
Abstract
BACKGROUND:
Transcutaneous electrical nerve stimulation (TENS) is one of the most common methods for managing shoulder pain, and high voltage pulsed currents (HVPS) may be used for reducing pain. However, their immediate effects on resting pain and pain-free active range of shoulder motion (pfROM) in patients with subacromial pain syndrome (SAPS) have not been studied comparatively, yet.
OBJECTIVES:
The aim of this study was to compare the immediate effects of TENS, HVPS and placebo stimulation on shoulder resting pain and pfROM in patients with SAPS.
METHODS:
Randomized, placebo-controlled, double-blind, crossover study. One hundred and six patients with SAPS received placebo (predetermined 1st day application), TENS and HVPS with 1-day interval, in a random sequence. Before and after each application, resting pain and pfROM were evaluated by 0–10 cm visual analogue scales and a digital inclinometer, respectively.
RESULTS:
Intensity of pain decreased significantly after TENS, HVPS and placebo interventions (
CONCLUSION:
In patients with SAPS, both HVPS and TENS, but preferably HVPS can be used effectively to decrease pain and increase pfROM.
Keywords
Background
All non-traumatic, usually unilateral shoulder problems that cause pain, localized around the acromion, often worsening during or subsequent to lifting of the arm are defined as subacromial pain syndrome (SAPS) [1]. Bursitis, tendinosis calcarea, supraspinatus tendinopathy, partial tear of the rotator cuff, biceps tendinitis, or tendon cuff degeneration are different clinical and/or radiological names under this title [1].
SAPS, which is reported to be the most frequent cause of shoulder pain during physician office visits, gradually leads to functional loss and disability, hence, negatively affects quality of life [2, 3]. It is preferably treated by conservative approaches such as rest, nonsteroidal anti-inflammatory drugs, corticosteroid injections, extracorporeal shock wave therapy, exercise therapy, mobilizations, massage, laser therapy, hot-cold agents, acupuncture, bandaging, ultrasound (US) therapy, electrical stimulation, magnetic field therapy and combined methods [1, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12]. In a systematic review by Haik et al. [13], which investigated physical therapy modalities for SAPS on pain, function/disability or range of motion, it was reported that there was high level of evidence regarding the lack of beneficial effects of physical resources such as low-level laser, US and pulsed electromagnetic field (PEMF) in the treatment of SAPS, and there was limited evidence for microwave diathermy and TENS.
Transcutaneous electrical stimulation (TENS) and high voltage pulsed current/stimulation (HVPS) are both electrophysical agents which can be used for pain relief in musculoskeletal conditions. Standard TENS devices usually deliver biphasic pulsed currents with a pulse duration between 50
Approximately 1/3 of physiotherapists use pain-focused electrotherapy within their treatment programs for patients with subacromial impingement syndrome [11]. Johansson et al. investigated clinicians’ beliefs in interventions for subacromial pain and reported that the majority of physiotherapists (68%) has trust in TENS, although there is no available evidence for its efficacy in patients with subacromial pain [8]. The lack of evidence for the efficacy of TENS as well as other pain-focused electrotherapy agents may be due to the use of inadequate research designs and methodological weaknesses of the studies [6]. In addition, there has been little experimental work on the effects of HVPS on pain relief in the literature [14, 15] and no study for its efficacy in SAPS.
According to the Philadelphia Panel regarding rehabilitation interventions for shoulder pain, there is an urgent need for prospective randomized controlled trials, which use rigorous methods such as use of an appropriate placebo and double-blind procedure, adequate randomization, homogeneous sample of patients and adequate sample size [6]. Therefore, the aim of this study is to investigate and compare the immediate effects of single session applications of conventional TENS and HVPS on pain and pain-free range of active shoulder motions (pfROMs) in patients with SAPS, using a placebo-controlled, double-blind, randomized method in crossover design.
Methods
Study design and setting
This study was carried out at a private hospital in Fethiye, Muğla, between November 2015 and January 2017. The study was performed in accordance with the ethical standards in the 1964 Declaration of Helsinki. The Scientific Research Ethical Board of Muğla Sıtkı Koçman University approved this study (Protocol no: 161, Decision no. 145, Date: 22.10.2015). This double-blind, randomized, placebo-controlled crossover trial is registered on ClinicalTrials.gov (NCT03588143).
Participants
The participants in this study were outpatients of a physical therapy and rehabilitation clinic. They were diagnosed with SAPS (Neer stage 1–2) by a physician according to the Guideline of Dutch Orthopedic Association [1, 18]. Within the study calendar, among 164 patients diagnosed with SAPS, 106 met the inclusion criteria, signed the informed consent, andwere recruited (Fig. 1). The inclusion criteria were: (1) being 18–65 years-old; (2) having pain with active shoulder movements; (3) being diagnosed with SAPS for 1–10 weeks; (4) positive Hawkins-Kennedy and painful arc tests; (5) infraspinatus weakness; and (6) a negative drop-arm test for patients with partial rotator cuff tear [10, 11]. The exclusion criteria were: (1) radiologically confirmed malignity or acromial/acromioclavicular arthritis; (2) history of fracture or surgery in the affected shoulder-arm complex; (3) clinically confirmed polyarthritis, rheumatoid arthritis, fibromyalgia, adhesive capsulitis or osteoarthritis of the glenohumeral joint or subacromial region; (4) cervical or thoracic spinal problems; (5) neurological problems which may affect upper extremity movements or pain perception (stroke, peripheral neuropathy, brachial plexus lesion, etc.); (6) using anti-inflammatory, analgesic, or myorelaxant medicine during the study; (7) body mass index
Flow diagram of the study.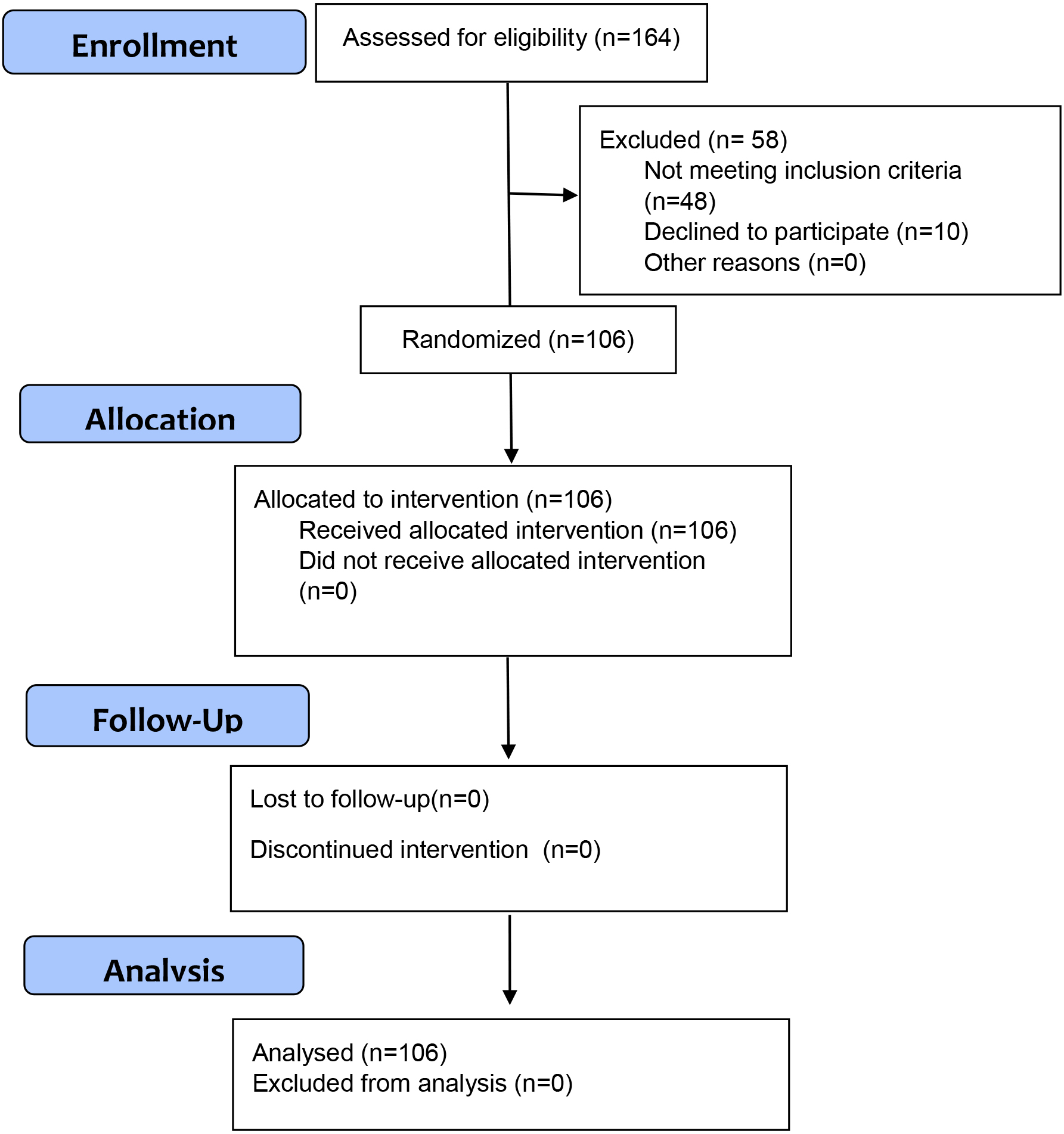
Physical (age, gender, height, weight, body mass index values) and sociodemographic (occupation, educational level, marital status) characteristics of the participants, as well as the affected shoulder (right/left) and time since diagnosis of SAPS (week) were recorded.
Outcome measures of this study were intensity of resting pain and pfROMs. The participants were asked to mark their resting pain intensity on a 0–10 cm visual analogue scale, where 0 cm indicated no pain and 10 cm indicated unbearable pain. The distance of the marked point from zero point was recorded as the intensity of pain.
Pain-free ranges of active shoulder flexion, abduction, internal and external rotation were measured by a digital inclinometer (Baseline Digital Inclinometer, 2008 New York-USA), which was calibrated on a flat surface before each measurement. Pain-free active shoulder internal and external rotations were measured in supine-hook lying position, where the shoulder was in 90
All evaluations were performed before and just after each modality, which were applied in three consecutive days, with 24 hours’ washout period. All of the measurements were performed by a physiotherapist blinded to the modalities applied (placebo/TENS/HVPS).
In this crossover study, closed opaque envelopes including numbers which indicate the interventions, were used for randomizing the order of interventions. However, at the first day, all subjects received placebo intervention in order to prevent them to distinguish the feelings of current and placebo applications. The subjects only knew the number written inside of the closed envelope they chose, and only the physiotherapist who applied the interventions knew the indications of the numbers. Therefore, subject blinding was assured. All pfROM assessments were carried out by another physiotherapist who was kept blind to the interventions applied. No other interventions (medication, physiotherapy, advice, etc) were given to the subjects till the end of three-day trial.
All interventions (placebo, TENS and HVPS) were applied by the same combined electrotherapy device (Intelect Advanced, Model 2762CC, Chattanooga Group-USA) and the electrodes with same characteristics (5
The subjects were sitting on an armchair with their elbows flexed at about 90
Comparison of within-intervention differences of visual analogue scale scores (cm) and pfROM values (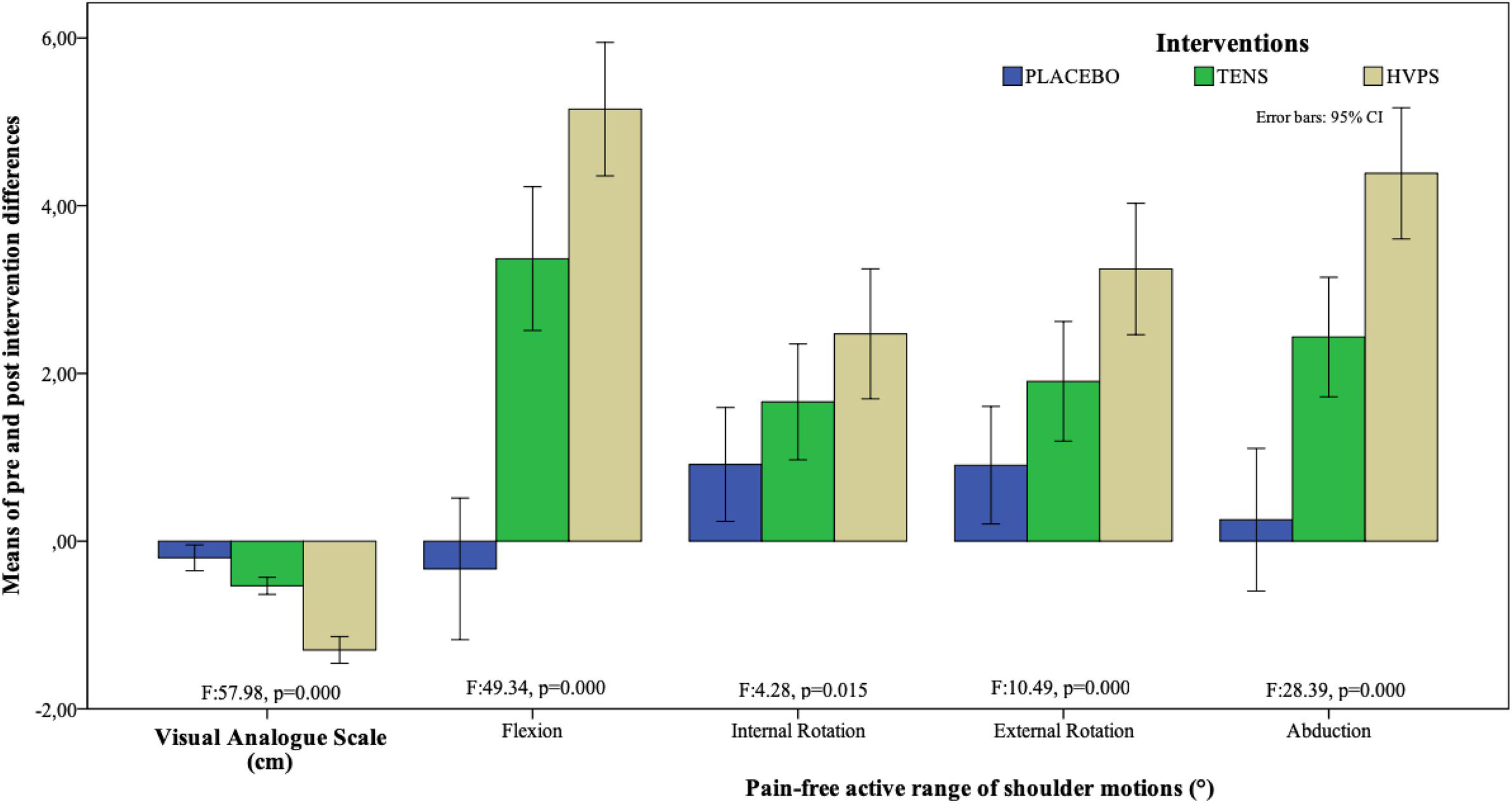
TENS was applied with asymmetrical biphasic current at 65
The sample size was calculated by G-Power statistical software package version 3.1.9.3 for Mac (
Physical and sociodemographic characteristics (
106)
Physical and sociodemographic characteristics (
Visual analogue scale scores (cm) before and after interventions
TENS: Transcutaneous electrical nerve stimulation, HVPS: High voltage pulsed currents cm: centimeter, SD: Standard deviation,
PfROM values (
PfROM: Pain-free active range of shoulder motion, TENS: Transcutaneous electrical nerve stimulation, HVPS: High voltage pulsed currents, SD: Standard deviation,
The study sample consisted of 61 women (57.5%) and 45 men (42.5%) with SAPS, who were 24–65 years-old. Their physical and sociodemographic characteristics are presented in Table 1. In 94 (88.7%) participants, the right extremity was the dominant extremity, and only 65 (61.3%) of them had suffered the injury to that extremity. Mean time since diagnosis was 1.45
There were no significant baseline differences of pre-intervention values of pain intensity and pfROM (
All PfROMs significantly improved after TENS (
Discussion
Both TENS and HVPS are commonly used methods in orthopedic rehabilitation with the aim of relieving pain. However, the effectiveness of HVPS on SAPS has not been reported previously, and this is the first randomized and placebo-controlled study to compare the effects of TENS and HVPS on pain and pfROM in patients with SAPS.
The findings reveal that both interventions are effective in decreasing rest pain and increasing pfROMs, and HVPS is more effective than TENS and placebo applications on the outcomes.
Both conventional TENS and HVPS have been proposed to promote pain relief through spinal gating mechanism by stimulating the large afferent neurons (A
Although there were significant differences among the interventions, placebo application also caused a decrease in pain. This finding may indicate that success of TENS and HVPS depends not only on physiological but also their placebo effects. After placebo intervention, only pain free internal and external rotation ranges increased significantly. This may be due to the biomechanical advantage of the measurement positions used for rotations. Supine position with 90
Literature findings related with TENS in shoulder pain generally report its cumulative effects at the end of several sessions, and in comparison with other electrophysical agents such as US, interferential therapy and radiofrequency currents, as well as with placebo intervention [22, 23, 24, 25, 26]. However, there is lack of knowledge about the immediate effects of TENS on shoulder pain, and to our knowledge, the only relevant research is the study of Başkurt et al. [27]. In that study, the authors have found that TENS (100 Hz frequency, 0.1 ms pulse duration, symmetrical biphasic waveform, tolerable intensity) was effective in decreasing pain in stage I shoulder impingement syndrome. This finding supports the results of the present study, which indicate that the immediate effect of TENS on reduction of pain in patients with SAPS was significant.
Lack of randomization in the sequence of pfROM measurements stands as a limitation for this study. In addition, only immediate effects of interventions have been investigated, and no conclusions at the moment can be drawn about their cumulative or long-term effects. In addition, only time since SAPS diagnosis was recorded, but information about the duration of SAPS symptoms in this sample is lacking. Therefore, it is difficult to identify if the study sample had an acute or chronic condition. This point may be a limitation for generalizability of the findings.
Conclusion
The main strength of this study stands on its rigorous methodology including use of an appropriate placebo and double-blind procedure, adequate randomization, homogeneous sample of patients and adequate sample size. Since the guideline for diagnosis and treatment of SAPS recommends movement and exercises which specifically focus on rotator cuff and scapular stabilizers within the pain threshold [1], inclusion of TENS or preferably HVPS within treatment sessions prior to these exercises, may contribute to desirable outcomes.
Footnotes
Acknowledgments
This research (Project Grant Number 16/044, title “Acute Effects of Transcutaneous Electrical Nerve Stimulation and High Voltage Pulsed Stimulation on Subacromial Pain and Shoulder Movements”) was supported by the Muğla Sıtkı Koçman University Research Projects Coordination Office. The authors thank Levent Eker (MD) for helping to determine the sample size; Erhan Çetin (MD) for referring eligible patients to the study; Sera Kopuz (PT) for her valuable help in evaluating the patients, and the Private Lokman Hekim Hospital staff for their support in arranging the workplace conditions.
Conflict of interest
Each author certifies that he or she has no commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Funding
This paper is a part of the thesis by Furkan Bilek, which has been granted by the Muğla Sıtkı Koçman University Research Projects Coordination Office (Project Grant Number: 16/044, title “Acute Effects of Transcutaneous Electrical Nerve Stimulation and High Voltage Pulsed Stimulation on Subacromial Pain and Shoulder Movements”).