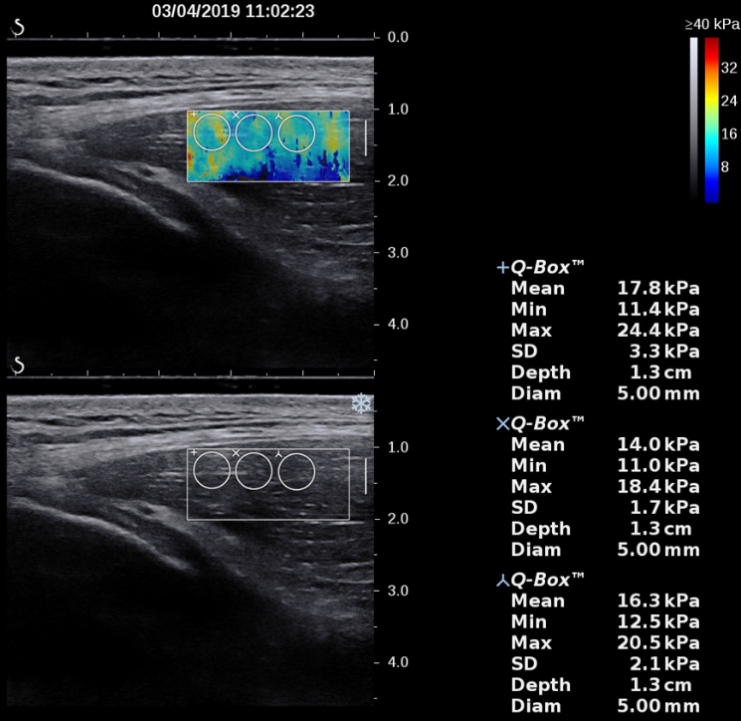
The measurement site was defined as the mid-point between the anterior iliac spine and the greater trochanter of the femur. The transducer was placed longitudinally on a hydrogel pad of 7
The Shapiro-Wilk test was used to assess whether the data were normally distributed. To assess the intra-rater reliability of the shear elastic modulus measurement, the intra-class correlation coefficient (1, 1) (ICC
Results
Twenty-two healthy young individuals participated in this study. Their characteristics are shown in Table 1. The angle of the dropped pelvis in the FLLD was 5.9
Participants’ characteristics (mean (SD))
Participants’ characteristics (mean (SD))
Reliability of shear elastic modulus measurements
ICC, intraclass correlation coefficient (1, 1); 95% CI, 95% confidence interval; FLLD, functional leg length discrepancy.
One-way repeated-measures ANOVA showed a significant main effect of the standing condition (
Bar chart showing the shear elastic modulus (kPa) of male and female participants in the post hoc test for standing condition. The shear elastic modulus of male and female participants is significantly lower in the FLLD group than in the NO and SL groups. 
The ICC
The present results show that TFL stiffness was lower in the FLLD condition than in the NO and SL conditions. In the FLLD condition, the hip joint on the downward side of the pelvic tilting was abducted because the adjustment on the hip orthosis was fixed at 20
The change in muscle stiffness during passive joint motion could be attributed to a change in muscle tension. Muscle tension forces with passive motion increase exponentially as the muscle is stretched to its maximal length [17]. The decrease in TFL stiffness in the FLLD condition could indicate passive shortening of TFL length, because the origin and insertion of the TFL come closer together with hip flexion. In contrast, the increase in TFL stiffness in the SL condition from the FLLD condition could indicate passive stretching of TFL length, because the origin and insertion of the TFL move further away from each other with hip extension. These findings would support the previous finding that the shear elastic modulus of the hip extension position was significantly higher than that of the neutral position [8]. However, this interpretation can be acceptable when the TFL activations are equal across the three standing conditions. It has been reported that leg muscle activation patterns varied with weight-bearing load [18, 19]. It can be assumed that the TFL activations could be maintained equally because the participants controlled the leg loadings by visual and auditory feedback across the three standing conditions. Therefore, using the shoe lift to correct the compensatory hip flexion position in the FLLD could lead the hip joint to a functional position which can stretch the TFL because it is thought that positioning a muscle close to its end of range will provide a greater effect on contraction [20].
In contrast, based on the classical kinesiological understanding, it is considered that change of the knee joint into extension passively shortens TFL length. Nevertheless, TFL stiffness increased in the SL condition, indicating that the TFL was stretched. A previous study reported that the stretching position with 90
These findings showing that the shoe lift for the FLLD condition can result in a functional hip position to improve TFL shortening could support the previous finding indicating the effectiveness of the heel lift in the treatment of FLLD after THA [7]. The shoe lift can be used not only as one of the compensatory approaches for reversible FLLD, but also as one of the remediation approaches to help improve the TFL shortening that causes pelvic obliquity and results in FLLD. Therefore, future studies are required to determine whether the posture change using the shoe lift for the FLLD is the functional position to improve TFL shortening in patients after THA. Clinical intervention studies should be conducted using SWE to investigate the effect of shoe lifts in the treatment of TFL shortening with FLLD after THA.
The present findings show that the effect of the shoe lift for stretching the TFL in FLLD might be useful in rehabilitation after THA. However, the findings also need to be interpreted in the context of the limitations of this study. First, the postural change between the FLLD and SL conditions was defined by extending the distance from the umbilicus to the medial malleolus while maintaining the angle of the dropped pelvis, but postural changes in lower limb joints were not evaluated quantitively. The postural changes in the SL condition could include other factors contributing to the ideal posture in addition to hip and knee extension. Second, the effect of shoe lifts for the FLLD should be applied only to the TFL muscle, because hip abductors include the anterior portion of gluteus maximus, gluteus medialis and gluteus minimus. These other hip abductors also need to be assessed in future studies. Third, lack of TFL activity assessment during the acquisition of SWE is a potential limitation of the study; it is needed to verify the assumption that the TFL activities can be maintained by controlling leg loading across the three conditions. Finally, the FLLD condition was simulated in each participant by fixing the hip angle at 20
Conclusions
The present study investigated the effect of an FLLD on TFL length and the effectiveness of the use of a shoe lift to correct the compensatory posture with an FLLD for the TFL elongation using ultrasound SWE. In the FLLD condition, the shear elastic modulus of the TFL decreased. With the shoe lift, the shear elastic modulus of the TFL was restored. These results suggest that using the shoe lift for FLLD can result in a functional hip position, stretching the TFL
Footnotes
Acknowledgments
This work was supported by JSPS KAKENHI Grant Number 18K17755 and the Yamagata Health Support Association.
Conflict of interest
The authors have no conflicts of interest associated with this study.