
Abstract
BACKGROUND AND OBJECTIVE:
Morel-Lavallée Lesion (MLL) of the knee is an uncommon cause of knee swelling usually due to high-energy impact or in patients on anticoagulation. MLL of the knee due to low-energy non-athletic associated trauma in patients without antithrombotic therapy is rare. Early diagnosis can be achieved using point-of-care ultrasound.
CASE REPORT:
A 60-year-old female who was previously well was referred to our center for a persistently swollen left knee 2 months after a fall while on a flight of stairs. A point-of-care ultrasound identified a possible MLL of the knee. This was subsequently confirmed on magnetic resonance imaging (MRI). The lesion resolved with ultrasound-guided therapeutic aspiration.
CONCLUSION:
MLL of the knee should be a differential diagnosis of traumatic knee swelling, even in low-energy trauma and in patients without bleeding diatheses. Ultrasound is a readily available and rapid modality that can aid both in the diagnosis and management of such lesions.
Introduction
A Morel-Lavallée Lesion (MLL), first described in 1863 [1], is a rare closed soft tissue degloving injury sustained over bony regions, classically over the hip or thighs. The hypodermis is separated from the underlying fascia, disrupting perforating vascular and lymphatic structures, allowing fluid to accumulate in the potential space between the tissue layers [2].
MLLs are usually associated with high-energy trauma seen in road traffic accidents and contact sports, due to a shearing or crush injury [2, 3]. MLLs of the knee are unusual, and have been described in the context of motorcycle accidents in case reports [4, 5]. They have also been reported in athletes sustaining high-energy impact such as football players [6]. However, low-energy trauma in non-athletes resulting in MLL of the knee are rare in the literature. A case report describe an elderly woman, on aspirin and prophylactic enoxaparin sodium who developed an MLL of the knee 10 days after falling in a hospital bathroom [7]. Similarly, Hogerzeil et al. report an overweight patient on anticoagulation medication (acetylsalicylic acid and clopidogrel), who presented with an MLL of the proximal tibia 2 months following a fall in his backyard [8]. However, MLL of the knee has not been well-described in patients experiencing low-energy trauma who were not on anticoagulation.
Early diagnosis is crucial to differentiate the cause of traumatic knee swellings. Such lesions are often evaluated with MRI as the gold standard, but the use of point-of-care ultrasound can potentially be highly accurate as well, while providing a low-cost option [9]. The following case illustrates a rare presentation of MLL of the knee in a non-athlete after low-energy trauma, which was diagnosed and managed early with the use of point-of-care ultrasound.
Case report
A 60-year-old woman fell down while on a flight of stairs and presented with a persistently swollen left knee 2 months after her injury (Fig. 1). She had no significant medical history and was not on any antiplatelets or anti-coagulants. She was initially treated for haemarthrosis with splinting by another doctor, but the knee swelling did not improve. On examination, her left knee was slightly tender and a large fluctuant mass over the patella was observed with no increased warmth. She was unable to fully flex her knee due to the swelling. Ligament and meniscal tests were negative. Laboratory tests did not reveal any evidence of bleeding diatheses or infection, and a plain radiograph of the knee was normal.
Left knee swelling.
A point-of-care ultrasound identified an effusion superficial to the knee joint and deep to hypodermis, with lateral and proximal extension (Fig. 2A and B). The characteristic location raised the suspicion of an MLL of the knee. There was no vascularity demonstrated on sonography. A bedside knee aspiration removed 55 mls of bloody fluid with no crystals. No organisms were seen on the gram stain and cultures were negative. A subsequent magnetic resonance imaging (MRI) revealed a hyperintense lipogenous effusion between the subcutaneous fat and patella with lateral extension on fat-saturated intermediate-weighted images (Fig. 2C and D), confirming the diagnosis of an MLL of the knee.
Morel-Lavallée Lesion of the left knee evaluated with ultrasound (A, B) and magnetic resonance imaging (MRI) (C, D). A, Longitudinal sonographic axis shows an anechoic fluid collection (asterisk), located anterior to the patella (arrowheads), and tracking proximally towards the thigh. B, Short sonographic axis shows an anechoic fluid collection (asterisk), located anterior to the patella (arrowheads), and tracking laterally. C–D, Intermediate weighted fat-saturated MRI of the knee on axial and sagittal planes show a hyperintense effusion between the subcutaneous fat and patella with lateral and proximal extension.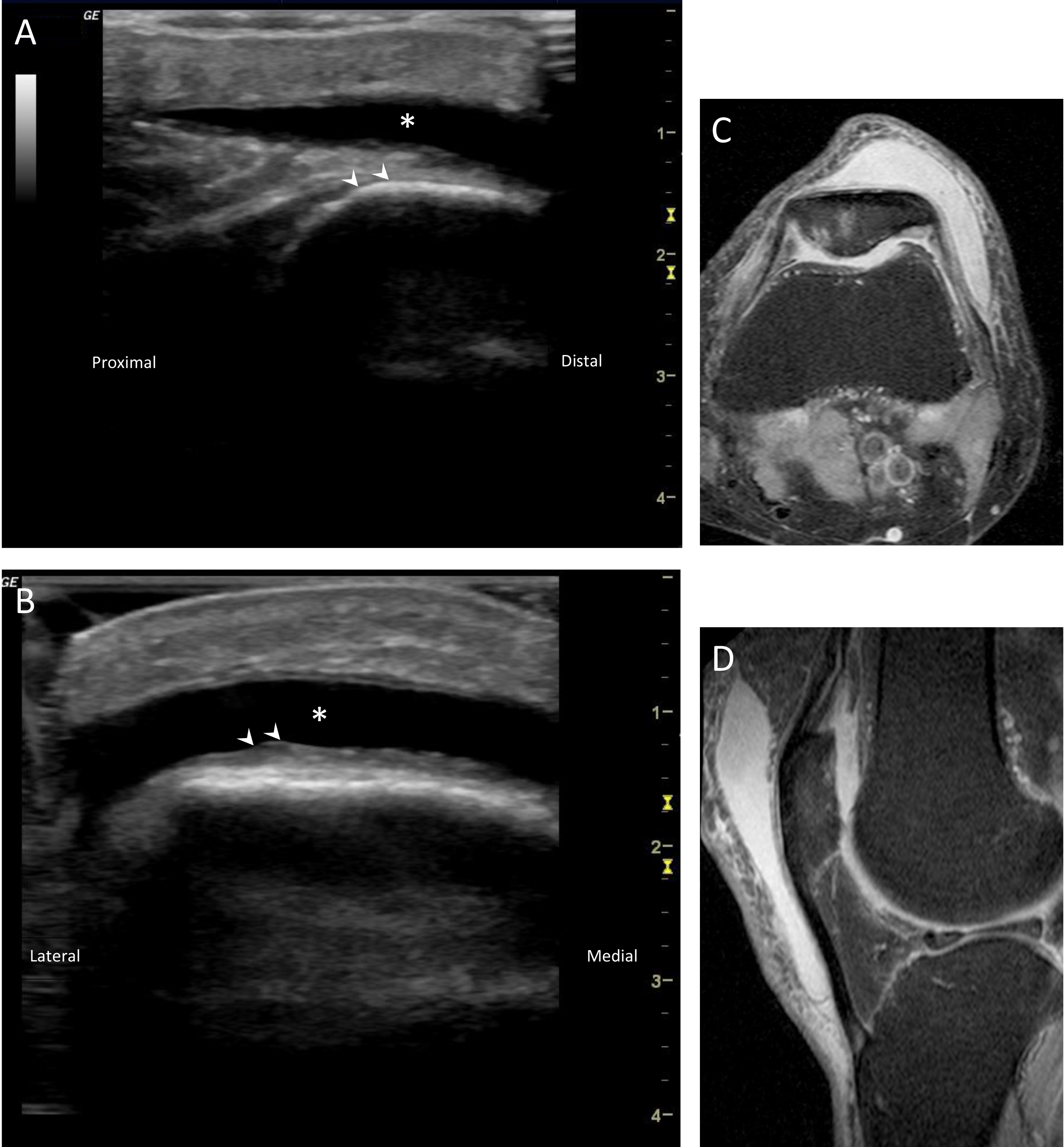
The patient underwent a second therapeutic aspiration with ultrasound guidance, followed by compressive bandaging with regular clinical visits to observe for complications. There was no further recurrence at 6 months follow-up.
The incidence of MLL of the knee is unknown, and the diagnosis is often delayed or missed due to the rarity of the condition in low-energy, non-athletic-related trauma [7]. Moreover, this patient was not taking any anticoagulation, which has previously been linked with MLL of the knee in low-energy injuries [7, 8]. This case report is hence unique in that it demonstrates that MLL of the knee can result from low-energy falls, likely due to a shearing mechanism, which can occur even without any underlying bleeding diatheses.
The onset of swelling in MLLs is typically within hours or days after trauma [2]. In addition to direct trauma over the involved area, careful history taking often reveals gradual fluid accumulation and progressive limitation in knee flexion [6]. However, clinical findings in an MLL such as tenderness, limited range of motion and fluctuance around the knee are often non-specific and may mimic haemarthrosis secondary to a traumatic intra-articular lesion. Ultrasound is a readily available modality that can be used for rapid diagnosis and serial monitoring. These advantages have led several authors to consider ultrasound as an reliable imaging modality for the evaluation of posttraumatic fluid collections [9, 10, 11, 12, 13]. Common differential diagnoses that should be excluded on ultrasound include traumatic hemarthrosis, subcutaneous hematoma and prepatellar bursitis [12]. On sonography, hemarthrosis is usually limited to the suprapatellar recess, while a subcutaneous hematoma is located more superficially to the hypodermis [13]. Unlike MLL of the knee, prepatellar bursitis do not extend medially or laterally beyond the mid-coronal plane nor towards the mid-thigh, which are beyond the anatomical borders of the prepatellar bursa [6]. Fluid aspiration is often necessary to exclude septic bursitis in the latter. It is also important to distinguish prepatellar bursitis from an MLL, given that the latter do not respond significantly to steroid injections due to the lack of a synovial lining, unlike the former [14].
If the diagnosis is still in doubt, MRI of the knee can be obtained for further characterization of superficial knee effusions [13, 14]. Fat-saturated images allow the classification of intralesional hyperintense foci as lipogenous in nature, identifying the fluid collection as an MLL [13]. Several MRI features can also be used to distinguish MLL of the knee from various differential diagnoses. Intra-articular injuries resulting in hemarthrosis can be clearly demonstrated on MRI. Compared to MLL, subcutaneous hematomas have a relatively higher internal fluid density with fluid-fluid layers in the setting of clot lysis. Prepatellar bursitis are seen as fluid lesions with heterogeneous signal intensity between the subcutaneous tissue, with T2 shortening on gradient-echo (GRE) images in hemorrhagic lesions [13, 14]. In this patient, ultrasound was sufficient to make the provisional diagnosis of an MLL of the knee, which was further confirmed on MRI. Ultrasound was also critical in the management of the patient, by ensuring accurate and complete aspiration of the lesion under ultrasound guidance.
Appropriate management of uncomplicated MLLs remains controversial [2, 3]. Early recognition with the aid of imaging is essential to avoid the complications of an expanding or chronic MLL, which include bacterial superinfection or overlying skin necrosis [15]. Subsequent treatment often depends on the lesion size, as larger lesions are less likely to resolve spontaneously [3]. Compressive bandaging can be effective in relatively small variants of MLL of the knee. This has a reported success rate of 52%, with a mean time to symptom resolution of 10 days [6]. If symptoms do not resolve or are disabling, percutaneous sterile aspiration can be considered if the overlying skin is viable [2, 15]. Surgical drainage and debridement can also be considered in large or chronic lesions [3].
Conclusion
An MLL of the knee should be considered as a differential diagnosis in patients presenting with a traumatic knee swelling. Ultrasound is a readily available modality that can be used to rapidly evaluate the swollen knee. Early management is essential to reduce the risk of complications.
Footnotes
Acknowledgments
We would like to express our gratitude to the patient in this case report.
Conflict of interest
None to report.